
The “PAWPER-on-a-page”: Increasing global access to a low-cost weight estimation system
2019-02-23 02:02:16MikeWellsLaraNicoleGoldstein
Mike Wells, Lara Nicole Goldstein
Division of Emergency Medicine, Faculty of Health Sciences, University of the Witwatersrand, Parktown, Johannesburg,South Africa
KEY WORDS: PAWPER tape; Weight estimation; Paediatric emergency care
INTRODUCTION
Appropriate weight estimation during the management of paediatric emergencies is an essential element of the resuscitation process.[1]This is because weight is required to quantify drug and fluid doses in children, and an accurate, measured weight is seldom obtainable for this purpose during emergency care.[2]Since inaccurate weight estimations frequently lead to medication errors,with a resultant risk of patient harm, it is essential that weight should be estimated as accurately as possible,notwithstanding the critical nature of the situation.[3]The PAWPER tape (Paediatric Advanced Weight Prediction in the Emergency Room tape) is one of the three most accurate paediatric weight estimation systems in the world (Figure 1).[4]Along with the Mercy method and parental estimates, it has outperformed all other, older methods of weight estimation.[5]The accuracy of a weight estimate is important during paediatric emergencies, as the safety and effectiveness of calculated drug doses are ultimately dependent on this weight estimation.[6]The PAWPER XL tape (extra-long and extra-large) is the newest version of the PAWPER tape which has an expanded ability to estimate weight in taller children (up to 180 cm) and severely obese children.[5]
The PAWPER tape was originally designed and intended to be an low-priced alternative to the very expensive Broselow tape (hence the pun on “pauper”).[7]However, since the PAWPER tape and PAWPER XL tape are produced on a non-commercial, not-for-pro fit basis, it is dif ficult to disseminate them both locally and internationally,as the cost of distribution far exceeds the costs of producing the actual tapes. This impedes their clinical use as well as further research and development on the tapes in different populations.
The “PAWPER-on-a-page” concept was conceived as a way to make the PAWPER tape (and the PAWPER XL tape) available to any person anywhere in the world who has access to the internet, a printer and the basic stationery required to assemble the tapes. The“PAWPER-on-a-page” is a PDF digital image file that can be downloaded free-of-charge and then printed in black and white on a single A4 page. The “PAWPER XL-on-a-page” tape can similarly be downloaded and printed in colour on an A3 page (see Figure 2). It is clear that the accuracy of the “PAWPER-on-a-page” and“PAWPER XL-on-a-page” would depend on the user being able to print it exactly to scale and then assemble it with precision. Mistakes in printing or assembly could result in inaccurate weight estimations, erroneous drug doses and potential patient harm. This needed to be tested to ensure that users could create safe versions of the PAWPER tapes for clinical and research purposes.
Importance and relevance
This study was important because it addressed the problem of the restricted global availability of the PAWPER tape. This is relevant, because accurate weight estimation plays an important role in paediatric patient safety during emergency care. The PAWPER-on-a-page,a potential solution to increasing access to the PAWPER tape, needed to be formally evaluated amongst potential users.
Research question
The main research question of this study was to establish whether the “PAWPER-on-a-page” and the“PAWPER XL-on-a-page” system could be accurately,easily, affordably and acceptably fabricated by healthcare providers. This was in order to establish whether this system would be a safe and practical solution to increase global access to the PAWPER system for clinical use.
The specific objectives of this study were: to determine whether downloaded PDF images could be accurately printed on home printers as well as
What is the PAWPER tape?
It is a dual length- and habitus-based method used to estimate the weight of children during medical emergencies.
Why is the PAWPER tape more accurate than other methods of weight estimation?
It makes use of two variables to produce an estimate of weight: body length and a visual assessment of body habitus.
What are the habitus scores?
The habitus scores quantify the child's "thinness" or "fatness".
HS1 represent a very thin child, HS3 an "average" child, HS5 a very overweight child and HS7 a severely obese child.
Is the PAWPER tape easy to use?
Yes. The estimated weight can be read directly off the tape and no calculations are required. It was designed to be used during emergencies.
What is the PAWPER XL tape?
It is the updated version of the original tape - it is longer (180 cm vs.153 cm), has an improved capacity to estimate weight in obese and severely obese children (7 habitus score categories vs. 5 categories)and is printed in color. It also provides an estimation of ideal body weight for obese children.
How are the tapes used to estimate weight?
Both tapes are used in much the same way, in three steps:
Step 1 the tape is used to measure the child's length.
Step 2 the user makes an assessment of the child's habitus with either a gestalt visual assessment or a reference image-guided assessment.
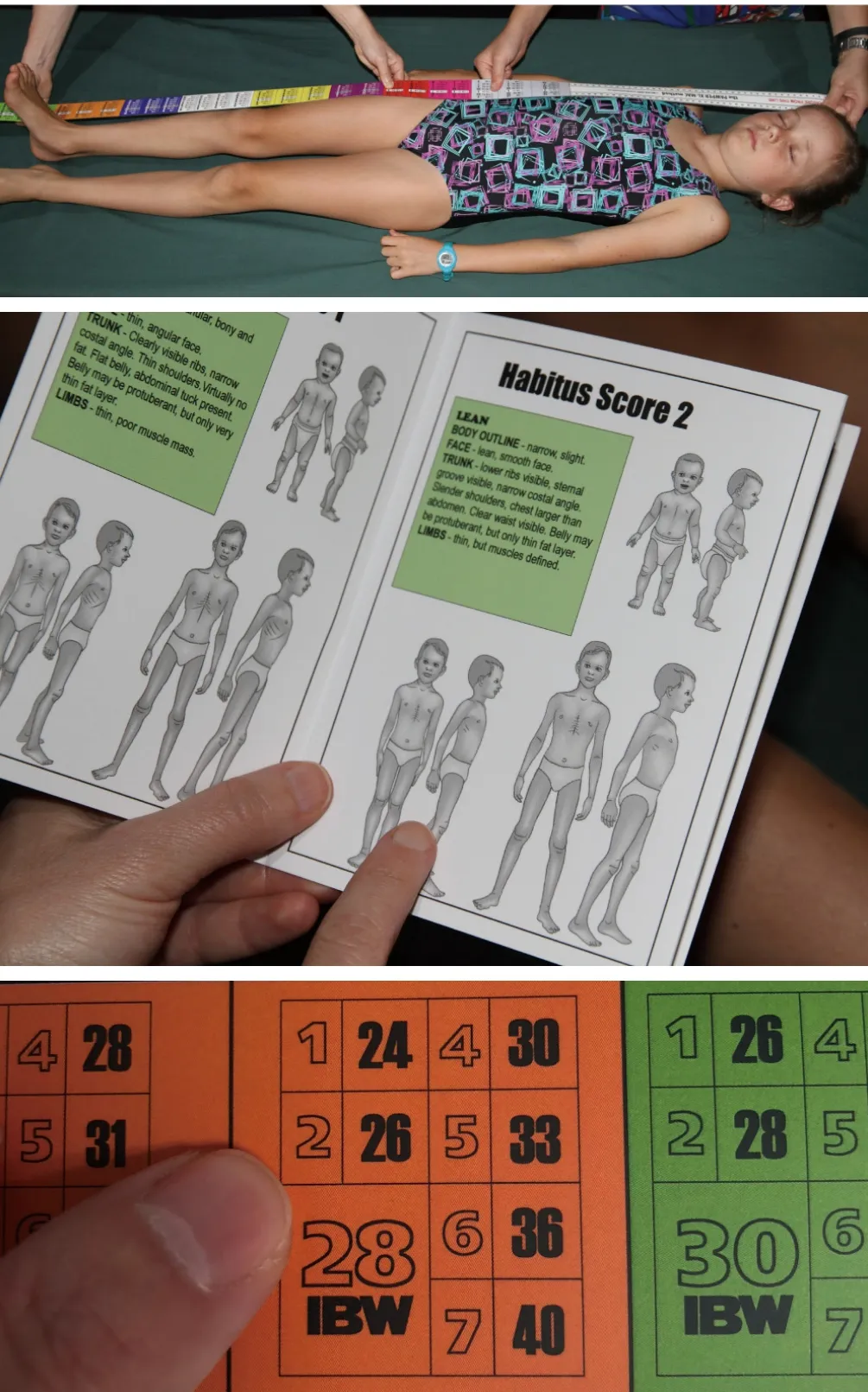
Figure 1. A description of the PAWPER tape and how it is used.
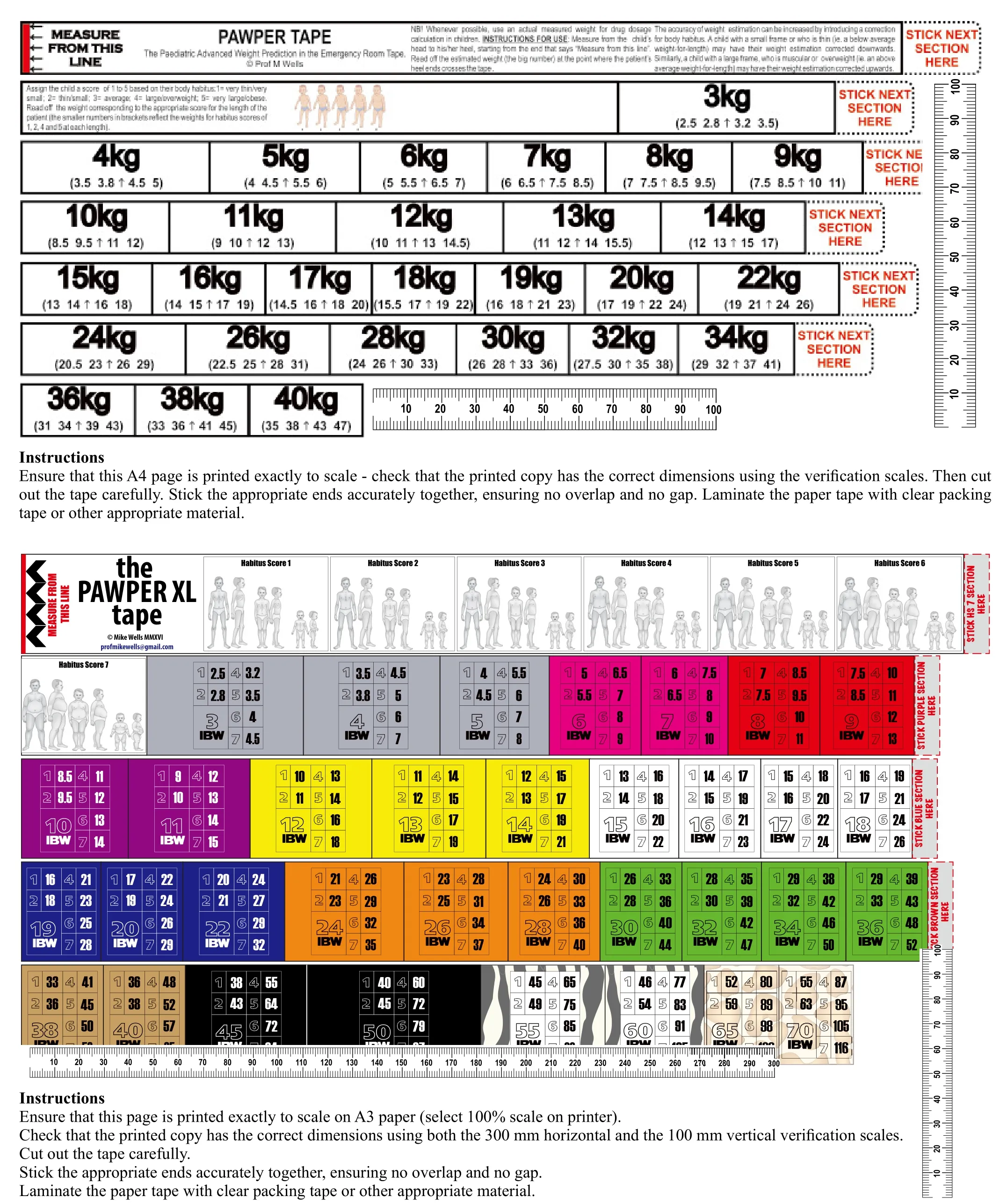
Figure 2. The “PAWPER-on-a-page” and the “PAWPER XL-on-a-page” images that were used for the study.
Step 3 the weight for the appropriate habitus score is read directly off the tape in the segment at which the child's heel crossed the tape.commercial printers and to compare the cost and accuracy of each; to determine how long it would take healthcare providers to assemble the “PAWPER-on-a-page” and the “PAWPER XL-on-a-page” and to determine the prevalence and magnitude of assembly errors; to determine the satisfaction of the participants with the final assembled tape
METHODS
Participants
Doctors and nurses from two academic institutions in Gauteng, South Africa were invited to participate.Healthcare providers who had home internet access,a home printer and access to transportation to go to a commercial printer were eligible for inclusion. This study was approved by the Human Research Ethics Committee of the University of the Witwatersrand. All volunteers signed written informed consent. A sample size of 24 participants was required to allow an 80%power to detect a 20% difference in paired comparisons between groups using the McNemar test.
Study protocol
The participants were given an instruction sheet which provided detailed step-by-step instructions on what they would be required to do: (1) Download the two image files (the “PAWPER-on-a-page” and the“PAWPER XL-on-a-page”) from google docs (Figure 2).(2) Watch the YouTube video instructions for the printing and assembly (https://youtu.be/gFbbPtfxLFI). (3) Print two copies of the “PAWPER-on-a-page” on their home printer and get one copy of the “PAWPER-on-a-page”and two copies of the “PAWPER XL-on-a-page” printed at a commercial printer. The importance of printing the pages exactly to scale was emphasized. (4) Cut out and assemble a home-printed “PAWPER-on-a-page” and a commercially printed “PAWPER XL-on-a-page”. (5)Take note of and record the time taken to complete each task. (6) Complete the questionnaire attached to the instruction sheet. Return the questionnaire, the assembled tapes and the unassembled printed documents to the researchers. (7) The participants were remunerated for the costs of the home and commercial printing.
Data collection
After the completed items were returned by the participants, the printed “PAWPER-on-a-page” and“PAWPER XL-on-a-page” and the assembled tapes were examined to determine the accuracy of the printing and of the finished product. The calibration scales on the printed pages were measured with a high-precision metal ruler (to the nearest 0.5 mm). Measurements of the length and accuracy of the assembled tapes were obtained using a high-precision steel measuring tape (to the nearest 1 mm).Finally, the data from the questionnaires completed by the participants was captured. This included information on the time taken for assembly of the tapes, the costs of printing and any comments about the process from the participants.
Data analysis
The proportion of printed pages in which errors were detected was calculated and a comparison made between home-printed pages and commercially-printed pages using the Fisher exact test. A percentage error was calculated for total length for each of the assembled tapes. The medians and interquartile ranges for the printing costs and assembly times were calculated. The questionnaire responses were evaluated using basic qualitative research techniques, focused on identifying trends and common themes in the answers.
Outcome measures
The a priori tolerance that was allowed for error was 0.2% (3 mm for the PAWPER tape and 4 mm for the PAWPER XL tape). Tapes with errors exceeding these values were considered to be inaccurate. This tolerance was selected as we were concerned that any greater error could potentially increase the risk of weight estimation errors.
RESULTS
Characteristics of participants
A total of 36 invitations were issued and 32 participants completed the activity (89%). There were two nurses(6.2%) and 30 doctors (93.8%).
Main results
The results of the analyses the page scale error,the assembly times and the costs of the printed pages are shown in Table 1. Approximately two thirds of all the printed tapes fulfilled the predetermined accuracy standards, with no significant differences in scaling error rates between home- and commercially printed tapes.About three quarters of the tapes were assembled within 10 minutes, with no significant difference between the PAWPER and PAWPER XL tapes. The black and white PAWPER tapes all cost less than 20 US cents while the full colour PAWPER XL tapes cost about 1 US dollar.
The results of the accuracy analysis of the assembled tapes, in terms of percentage errors, are shown in Figure 3. The assembly process added minimal errors in the final assembled tapes because all but one of the participants(96.9%) assembled the tapes with sufficient precision not to affect the overall accuracy of the tape. This meant that more than 72% of PAWPER tapes and 67% of PAWPER XL tapes achieved the required standard of accuracy.
The comments from the participants regarding the study are shown in Table 2. All participants reported that the assembly process was easy and virtually all participants were satisfied with the final assembled tapes. The majority of the tapes that were printed with a significant scale error were identified by the participants.
DISCUSSION
The findings of the study were clear that the tapes were quickly, easily and accurately assembled, according to both the objective findings and the participant feedback, and that the system was favourably received.More than two-thirds of the assembled tapes were within the allowable error margin of 0.2% and the majority of the tapes falling outside of this limit were identified by the participants. The commercial printing was also inexpensive, costing at most $1 for the colour A3 “PAWPER XL-on-a-page” printing. These were positive factors supporting the safe use and the potential acceptance of this system. The negative factors were the relatively high number of tapes that were not printed exactly to scale, both by the participants as well as the commercial printers.
This was the first study on this topic, with no similar studies with which to compare this one. There has been no previous work on the required accuracy tolerances of length-based weight estimation devices,or on methods of improving international access to not-for-profit weight estimation systems. One of the other “top three” weight estimation systems, the Mercy method, has freely-available tables which may be used to convert measurements of humeral length and mid-arm circumference into estimates weights.[8]The actual 2D and 3D Mercy tapes are not yet available but are likely to be distributed on a for-pro fit basis.
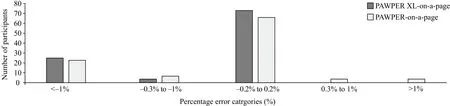
Figure 3. Error rates of the assembled tapes. The third rectangle indicates the proportion of tapes with an acceptable error. A negative figure indicates tapes in which the scale was too small (i.e. the tapes were too short).

Table 1. Printing scale error rate, assembly time and cost for each system

Table 2. Participant feedback obtained via questionnaire
The accuracy of the printing process was the single major concern, however, as nearly one-third of the printed pages were outside the specified tolerance level.This was most likely as a result of incorrect printer scale settings or a problem with the program reading the PDF image files. This would probably not have resulted in a potentially dangerous final product, however. Every page that was printed incorrectly could be identified,before assembly, using the calibration scale on the page.Furthermore, an assembled tape that was outside of the tolerance parameters could be easily identified by simple measurement of the length of the tape. This checking and double-checking might add to the time taken but would be essential to ensure that the system was appropriate for use. Fortunately, two-thirds of the printed pages were perfectly to scale, and the final assembled tapes were acceptably accurate.
Following the suggestions of the participants, some minor changes were made to the design of the image files. This primarily involved the spacing of the panels on the “PAWPER-on-a-page” to require fewer cuts. The instructions were amended to emphasise the need to check the printing scale and then double check the final assembled tape to ensure accuracy. The final versions of the “PAWPER-on-a-page” and the “PAWPER XL-on-a-page” may be found in the supplementary online material (Figures 4, 5).
Limitations
It is not known what exact tolerance level for error would be required to prevent errors in weight estimation,so for this reason, a moderately stringent error limit was used. There were some costs that could not be taken into account (e.g. transport to the commercial printers)and some that were not considered (e.g. the cost of the plastic tape which may be used as a cover). Images files in different formats (e.g. JPEG) were also not evaluated in this study. Finally, this study did not evaluate the time taken to make the tapes more robust, although the use of an outer covering would be strongly recommended.The use of a clear plastic tape coating for the paper tapes would increase their durability and strength.
CONCLUSION
The “PAWPER-on-a-page” system could be quickly,easily, cheaply and accurately printed and assembled,with a unanimous approval by the participants. The potential for inaccurate printing was identified and the printed pages and final assembled tapes would need to be carefully evaluated to ensure that they fall within acceptable accuracy limits. The participants in this study had no previous experience with the “PAWPER-ona-page” system and are likely to be representative of users anywhere in the world with access to the resources defined in the inclusion criteria.
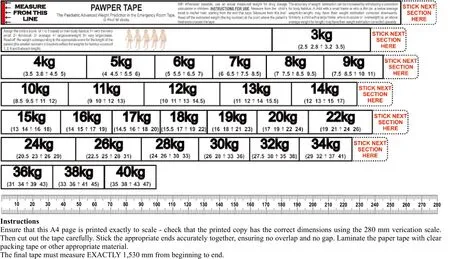
Figure 4. The “PAWPER-on-a-page”.
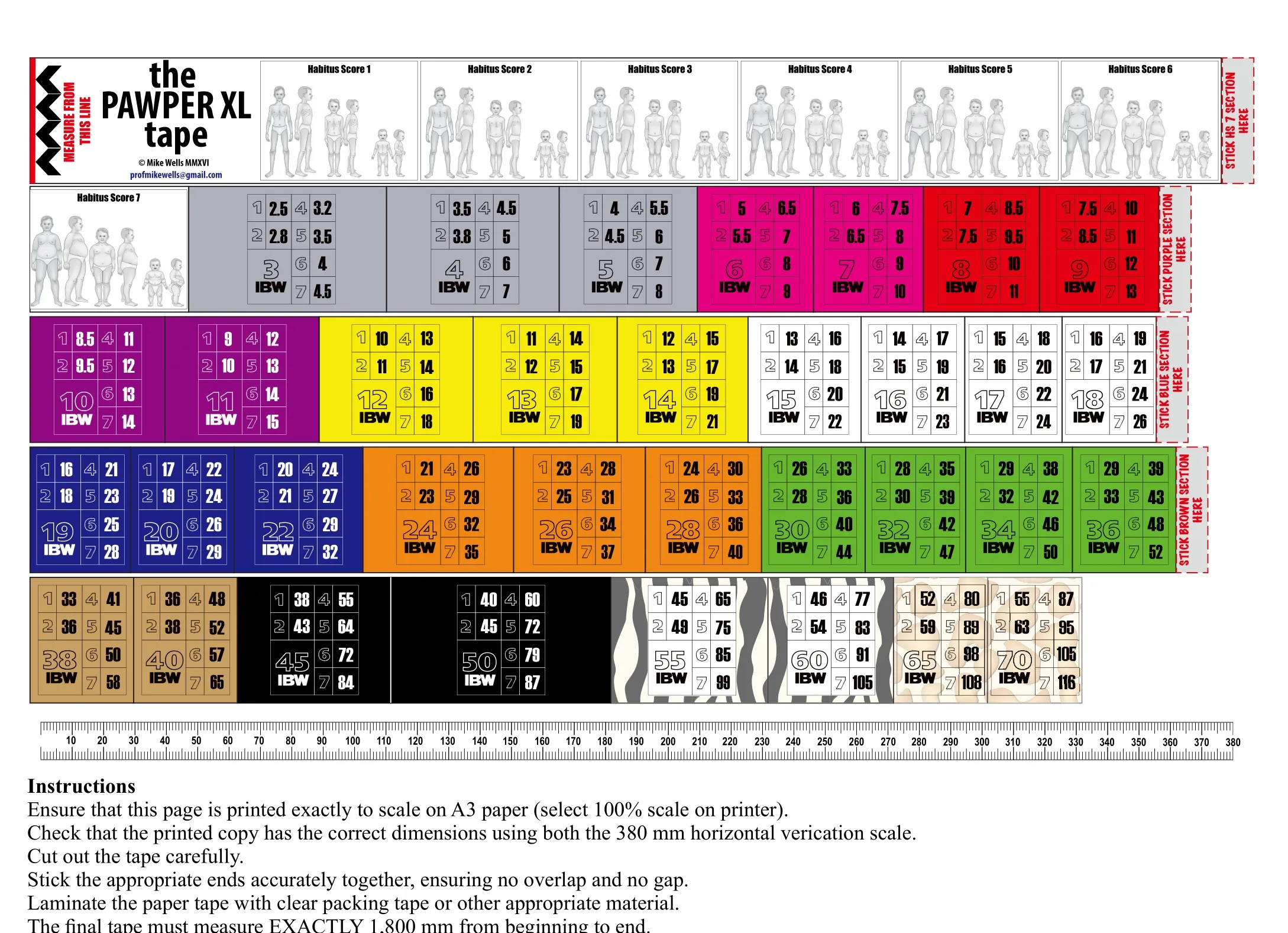
Figure 5. The “PAWPER XL-on-a-page”.
Implications of these findings
These findings have managerial, clinical and academic implications, primarily that the global availability of the PAWPER tape could be increased easily and at minimal cost. This would allow increased usage of the PAWPER tape in clinical practice as well as facilitate further research on the tape in different populations and settings.
Recommendations and future studies
The PAWPER-on-a-page system can be used to create tapes for clinical and research work, especially in lowresource settings, if the original tapes are not available.
Future studies should be conducted to validate the PAWPER-on-a-page system in other settings and by other users - both the accuracy of the printing and assembly as well as the accuracy of the assembled tape in a clinical setting. This would allow further independent evaluation of the accuracy of the PAWPER tape system in different populations.
Funding:None.
Ethics approval:This study was approved by the Human Research Ethics Committee of the University of the Witwatersrand.
Competing interests:The authors have no conflict of interest, no financial issues to disclose.
Contribution:All authors have substantial contributions to the acquisition, analysis, or interpretation of data for the work;drafting the work or revising it critically for important intellectual content; and final approval of the version to be published.
 World journal of emergency medicine2019年2期
World journal of emergency medicine2019年2期
- World journal of emergency medicine的其它文章
- Keeping nephrotic syndrome on the emergency department edema differential: A case report
- Instructions for Authors
- A patient presenting painful chest wall swelling:Tietze syndrome
- Central nervous system manifestations due to iatrogenic adrenal insufficiency in a Ewing sarcoma patient
- Perceived effectiveness of infection control practices in Laundry of a tertiary healthcare centre
- Can an 8th grade student learn point of care ultrasound?