
Diagnostic Value of Sialic Acid in Pleural Effusion
2010-09-16 03:59:18BANSALTANDONKHARB
中國肺癌雜志 2010年4期
A BANSAL, S TANDON, S KHARB
Department of Biochemistry and Tuberculosis and Respiratory Medicine, Pt B D Sharma University of Health Sciences, Rohtak, India
Abstract The present study was conducted in 30 patients of malignant pleural effusion and 30 patients of non malignant pleural effusion. Pleural fluid and blood samples were taken at the time of admission, before starting any treatment. Sialic acid levels were estimated in serum and pleural fluid by Warren’s TBA method. In the present study, serum sialic acid levels were higher in group II as compared to group I. In the present study, pleural fluid sialic acid levels and PF/S ratio was higher in malignant pleural effusion (though difference was not statistically significant). Smokers in group II had higher serum sialic acid as compared to group 1 (P<0.05). The sensitivity and specificity of pleural fluid/serum sialic acid ratio with cut off value of 0.7 were 76.67%and 20% respectively, while taking the cut off value of 70 mg/dL for pleural fluid sialic acid in malignant pleural effusions, the sensitivity was 63.33%, specificity 60% and positive predictive value 46.34%. These findings indicate that determination of sialic acid levels in pleural fluid has diagnostic value as a cheap, simple and reliable marker for malignant pleural effusion.
Key words Lung neoplasms; Thoracic surgical procedures; Lymphatic metastasis; Treatment outcome
Introduction
Malignant disease involving pleura is the second leading cause of exudative pleural effusions after parapneumonic effusions. It is one of the most common diagnostic problems requiring detailed investigation, encountered by specialist[1]. An increasing number of biochemical parameters have been reported to have diagnostic value in malignant pleural effusions[2-4]. Sialic acid levels have been found to be elevated in neoplastic cells derived from lung, breast, stomach, and colon, and ovary, prostate and liver tumors[5]. Recently sialic acid has been reported to have a diagnostic value[4]. Hence, the present study is designed to measure sialic acid in pleural effusion and serum samples of patients in order to differentiate between malignant and nonmalignant diseases.
Materials and methods
The present study was conducted in sixty patients attending Outpatient Department of Tuberculosis and Respiratory Medicine in collaboration with Department of Biochemistry,Pt BDS PGIMS, Rohtak, India. They were subdivided into two groups of thirty patients each: Group I (patients with pleural effusion proved malignant by pleural biopsy) and Group II(controls with nonmalignant pleural effusion). Inclusion criteria: sputum negative for AFB (at least on three occasions), confirmed malignant by pleural biopsy, exudative pleural effusion.All the cases were subjected to detailed clinical history, thorough clinical examination and routine investigations. Pleural fluid and blood samples were taken at the time of admission,before starting any treatment. Sialic acid levels were estimated in serum and pleural fluid by Warren’s TBA method[6]. Data so obtained was analyzed statistically; student’st-test was applied and regression analysis was carried out.
Observations
The clinical characteristics of the two groups are given in Tab 1. In group I, there were 14 patients who were smokers,while in group II there were 21 smokers. In group I, 4 out of 30 patients were cases of benign pleural effusion, 18 had tubercular etiology, 10 had pneumonitis and 2 cases were with chylothorax. In group II, 5 had malignant effusion, 25 had lung cancer, and 1 had mediastinal neoplasia.
Pleural effusion and serum sialic acid levels were higher in group II as compared to group I, though the difference was not statistically significant (Tab 2). PF/S ratio was higher in group II as compared to group I though difference was not statistically significant. Also, smokers had high pleural fluid and serum sialic acid levels and PF/S ratio as compared to nonsmokers.Smoker in groups II had higher serum sialic acid as compared to group I (P<0.05).
Taking cut off value of pleural fluid sialic acid as 65 mg/dL,in malignant pleural effusion, sensitivity was 63.33%, specificity 60% and positive predictive value 46.34% (Tab 3). Taking cut off value of 0.7 for PF/S sialic acid ratio, sensitivity was76.67%, specificity 20%, and positive predictive value 48.94%in malignant pleural effusion.
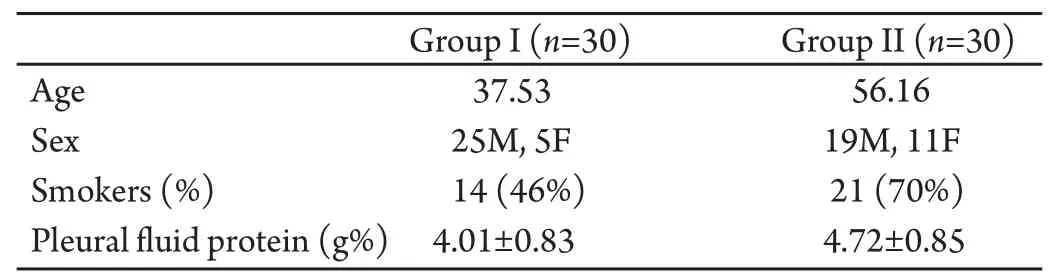
Tab 1 Clinical characteristics

Tab 2 Sialic acid levels in the two groups (Mean±SD, mg/dL)

Tab 3 Discriminative value of sialic acid level and PF/S ratio in both groups (%)
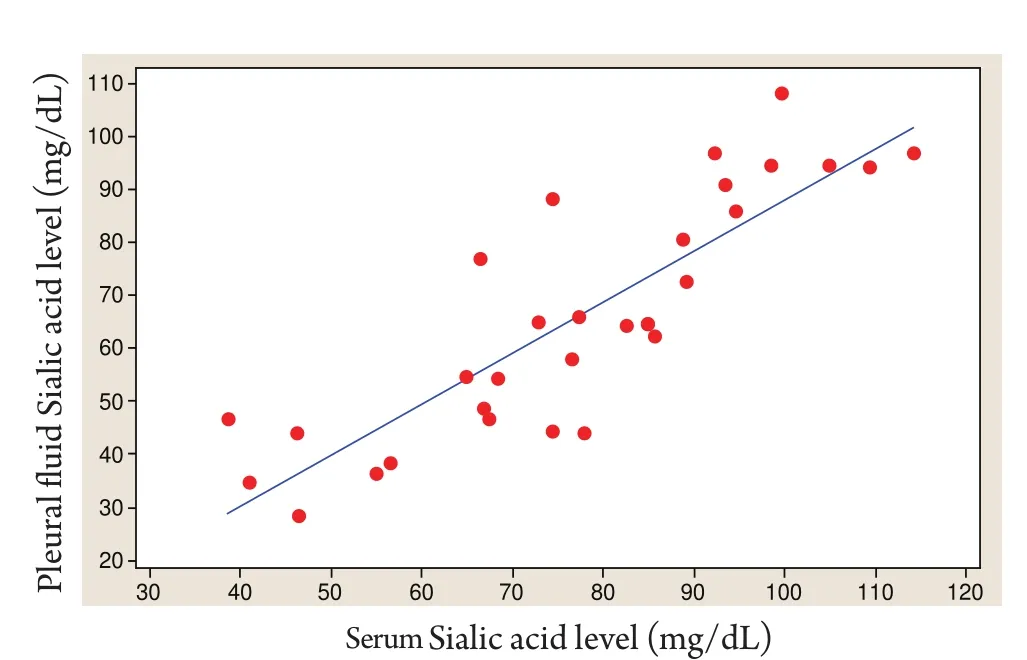
Fig 1 Correlation between PF and Serum Sialic acid in benign disease
A positive correlation was observed between rise in sialic acid in pleural fluid and serum Sialic acid levels in group I (Fig1)and no significant correlation could be observed in group II.
Discussion
In the present study, serum sialic acid levels were higher in group II as compared to group I. Changes in sialic acid content of patient’s sera have been reported to ref l ect growth processes of benign and malignant character[7]. Raised serum sialic acid levels have been reported in various cancers[5]. Our findings are in agreement with those reported by Krolikowskyet al[8]Bektemuret al[9]have reported high serum sialic acid levels in malignant pleural effusions though difference was not statistically significant. They also observed high pleural fluid sialic acid levels and PF/S ratio.
In the present study, pleural fluid sialic acid levels and PF/S ratio was higher in malignant pleural effusion (though difference was not statistically significant). Smokers in group II had higher serum sialic acid as compared to group I (P<0.05).
These findings are in agreement with those reported in literature[8-11]. In the present study, the cases selected were of malignant pleural effusion in stage 4, so no correlation was done with stage of disease since our aim was to analyze sialic acid for differentiating malignant from nonmalignant pleural effusion.
In differential diagnosis of exudative pleural effusions, cytology is the most sensitive method. Since cytology findings are positive in half of such fluids, combined use of reliable tumor marker and cytology is a logical approach. Elevated concentration of sialic acid could be due to implants of malignant cells on pleura producing effusion as well as diffusion by pleural capillaries into pleural fluid.
On comparing sialic acid levels in serum and pleural fluid,33.33% of cases of malignant pleural effusions had raised pleural fluid sialic acid (>70 mg/dL) as compared to serum levels which were in the normal range. This could be either due to production and gradual absorption of sialic acid in diseased area or elevation of both serum and pleural fluid levels,but sialic acid disappears more slowly from pleural fluid.
Reports comparing sialic acid levels in serum in various histopathological types have found raised levels in squamous cell carcinoma and small cell carcinoma[12], but, studies in pleural fluid are lacking. In the present study no specific correlation of sialic acid with any particular histopathological type could be observed.
Smokers had higher pleural fluid sialic acid levels in malignant pleural effusion as compared to non smokers (Tab 2,P>0.05). While in benign pleural effusion pleural fluid sialic acid levels were higher in non smokers (Tab 2,P>0.05). PF/S ratio was higher in smokers than in non smokers in malignant pleural effusion and lower in smokers in benign pleural effusions (Tab 2,P<0.05,P>0.05, respectively).
Serum sialic acid levels have been reported to be increased in smokers and alcoholics since smoking induces tissue inf l ammation and is a known carcinogen[13]. Hence elevated sialic acid levels in pleural fluid could be attributed to smoking and this could possibly a secondary process to malignancy that needs to be established by further studies. Since the studies have reported that total sialic acid levels remain unchanged following one year of smoking cessation[13,14].
In the present study, a significant positive correlation was observed between pleural fluid and serum sialic serum sialic acid levels in benign pleural effusion (Fig 1). A positive correlation was also observed between pleural fluid and serum sialic acid levels in malignant pleural effusion though difference was not statistically significant. Bektemur et al had also observed no significant correlation between pleural fluid to serum lipid bound sialic acid ratios in benign and malignant groups[9].
Taking cut off value of 70 for pleural fluid sialic acid in malignant pleural effusions, sensitivity was 63.33%, specificity 60% and positive predictive value 46.34% (Tab 3).
Taking cut off values of >0.7 for PF/S ratio, sensitivity was 76.67%, specificity 20% and positive predictive value 48.94%(Tab 2). These findings are in agreement with those reported in literature[10]. Thus, pleural fluid sialic acid in malignant pleural effusion along with PF/S ratio have good sensitivity and positive predictive value and can prove to be a reliable marker in differentiating benign and malignant pleural effusion.
- 中國肺癌雜志的其它文章
- 重組人血管內(nèi)皮抑制素聯(lián)合放射治療對lewis肺 癌小鼠的作用
- 非小細(xì)胞肺癌中EGFR基 因狀態(tài)的檢測對EGFR-TKIs療 效的預(yù)測價(jià)值
- A Review of Epidermal Growth Factor Receptor/HER2 Inhibitors in the Treatment of Patients with Non-Small-Cell Lung Cancer
- IIIa期 非小細(xì)胞肺癌術(shù)后輔助治療的臨床應(yīng)用
- 《中國肺癌雜志》網(wǎng)站全文對中國抗癌協(xié)會(huì)肺癌專業(yè)委員會(huì)會(huì)員免費(fèi)開放
- Tracheal Carinal Reconstruction and Bronchovasculoplasty in Central Type Bronchogenic Carcinoma