
Lack of validity of self-reported mammography data
2019-04-11 06:27:36RobertLevineBarbaraKilbourneMaureenSandersonMaryFaddenMariaPisuJasonSalemiMariaCarmenzaMejiadeGrubbHeatherHaraBaqarHusainiRogetZoorobCharlesHennekens
Robert S Levine, Barbara J Kilbourne, Maureen Sanderson, Mary K Fadden, Maria Pisu, Jason L Salemi, Maria Carmenza Mejia de Grubb, Heather O'Hara, Baqar A Husaini, Roget J Zoorob, Charles H Hennekens
ABSTRACT This qualitative literature review aimed to describe the totality of peer-reviewed scienti fi c evidence from 1990 to 2017 concerning validity of self-reported mammography.This review included articles about mammography containing the words accuracy, validity, specificity,sensitivity, reliability or reproducibility; titles containing self-report, recall or patient reports, and breast or‘mammo’; and references of identified citations focusing on evaluation of 2-year self-reports. Of 45 publications meeting the eligibility criteria, 2 conducted in 1993 and 1995 at health maintenance organisations in Western USA which primarily served highly educated whites provided support for self-reports of mammography over 2 years. Methodological concerns about validity of selfreports included (1) telescoping, (2) biased overestimates particularly among black women, (3) failure to distinguish screening and diagnostic mammography, and (4) failure to address episodic versus consistent mammography use. The current totality of evidence supports the need for research to reconsider the validity of self-reported mammography data as well as the feasibility of alternative surveillance data sources to achieve the goals of the Healthy People Initiative.
lNTRODUCTlON
The Healthy People Initiative, administrated by the Office of Disease Prevention and Health Promotion of the US Centers for Disease Control and Prevention (CDC),provides science-based, 10-year national objectives which constitute a national prescription for improving the health of all Americans.1The programme establishes benchmarks and monitors progress over time, partly to measure the impact of prevention activities.1The Initiative also identifies specific data sources to be used for each objective. For breast cancer prevention, Objective C-17 for Healthy People 2020 aims to ‘Increase the proportion of women who receive a breast cancer screening based on the most recent guidelines’.2The target population includes women ages 50–74 years. The data source designated for surveillance of progress towards this objective is the National Health Interview Survey (NHIS),also administered by the CDC.2The NHIS is a nationwide, cross-sectional, inperson,household interview survey based on cluster sampling of households and non-institutional group quarters (eg, college dormitories).3The following are specific NHIS questions used for monitoring: (1) Have you ever had a mammogram? and (2) When did you have your most recent mammogram?2Mammograms themselves are described as ‘An x-ray of each breast to look for breast cancer’.4Monitoring estimates track the percentage of women aged 50–74 years who have had a mammogram in the past 2 years. Data used for monitoring are therefore based on self-report, which has been criticised for its tendencies towards over-reporting, particularly among minority populations.5Moreover, these NHIS questions do not distinguish between screening mammograms and mammograms which are used for follow-up after a diagnosis of breast cancer has been made, thereby adding to the probability of overestimation.5
Possible reasons for overestimation among blacks and African–Americans include the less detailed wording of the NHIS questions pertaining to mammography. In part, this possibility became apparent in the data from the US Behavioral Risk Factor Surveillance System (BRFSS). BRFSS is a long-standing state and local telephone survey of non-institutionalised residents regarding health-related risk behaviours, chronic health conditions and use of preventive services.6More than 400 000 adult interviews are conducted each year.6The BRFSS questionnaire wording reveals that more specific descriptions of mammography (ie, ‘A mammogram is an X-ray of the breast and involves pressing the breast between two plastic plates’) resulted in lower estimates of mammography use, particularly among African–Americans.5A possible reason is that the more graphic description resulted in increased specificity in responses.5It is also proposed that women with poor health who may be seeking care for numerous conditions requiring frequent contact with the medical system may make the specifics of mammography less distinct and more difficult to recall.7
At present, plans are under way for Healthy People 2030,8so it seems important and timely to conduct a comprehensive qualitative review of peer-reviewed scientific publications pertaining to the validity of self-reported mammography.
METHODS
We used Medline search strategies previously reported in meta-analyses of the validity of self-reported mammography.910These strategies included using article titles containing the words accuracy, validity, specificity, sensitivity, reliability or reproducibility, and titles containing self-report, recall or patient reports, and breast or‘mammo’. We also searched the references of identified citations to locate additional studies of interest.We described the resulting publications in terms of time, place, age, race and ethnicity, source of the study population, type of healthcare facility, whether there was information on annual and/or biennial frequency of mammography, and whether 2-year self-reports were specifically addressed. The enquiry focused on 2-year self-report. This is particularly pertinent to Healthy People since women with mammography screening within 2 years are considered up to date. In addition,since Medicare provides insurance benefits for mammography to all women 65 years and older, we also explored specific information about this population.
RESULTS
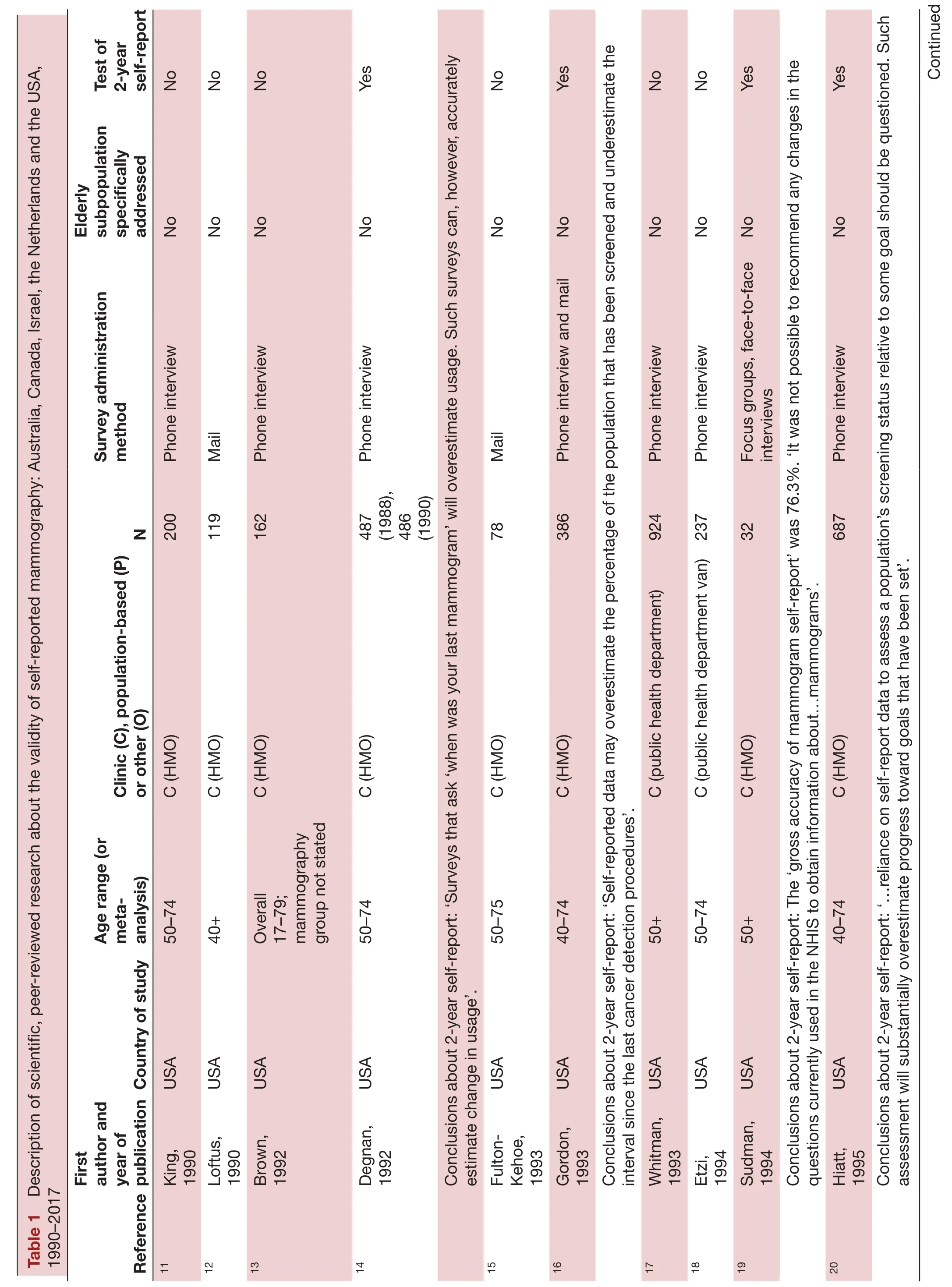
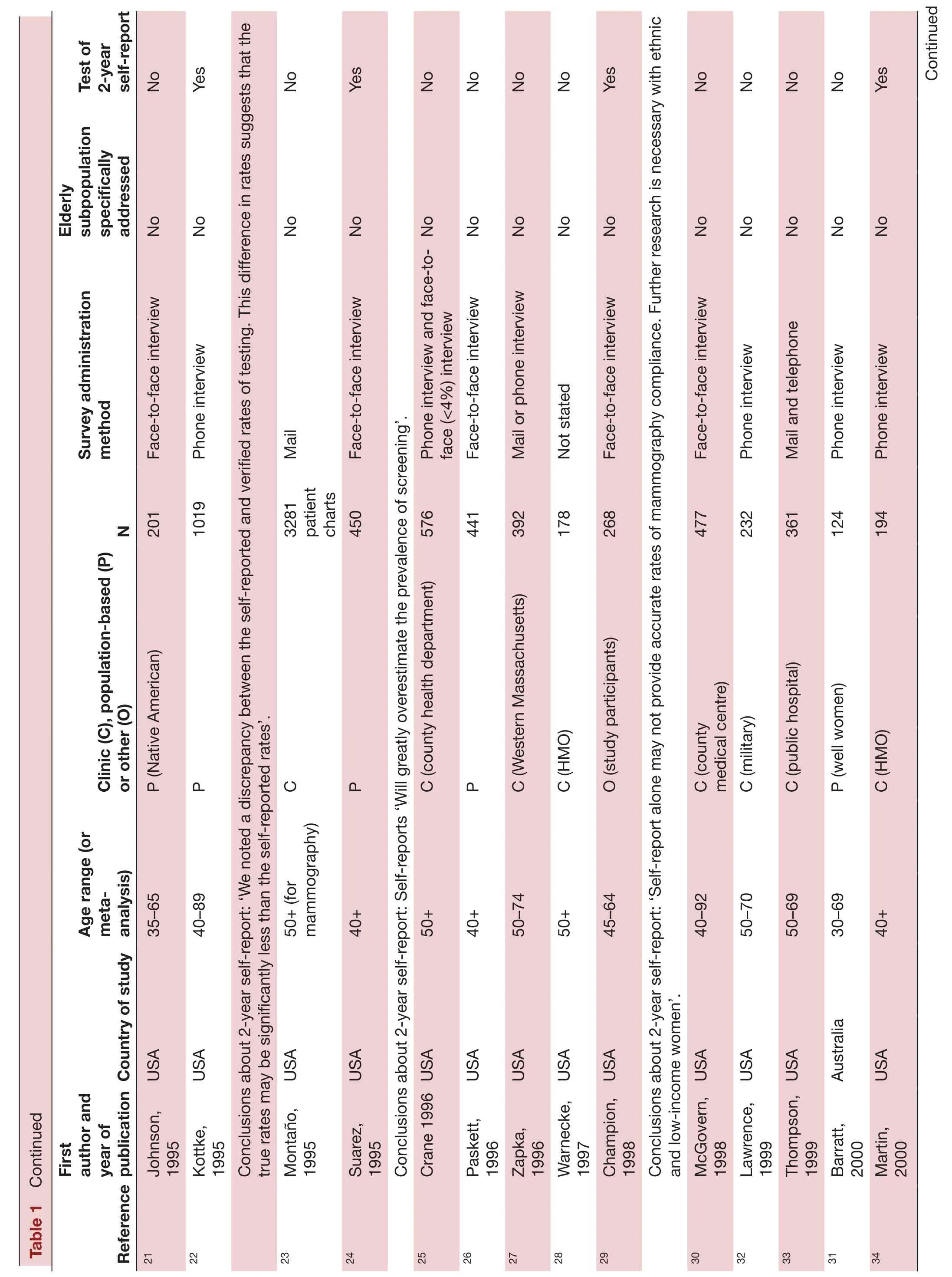
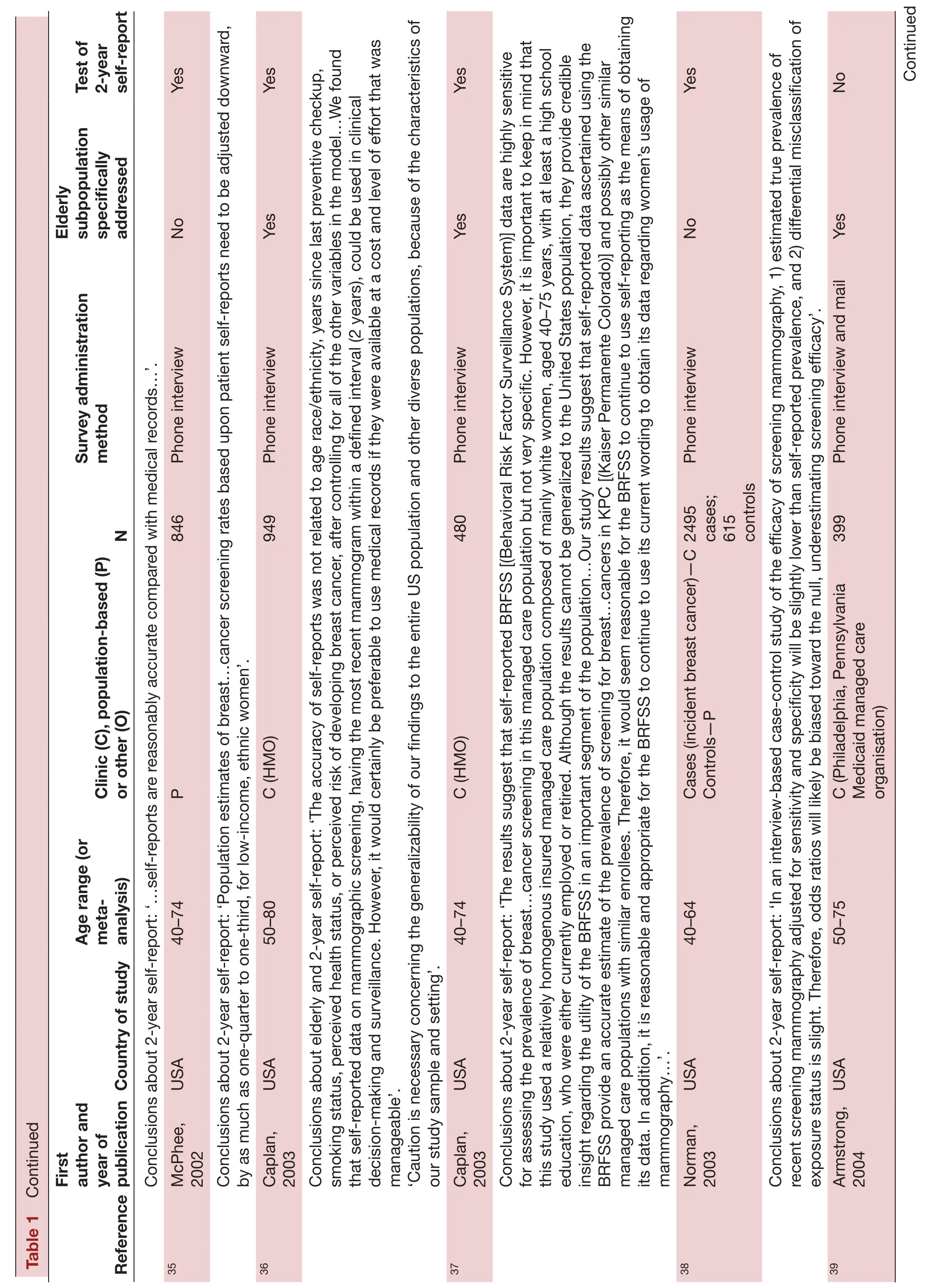
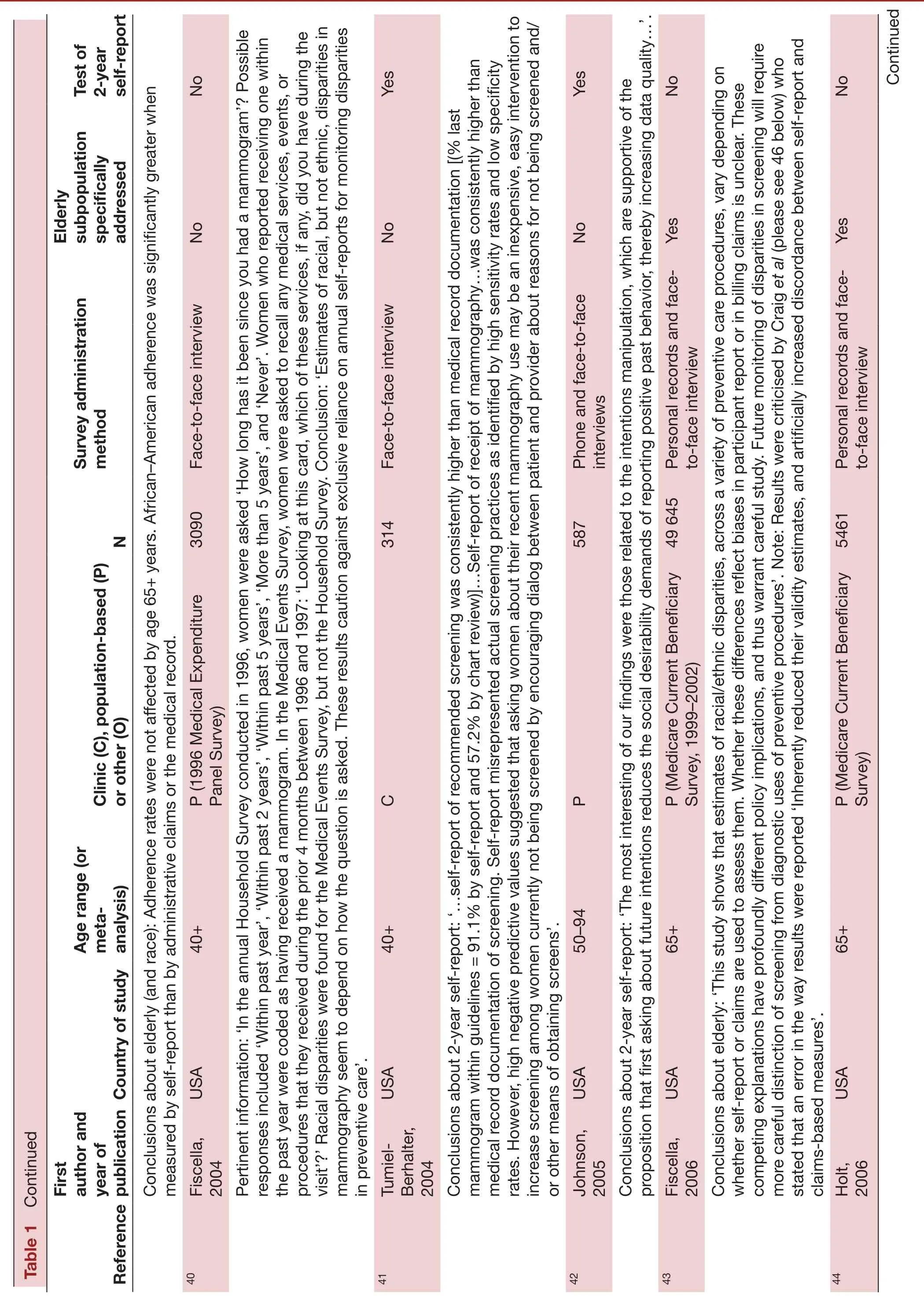
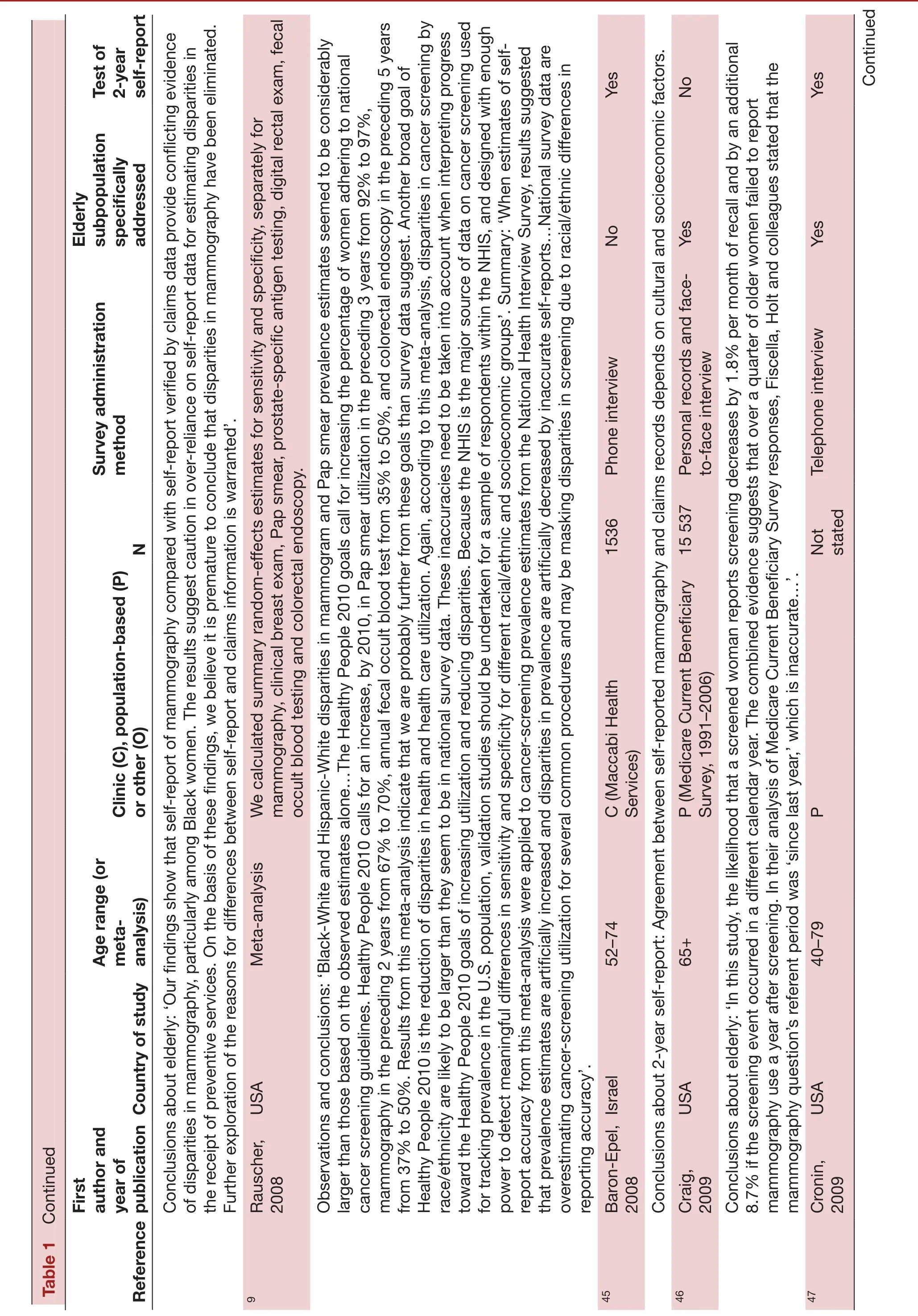
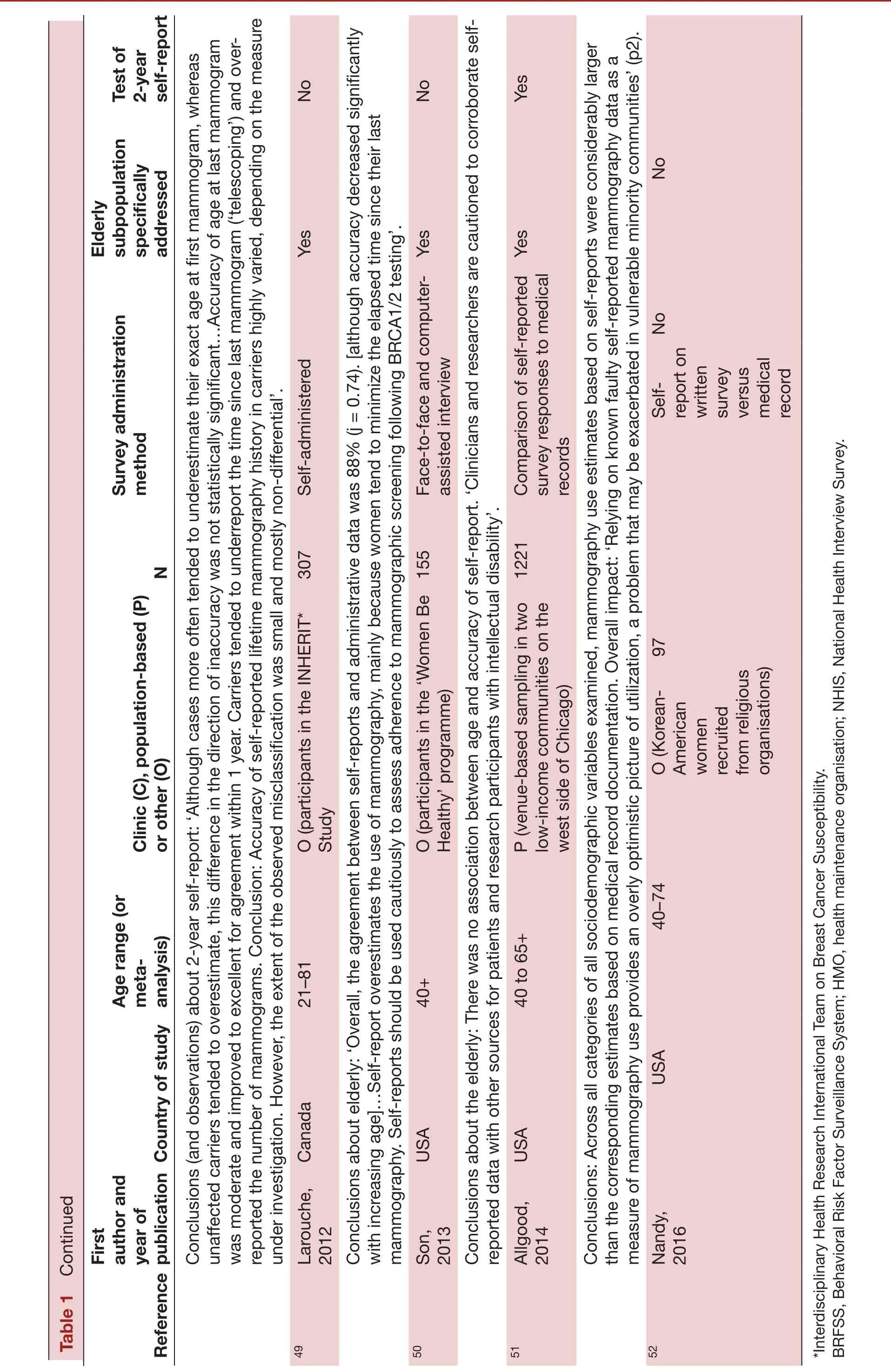
Forty-five publications were identified (4, 9–52),49–52and these are summarised in table 1. In all, 9 articles were published from 1990 to 1994,11–1913 from 1995 to 1999,20–329 from 2000 to 2004,33–418 from 2005 to 2009,91042–475 from 2010 to 2014,448–51and 1 from 2015 to January 2018.52Aside from the USA, countries of origin included Canada,49Israel45and the Netherlands.48The lower age limit for inclusion for all but three studies was 40 years. Two of the three studies accepting women younger than 40 years were concerned with validity of self-reports among persons with known genetic risk for breast cancer.4849Participants included a variety of racial(black, white, Native American, Asian) and ethnic/religious (Arab, French Canadian, Hispanic, Orthodox Jewish) groups. Studies included persons from across the socioeconomic spectrum, although several studies(reviewed in refs 10) focused on the socioeconomically disadvantaged. One study50concerned persons with intellectual developmental disabilities. Settings (specifically identified in table 1) for the 42 non-meta-analysis studies included health maintenance organisations (HMOs)(n=12), non-HMO clinical services (n=13), populations(n=13) and participants in research investigations (n=4).Of the 45 articles, 27 addressed 2-year recall or recall in the elderly. Of these, only two studies supported the validity of self-reported, 2-year recall among the elderly(65+ years of age). Each was done in HMO settings in 1993 and 1995 and reported in 2003.3637While finding the accuracy of self-reports acceptable in the study settings, the authors nonetheless cautioned against projecting their findings to the general population:‘Caution is necessary concerning the generalizability of our findings to the entire US population and other diverse populations, because of the characteristics of our study sample and setting’.36In the second study of Caplan et al,37they noted: ‘It is important to keep in mind that this study used a relatively homogenous insured managed care population composed of mainly white women, aged 40–75 years, with at least a high school education, who were either currently employed or retired. Although the results cannot be generalized to the United States population, they provide credible insight regarding the utility of the BRFSS in an important segment of the population…Our study results suggest that self-reported data ascertained using the BRFSS provide an accurate estimate of the prevalence of screening for breast…cancers in KPC[(Kaiser Permanente Colorado)] and possibly other similar managed care populations with similar enrollees’.
Holt et al44conducted a particularly relevant study in which they compared the responses of 5461 participants in the Medicare Current Beneficiary Survey with claims data. Each participant, in effect, served as her own control.The authors concluded that ‘On the basis of these findings, we believe it is premature to conclude that disparities in mammography have been eliminated. Further exploration of the reasons for differences between self-report and claims information is warranted’.
Two meta-analyses focused on current self-reporting methods used for the NHIS9and BRFSS.4Each of these reports concluded that these methods overestimate mammography utilisation and underestimate racial disparities or inequalities. Specifically, Rauscher et al9concluded that
When estimates of self-report accuracy from this meta-analysis were applied to cancer-screening prevalence estimates from the National Health Interview Survey, results suggested that prevalence estimates are artificially increased and disparities in prevalence are artificially decreased by inaccurate self-reports…National survey data are overestimating cancer-screening utilization for several common procedures and may be masking disparities in screening due to racial/ethnic differences in reporting accuracy
Rauscher et al9specifically cautioned against reliance on the NHIS, stating that
Because the NHIS is the major source of data on cancer screening used for tracking prevalence in the U.S.population, validation studies should be undertaken for a sample of respondents within the NHIS, and designed with enough power to detect meaningful differences in sensitivity and specificity for different racial/ethnic and socioeconomic groups
d ue ntin Co
d ue ntin Co
d ue ntin Co
d ue ntin Co
d ue ntin Co
d ue ntin Co
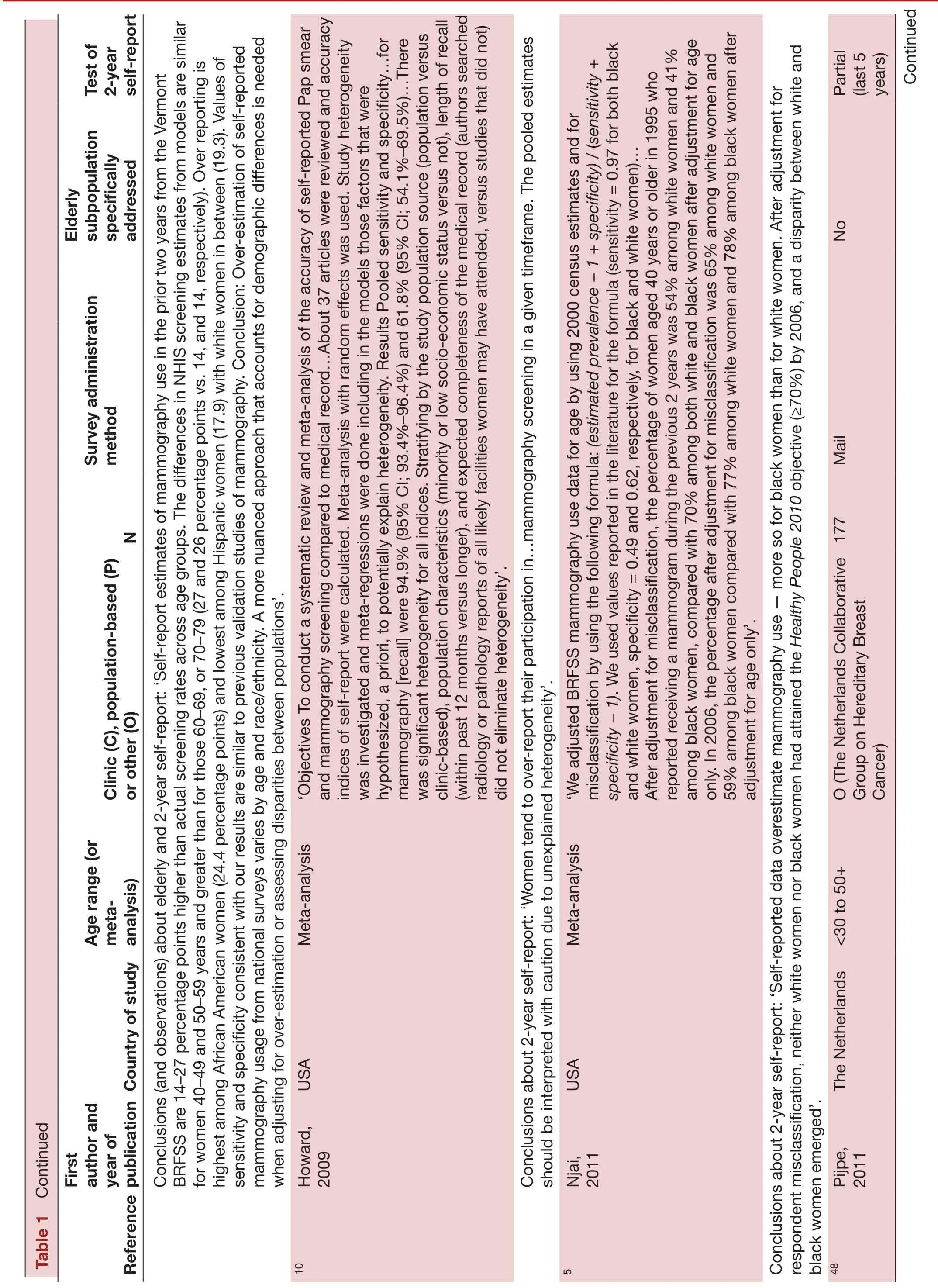
Njai et al5concluded that ‘Self-reported data overestimate mammography use — more so for black women than for white women. After adjustment for respondent misclassification, neither white women nor black women had attained the Healthy People 2010 objective (≥70%) by 2006, and a disparity between white and black women emerged’. With reference to 2-year self-report, they concluded that ‘Women tend to over-report their participation in…mammography screening in a given timeframe. The pooled estimates should be interpreted with caution due to unexplained heterogeneity’.4
DlSCUSSlON
The present qualitative review of the totality of published evidence suggests a lack of validity of self-reports of mammography. This review also documents the historical development of scientific evidence about the quality of self-reported information provided in response to health survey questions about mammography screening. It demonstrates a remarkably consistent set of challenges to surveillance practices of the Healthy People programme,even as methods of analysis have grown increasingly complex. The narrative approach was also chosen, in part,because extensive, well-done meta-analyses confirming previous concerns about self-report have already been published4910to little or no apparent effect.53Perhaps,by presenting more than quarter-century of research as it has evolved, the depth of scientific objections will become clearer.
In part, persistence of the present self-reported information protocols for mammography may reflect assertions that self-report is the only feasible, cost-effective way to obtain such information.52Nonetheless, the aforementioned NHIS questions (ie, Have you ever had a mammogram? and When did you have your most recent mammogram?)4are subject to several cogent concerns about bias, including (1) telescoping, whereby people recall distant events as occurring more recently than they actually happened54; (2) greater likelihood of producing inconsistent/overestimates from black women7; (3)failure to distinguish between screening and diagnostic mammography4; and (4) failure to address the issue of whether mammography screening is consistently used (as opposed to being ‘up to date’). This is so, even though additional questions already included in the NHIS survey were used as resources for tracking the progress of the Healthy People programme.55
Biased overestimates of mammography screening use may have serious adverse clinical and public health consequences. For example, Dr Harold Freeman, a past president of the American Cancer Society, wrote in the New York Times:…for many years, the dominant cause of higher mortality has been late-stage disease at the time of initial treatment, in part as a result of black women being less likely to undergo mammography. However, this gap has been closed. The CDC reports that the rate of mammography is now the same in black and white women….56
Similarly, the Susan G Komen Foundation, a leading organisation which focuses exclusively on breast cancer,quotes data to the effect that ‘Black women now have slightly higher rates of mammography use than other women’.57Based on the present data, neither the Freeman nor the Komen statements are likely to be accurate.
Aside from making more comprehensive use of existing NHIS information, additional surveillance alternatives include greater use of administrative claims58and HEDIS(Healthcare Effectiveness Data and Information Set),59as well as expansion of mammography registries.60Specifically, Smith-Bindman et al58noted that 94% of women who had at least one mammogram within a 2-year reference period were accurately classified by administrative claims data as having undergone a mammogram during that period. Also, while Medicare claims are not available from HMOs, these organisations and others do provide information on mammography utilisation to the HEDIS.59Finally, the National Cancer Institute’s Breast Cancer Surveillance Consortium60might serve as a national mammography registry model, but at present it only operates in the states of New Hampshire, North Carolina; Vermont; Washington; San Francisco, California; and Chicago, Illinois.60
In conclusion, the current totality of evidence supports the need for research to reconsider the validity of self-reported mammography data as well as the feasibility of alternative surveillance data sources to achieve the goals of the Healthy People Initiative.
ContributorsConception and design of study: RSL. Acquisition of data: RSL.Analysis and interpretation of data: RSL, BJK, MS, MKF, MP, JLS, MCMdG, HOH,BAH, RJZ, CHH. Drafting the manuscript: RSL, BJK, MS, MKF, MP, JLS, MCMdG, HOH,BAH, RJZ, CHH. Approval of the manuscript to be published: RSL, BJK, MS, MKF, MP JLS, MCMdG, HOH, BAH, RJZ, CHH.
FundingUS Department of Health and Human Services, National Institutes of Health, National Institute on Minority Health and Health Disparities (grant number 5P20MD/000516-07).
Competing interestsNone declared.
Patient consentNot required.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4.0
 Family Medicine and Community Health2019年1期
Family Medicine and Community Health2019年1期
- Family Medicine and Community Health的其它文章
- Obstacles for Iranian rural population to participate in health education programmes: a qualitative study
- Qualitative study to identify the perception and challenges faced by the faculty of community medicine in the implementation of competency-based medical education for postgraduate students
- OxyContin and the McDonaldization of chronic pain therapy in the USA
- Health services utilisation and responsiveness profiles in Iran: a provincial household study
- Out-of-pocket expenditure of families on the healthcare of children younger than 5 years
- Journey of a Lifetime