Malignant epidermoid arising from the third ventricle: A case report
2019-06-20 03:34:26SamadhanPawarChaitanyaBordeAtulPatilRajnishNagarkar
World Journal of Radiology 2019年5期
Samadhan Pawar,Chaitanya Borde,Atul Patil,Rajnish Nagarkar
Abstract
Key words: Epidermoid;Third ventricle;Magnetic resonance imaging;Case report
INTRODUCTION
Epidermoid cysts are an uncommon finding in routine clinical settings.They are slowgrowing,benign tumors that grow in the extra-axial areas.Epidermoid cysts account for less than 1% of all intracranial tumors.Intracranial dermoid cysts are often observed in the cranial midline,sub-frontal areas,posterior fossa,and suprasellar cistern.Intraventricular dermoid cysts are extremely rare and have been reported in the fourth ventricle.Current imaging modalities have made it possible to recognize intracranial tumors.The use of radiologic diagnosis for third ventricle epidermoid cysts is almost always possible.
We present a case of epidermoid cysts in the third ventricle in an adult male.
CASE PRESENTATION
Chief complaints
A 48-year-old male presented to our outpatient department with vomiting,headache,and involuntary micturition.
History of present illness
The above-mentioned symptoms had been present for five days.
History of past illness
The patient had no history of major illness.
Personal and family history
The patient had no relevant family history.
Physical examination upon admission
The patient had no pallor.General condition of the patient was normal.
Laboratory examinations
The patient’s routine laboratory investigations were within normal limits.
Imaging examinations
A non-contrast computed tomography scan of the head revealed a mass arising from the third ventricle appearing hypodense and showing coarse nodular as well as curvilinear calcifications (Figure 1).
A contrast-enhanced computed tomography (CT) of the head demonstrated minimal perilesional enhancement.The lesion obstructed the hydrocephalus of the lateral ventricles (Figure 2).No dilatation of the fourth ventricle was observed.The lesion measured 8-10 Hounsfield units.The maximum size of the lesion measured 77x57 mm on CT scan.
Magnetic resonance imaging (MRI) of the lesion revealed a large,lobulated,septated T2 hyperintense mass arising from the third ventricle (Figure 3B).It was hypointense on T1-weighted imaging with few cystic areas (Figure 3A).Few calcifications were observed within the cystic areas.On diffusion-weighted magnetic resonance imaging,the lesion showed increased restricted diffusion (Figure 3D).The lesion obstructed the hydrocephalus and caused moderate dilatation of the bilateral lateral ventricles.No dilation of the fourth ventricle was observed.On contrastenhanced CT scan,the lesion showed minimal peripheral enhancement without any demonstrable solid enhancing component.The maximum size of the lesion measured 73 mm × 65 mm × 64 mm in size (Figure 4).
On MR spectroscopy,there was high lipid/lactate peak with comparatively lower N-acetylaspartate (NAA) and choline levels.The maximum choline (Cho)/creatine ratio was 2.85 within the lesion and CHO/NAA ratio was 0.766 (Figure 5).MR perfusion derived relative cerebral blood volume (rCBV) maps demonstrating heterogeneous perfusion abnormalities.Mild higher normalized rCBV ratios in comparison with white matter were noted in the peripheral region of the cyst,which corresponded to malignant transformation (Figure 6).

Figure 1 A non-contrast computed tomography scan of the head showing a mass arising from the third ventricle appearing hypodense and showing coarse nodular as well as curvilinear calcifications.
FINAL DIAGNOSIS
Considering the imaging findings,we suspected the lesion to be an epidermoid,dermoid,or an arachnoid cyst.However,we ruled out the diagnosis of a dermoid or arachnoid cyst considering the presence of a restricted diffusion on diffusionweighted imaging (DWI).A combination of T1WI,T2WI,T2 axial FLAIR,and DW imaging techniques helped us diagnose an epidermoid cyst.However,the use of MR spectroscopy helped in making the probable diagnosis of a malignant epidermoid cyst arising from the third ventricle.
TREATMENT
The patient underwent craniotomy coupled with intra-hemisphere excision of the tumor.The patient was given levetiracetam 500 mg twice a day.
OUTCOME AND FOLLOW-UP
The patient is stable and currently doing well.
DISCUSSION
Epidermoid cysts are slow-growing and often benign congenital tumors that comprise 0.2%-1.8% of primary intracranial neoplasms.The first epidermoid cysts were described by an artist in 1807 in a French medical school.The French pathologist Cruveilhier gave the first full description of epidermoid cysts.From a histological point of view,epidermoid cysts often resemble the linear growth rate of the skin.They are made up of a thin epithelium lining that appears pearly white and smooth macroscopically.Epidermoid tumors often have a high content of cholesterol and an internal core composed of desquamated epithelial keratin that is distinctive on MR imaging and allied radiological modalities.
To the best of our knowledge,intracranial epidermoid cysts are located off the midline.The most common location of epidermoids includes the region within the cerebellopontine angle (CPA).Intracranial epidermoids account for the third most common tumor in the CPA region followed by vestibular schwannoma and meningioma.
There have been more than 100 cases of epidermoids reported in the fourth ventricle,followed by the parasellar and sellar regions.However,epidermoids may also be found in the lobes of the cerebral hemisphere,spine,and brainstem.
To the best of our knowledge,third ventricular epidermoid tumors are extremely rare.Patients with epidermoid tumors often present with signs and symptoms such as headache,seizures,cranial nerve defects,raised intracranial pressure,and cerebral signs.Our patient presented with headache and vomiting.

Figure 2 A contrast-enhanced computed tomography of the head demonstrates minimal perilesionalenhancement.
Epidermoids appear as well-defined lobulated,round hypoattenuated masses on CT imaging.However,there have been reports where uniformly hyperdense epidermoids have been reported on CT imaging,which are associated with a calcium constitution or high protein content.Epidermoids appear hyperintense on T2 weighted and hypointense on T1 weighted MRI imaging.In our case,we observed a hyperintense T2 weighted mass on MRI imaging.Lastly,MR spectroscopy showed an increase in the lactate peak,which was indicative of anaerobic metabolism.There was an increase in the Cho/NAA ratio,which is generally observed in neoplasms.The Cho/Cr ratio increased to 2.85.
As per current evidence,the major differential diagnosis for a third ventricle includes arachnoid cyst,cystic neoplasm,and dermoid cyst.The differential diagnosis of different third ventricle masses based on different sequences has been mentioned in Table 1.Arachnoid cysts often appear less lobulated and follow a signal intensity patterns similar to those of cerebrospinal fluid with all MR pulse sequences including DWI and FLAIR.Cystic neoplasms,such as cystic ependymoma and cystic medulloblastoma,have a varied appearance on imaging due to the varying degrees of necrosis,calcification,and hemorrhage.The solid component of these lesions often shows heterogeneous contrast enhancement and restriction on DWI.Dermoid cysts are similar to epidermoid cysts,as both are lined by stratified squamous epithelium.In the context of imaging,dermoid cysts show a hyperintense signal on T1-weighted images while they appear as well-defined low attenuating (fat density) lobulated masses on CT scan.
The patient underwent craniotomy coupled with intra-hemisphere excision of the tumor.The procedure was uneventful.The patient was administered levetiracetam 500 mg twice a day.The patient is currently doing well.The diagnosis of malignant transformation of an epidermoid cyst arising from the third ventricle is challenging.Our key strengths involved our multidisciplinary approach in diagnosing,treating,and managing the patient.Non-invasive imaging modalities such as MR spectroscopy helped us confirm the diagnosis of a malignant epidermoid cyst from the third ventricle.
CONCLUSION
We have presented a rare case of a third ventricular lesion presumed to be an epidermoid tumor as seen on MRI.The use of multimodality imaging can help radiologists diagnose uncommon tumors in unusual sites.The combination of CT,MRI,and MR spectroscopy was useful in confirming the diagnosis of a malignant epidermoid cyst arising from the third ventricle,an unusual site in routine practice.
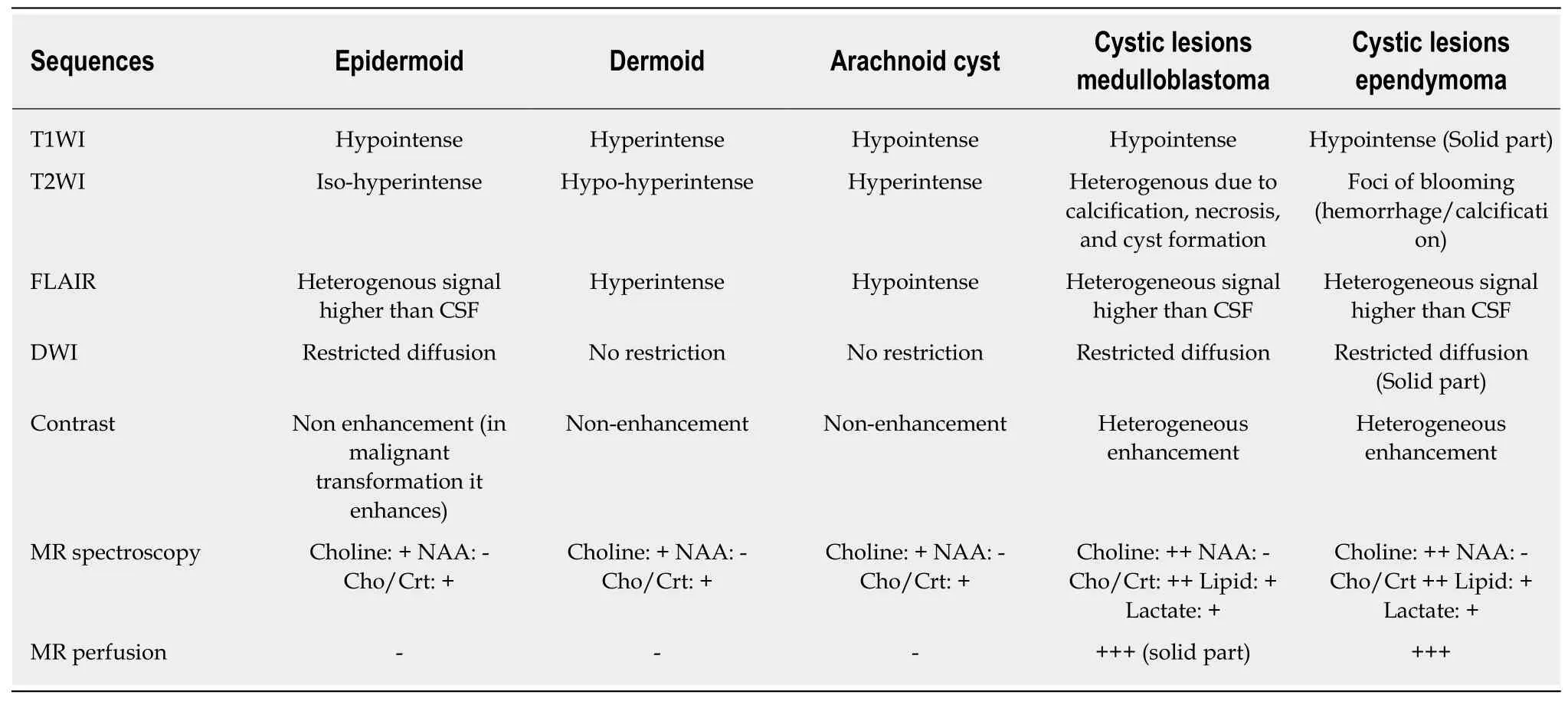
Table 1 Differential imaging considerations
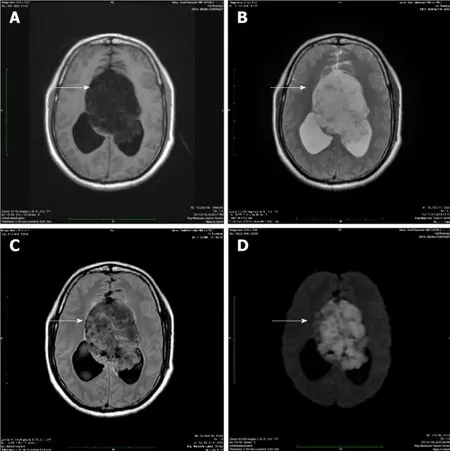
Figure 3 Magnetic resonance imaging.
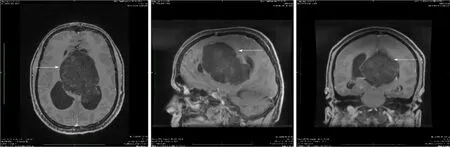
Figure 4 Minimal peripheral enhancement without any demonstrable solid enhancing component.
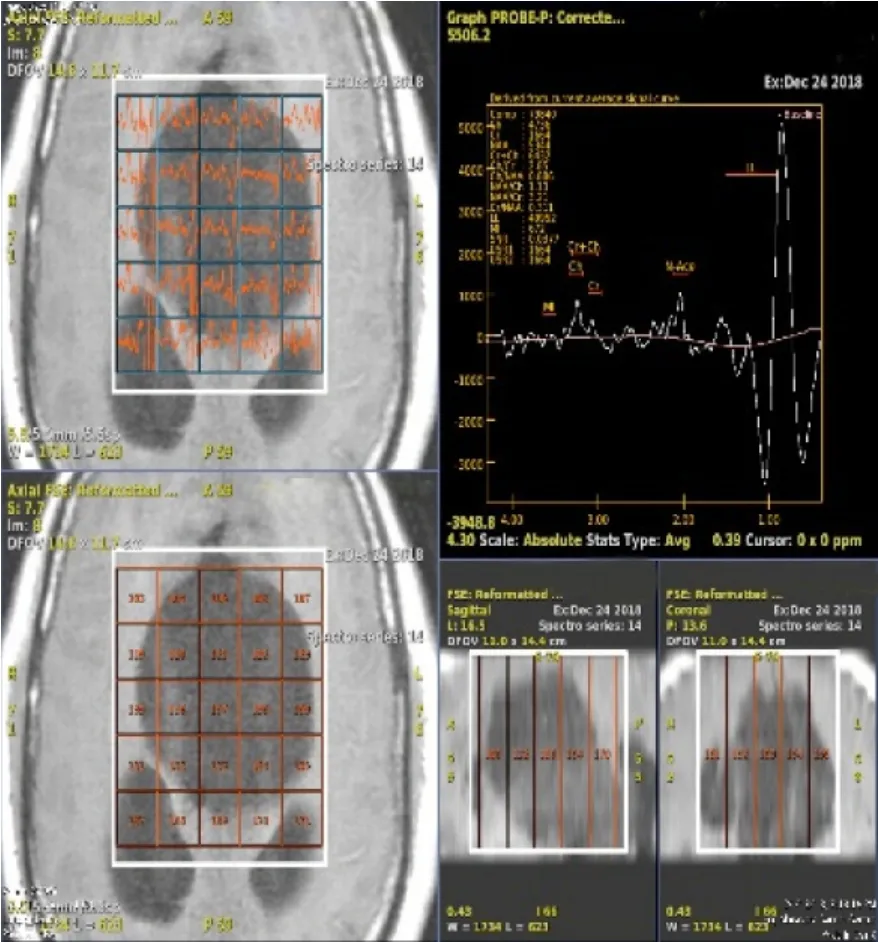
Figure 5 MR spectroscopy.
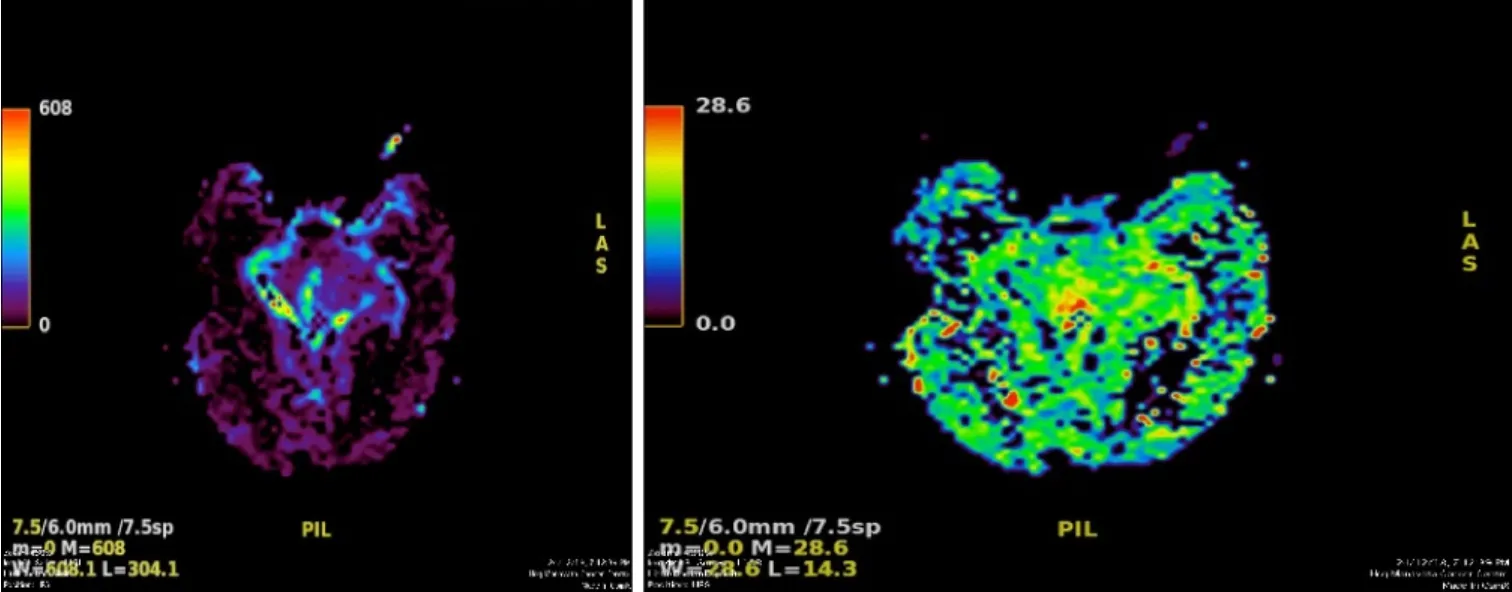
Figure 6 MR perfusion derived relative cerebral blood volume maps demonstrate heterogeneous perfusion abnormalities.
ACKNOWLEDGEMENTS
We would like to thank Mr.Lyndon Fernandes for his medical writing assistance.