
Effects of moxibustion on cancer-related fatigue: a meta-analysis
2019-06-28 12:27:28YuanJiaSiYuanYangLiMinGuoXueBaiYaNanWangFanJieMeng
TMR Non-Drug Therapy 2019年2期
Yuan Jia, Si-Yuan Yang, Li-Min Guo, Xue Bai, Ya-Nan Wang, Fan-Jie Meng, *
?
Effects of moxibustion on cancer-related fatigue: a meta-analysis
Yuan Jia1, Si-Yuan Yang1, Li-Min Guo1, Xue Bai1, Ya-Nan Wang2, Fan-Jie Meng1, *
1Tianjin University of Traditional Chinese Medicine, Tianjin, 300193, China.2Chief Nurse, Department of Oncology, First Affiliated Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, 300193, China.
To systematically evaluate the efficacy of moxibustion in the treatment of cancer-related fatigue (CRF).Randomized controlled trials (RCTs) using moxibustion to treat cancer-related fatigue in Cochrane Library, PubMed, China Knowledge Network, Wanfang and VIP databases were searched. Two reviewers independently searched, reviewed the literature, extracted data, and evaluated the methodological quality. RevMan5.3 software was used for meta-analysis.A total of 942 patients were included in 11 RCTs. The meta-analysis results showed that moxibustion can reduce fatigue score [MD = -2.04, 95% CI (-4.06, -0.33),< 0.001], improve the score of quality of life QLQ-C30 [(MD = 8.44, 95% CI (1.85, 15.03),< 0.001], also boost the number of differentiation antigen of T cells , such as CD3 [MD = 7.82, 95% CI (3.14, 12.49),= 0.01], CD8 [MD = -3.15, 95% CI (-11.36, 5.06),< 0.001], and the number of NK cells [MD = 5.88, 95% CI (3.56, 8.20),= 0.01].Moxibustion can improve the degree of CRF, improve the quality of life and enhance immune function.
Moxibustion, Cancer-related fatigue, Systematic review, Meta-analysis
Moxibustion can improve cancer-related fatigue (CRF) and enhance immune function. With the advantages of simplicity, convenient, efficacy, inexpensiveness, and lack of side effects, moxibustion appeared to be efficacious auxiliary therapeutic method for CRF.
The conclusion has some limitations as there exist few but rigorous randomized controlled trials and no trials in English, they were all from China. Much more high-quality studies with adequate design and power are in need urgently to confirm the therapeutic value of moxibustion for cancer-related fatigue profoundly.

CRF, Cancer-related fatigue; NCCN, National Comprehensive Cancer Network; TCM, Traditional Chinese medicine; QOL, Quality of life.
The authors declare that there is no conflict of interests regarding the publication of this paper.
Chang Liu
Introduction
Pain has been listed as the fifth vital sign after respiration, pulse, blood pressure, and body Cancer-related fatigue (CRF) is known as the "6th largest vital sign" and is one of the most common symptoms in patients with malignant tumors. The National Comprehensive Cancer Network (NCCN) Guide to 2018 defines CRF as "a disappointing, frustrating, persistent, subjective fatigue sensation caused by a tumor or anti-tumor treatment that is not proportional to physical activity [1]." And the sense of exhaustion, including physical, emotional and cognitive aspects, interfere with the daily activities and functions of patients." CRF can occur before and during treatment of the tumor, and it is aggravated during chemoradiotherapy, hormone or biological therapy. According to statistics, about 80% of patients receiving chemoradiotherapy have experienced fatigue, and the incidence of CRF in patients with distant metastases exceeds 75 %. Studies have shown that the fatigue status of tumor survivors can last for five years or more after the end of treatment [2]. CRF seriously affects the quality of life (QOL) of patients with cancer. Compared with the symptoms of pain, nausea and vomiting that can be controlled by drugs, CRF may be the most painful symptom caused by tumor and tumor treatment, but it is still clinically. There is no standard treatment plan.
The mechanism of CRF is still unclear. The etiology of CRF is complex, which may relate to tumor burden, physical state, treatment, cardiopulmonary dysfunction, myelosuppression, endocrine disorders, immune function decline or mental psychology. The main symptoms of CRF were fatigue, lack of energy, and lack of interest in the activities involved, similar to the "", the clinical manifestations of a consumptive disease in Chinese medicine [3]. Chinese medicine believes that tired is a general term for a variety of chronic weakness syndromes with visceral dysfunction, Qi (vital force that forms part of living entity in traditional Chinese culture.) and Yin (In Chinese philosophy, Yin and Yang is a concept of dualism describing how opposite forces depend on and give rise to each other) dysregulation, long-term illness and five-internal organs weakness as the main clinical manifestation. Moxibustion, using Moxa as the main material, directly or indirectly stimulates the acupuncture points to exert the functions of Qi, activate blood circulation, warm meridians and collaterals, reduce swelling and dispersing, warm the yang, and balance yin and yang [4]. Moxibustion has been receiving acknowledgements worldwide step by step in the treatment of CRF [5-6]. To date, although several published reviews and clinical trials focusing on acupuncture and moxibustion for CRF were available, we urgently require highly persuasive evidence. Therefore, a meta-analysis was conducted to assess the effectiveness of moxibustion in treatment of CRF.
Method
Search strategy and study selection
China Knowledge Network, Wanfang, VIP, the Cochrane Library and PubMed databases searches were carried out from their inception to October 2018 to identify all published and unpublished RCTs. The search uses the combination of subject words and free words, and references are tracked to reduce missing. The search strategy is as following: P: Tumor patients OR cancer patients OR cancer-related fatigue OR fatigue; I: Moxibustion OR direct moxibustion OR indirect moxibustion OR isolation ginger moxibustion OR isolation garlic moxibustion OR needle warming moxibustion OR wheat-moxibustion OR mugwort stick OR Chinese medicine external treatment method; S: Randomized controlled trial).
Literature screening and exclusion criteria
Inclusion criteria (1) type of research: Randomized controlled trials. (2) research object: Age ≥ 18 years old; cancer-induced fatigue is based on a scale of 0 to 10. The higher the score, the higher the fatigue (0 is no fatigue, 10 is the most severe CRF that can be imagined).
Interventions
Experimental group: the intervention measures are simple moxibustion or moxibustion combined with conventional treatment [simple Western medicine symptomatic treatment, traditional Chinese medicine (TCM) treatment or supportive treatment], moxibustion is not limited, such as wheat grain moxibustion, ginger moxibustion, thunder fire moxibustion, heat-sensitive moxibustion,The standardized acupuncture point locations had been used in previous research suggesting a therapeutic effect such as Guanyuan (CV4), Qihai (CV6), Zusanli (ST36) and Dazhui (GV14) points. The moxibustion was conducted 3 times a week or once every other day last 1-3 months. Control group: the control group received routine care and health education or conventional medicine if necessary.
Exclusion Criteria
Documents satisfying one of the following conditions were excluded: random assignment method was unknown; original text was not available through various channels; abstract provided insufficient information; statistical method was incorrect; repeatedly published articles; review.
Outcome indicators
Fatigue: the fatigue was evaluated using fatigue score. The scale has 2 items, measured from four dimensions: behavior, emotional meaning, feeling, and cognitive emotion. In each comment, the score of each item ranges from 0 (no fatigue) to 10 (most severe). The total score divided by 22 is the fatigue score. The higher the score, the more fatigue. Usually divided into 3 levels, namely: score 0 ~ 3 is divided into no fatigue or mild fatigue, 4 ~ 6 is divided into moderate fatigue, more than 7 is divided into severe fatigue. The patient reference scale entry is scored according to its own situation. After completion, the observer calculates the total score and the average score and records. QLQ-C30 and the KPS were used to evaluate the change of QOL. The number changes of immune-system cellular antigen such as CD3, CD4, CD8 and NK cells were used for immune function evaluation.
Filing and data extraction of literature
Use Note Express to remove duplicate documents; depending on the screening criteria, two researchers independently read the title and the abstract for the initial screening; after reading the entire text, the two researchers read independently to remove the documents that do not comply with the standards. The screening results were inconsistent and resolved through discussion. If the discussion not is able to reach an agreement, the third party will make a ruling; two researchers carefully read and independently extracted key information from the study, containing the author, year, number of studies, and outcome measures. See Table 1 for details.

Table 1 General information
Note: QOL: Quality of life.
Assessment for risk of bias and grading the quality of evidence
Methodological quality evaluation of the included studies was performed using the bias risk assessment tool provided by the Cochrane Handbook for Systematic Reviews of Interventions 5.1.0 [7]. The evaluation includes: (1) random sequence generation; (2) allocation concealment; (3) blind method; (4) whether to describe loss of follow-up; (5) selective reporting of research results; (6) other sources of bias. The quality level of the literature that satisfies the standard is A grade, the risk of bias is low, and the research quality is high; some meet the above criteria, the quality grade is B grade, suggesting that the possibility of bias is moderate; the one who does not meet the standard at all, the quality grade is C grade. For the C grade, there is a high risk of bias and the quality of the research is low. This study only included literature with a grade A or B of literature quality.
Data analysis
The meta-analysis of the included randomized controlled trials was performed using Rev Man 5.3 software. The binary data was measured using RR and 95% CI, and the continuity data was measured using MD/SMD and 95% CI [8]. The inter-study heterogeneity was tested by Cochrane Q test and I2:> 0.1, I2< 50%, indicating homogeneity between studies, meta-analysis using fixed effect model; if≤ 0.1, I2≥ 50%, it indicates that there is heterogeneity and data combination is performed using a random effects model.
Results
Search results
A total of 64 related articles were retrieved, including 49 Chinese literature and 14 English literature. Note Express software was used to remove duplicates. Through sifting layer upon layer strictly, 11 studies were included ultimately [7-17], with 942 patients. The literature screening process and results are shown in Figure 1.
Basic characteristics and methodological quality evaluation of the included literatures
The basic characteristics of the 11 included studies are shown in Table 1. According to the Cochrane Hand-book 5.1.0 evaluation criteria, the quality of the included literatures was evaluated. The results showed that 5 of the 11 studies reported the use of random number table method. The rests mentioned “random”, but not described the methods. All the 11 studies did not mention the allocation sequence method and the blind method, so it was rated as high risk; all the 11 cases were rated as low risk without loss of follow-up; the data in the 11 studies is complete and is rated as low risk; the final quality evaluation results of 11 studies were all grade B (Figure 2).
Meta-analysis results
Fatigue
11 articles [9-19] reported the effect of moxibustion on the fatigue of CRF patients. 5 articles [ 12, 13, 14, 18,19] reported the effect of moxibustion on reducing fatigue scores, and 7 articles [8, 9,10, 12, 14, 15, 16] reported the change of fatigue degree in moxibustion. The results showed that moxibustion can reduce the cancer-related fatigue score [MD = -2.04, 95% CI (-4.06, -0.33),< 0.001] (Figure 3), but has no effects on the fatigue degree [OR = 2.27, 95% CI (1.63, 3.16),= 0.06] (Figure 4). I2> 50%, random model was adopted.
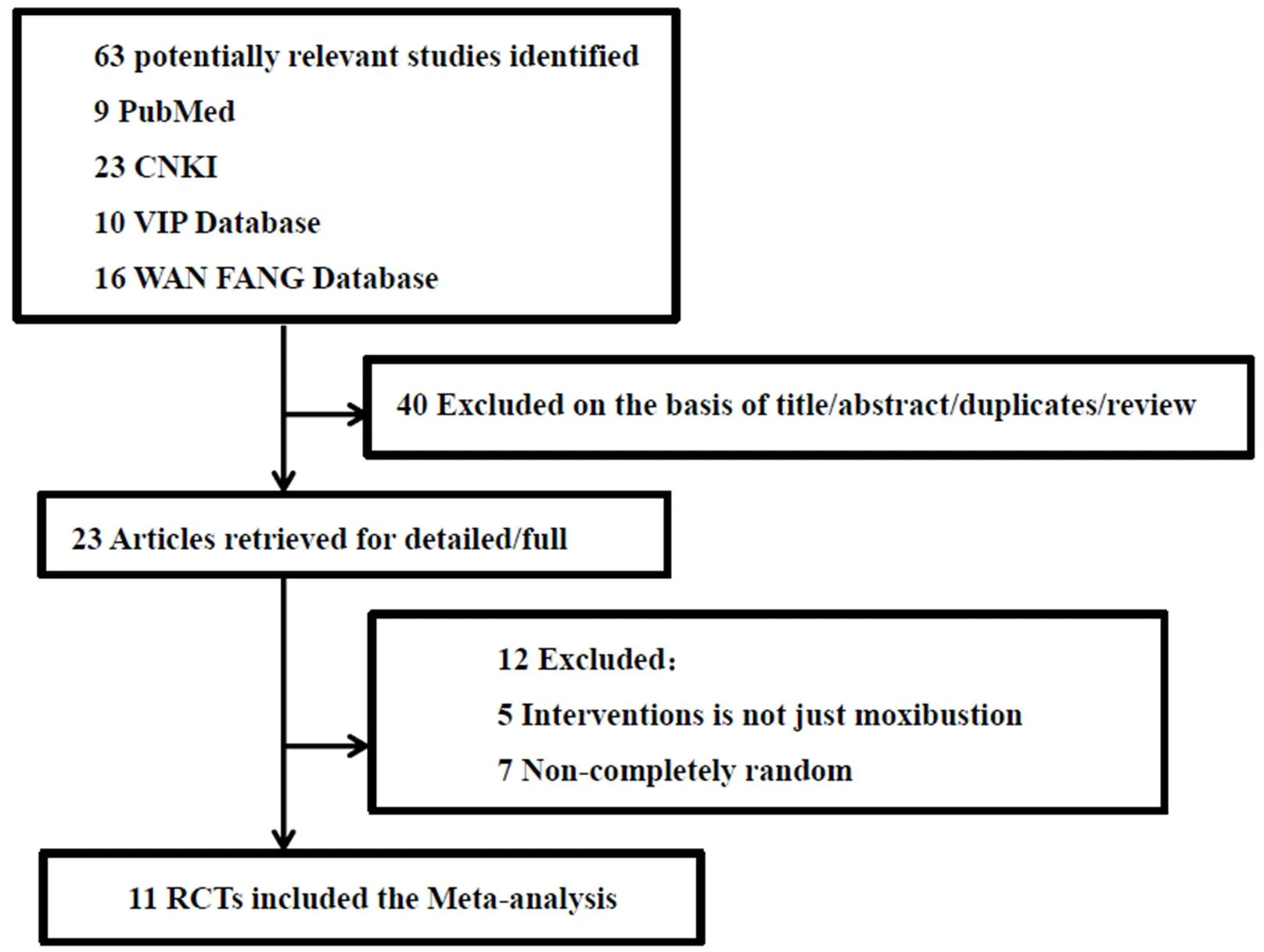
Figure 1 Literature screening flow chart
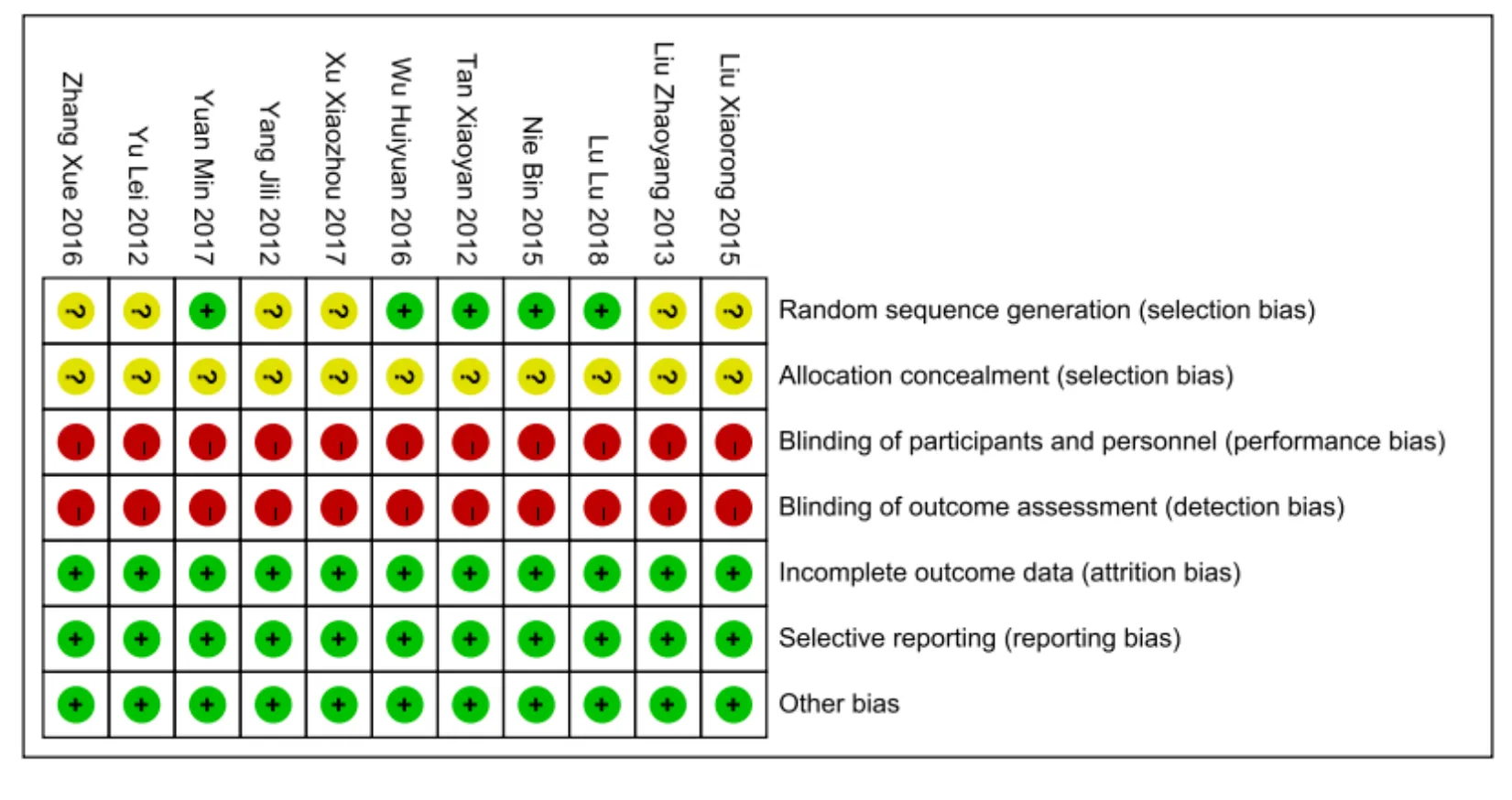
Figure 2 Methodological quality evaluation
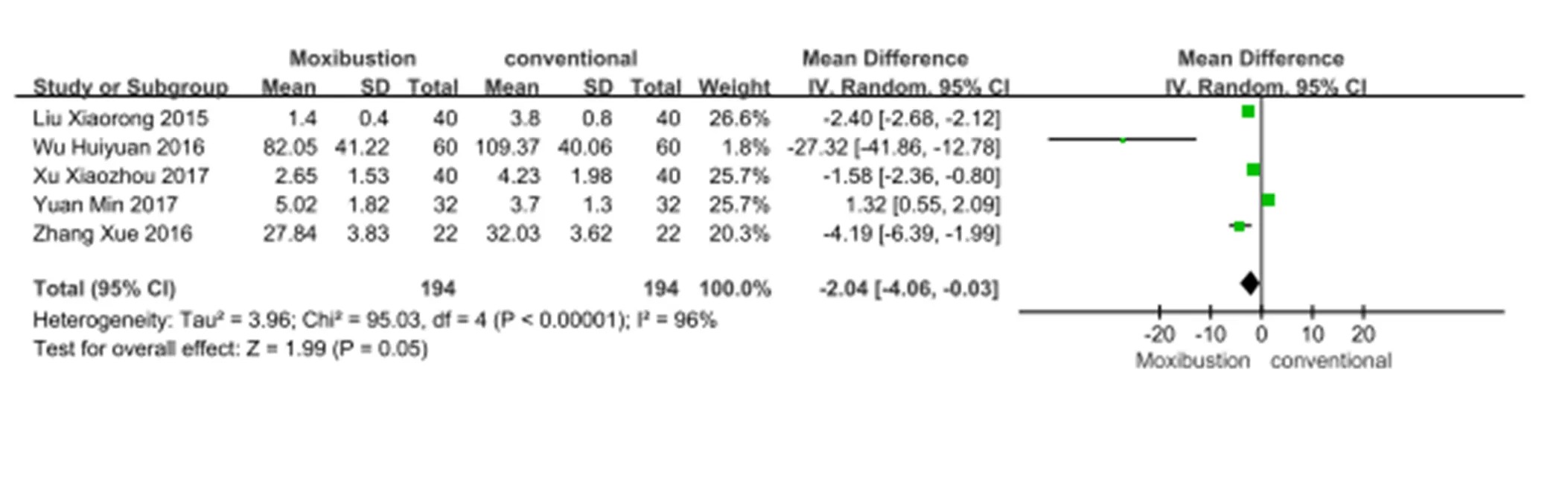
Figure 3 Forest map of cancer-related fatigue score
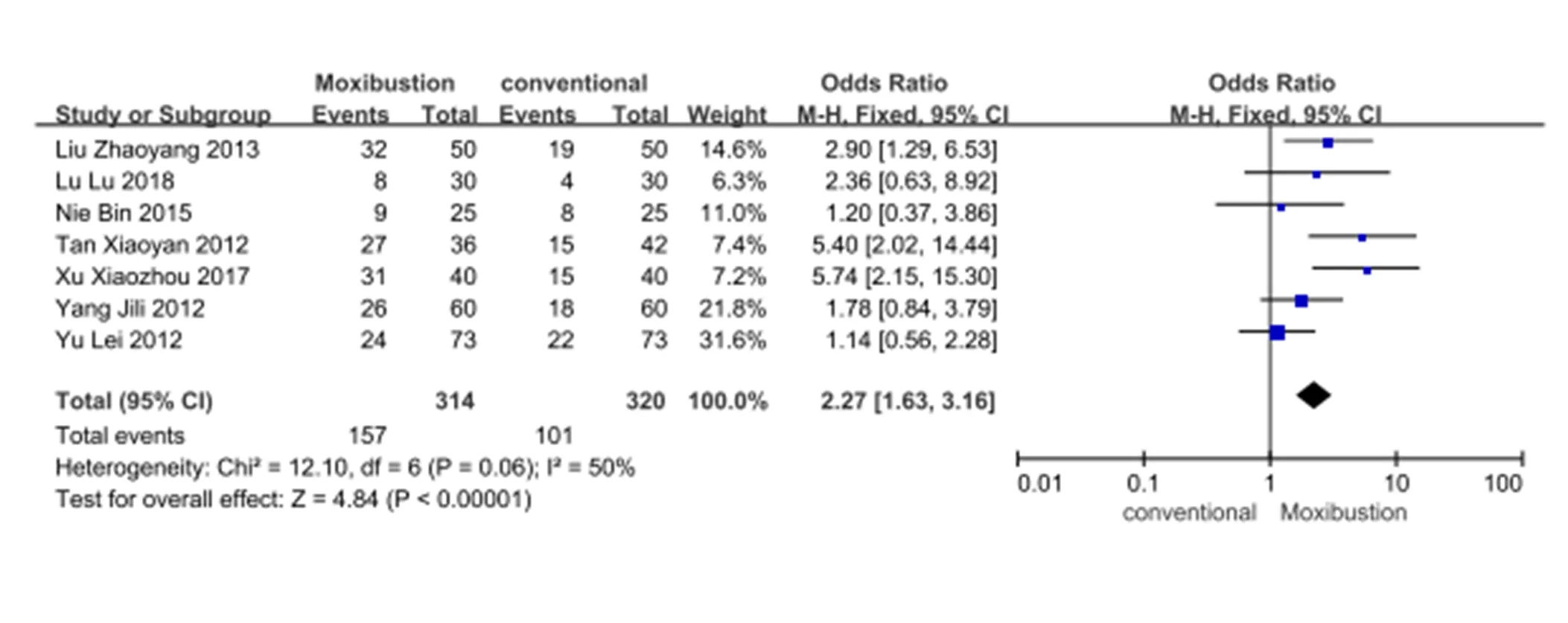
Figure 4 Forest map of fatigue degree
Quality of life
Seven articles [11, 12, 13, 14, 15, 16,18] reported the QLO after moxibustion intervention. Meta-analysis showed that moxibustion can improve CRF patients’ life quality as the QLQ-C30 score were improved [MD = 8.44, 95% CI (1.85, 15.03),< 0.001] and I2> 50%, random effects model was used (Figure 5); the KPS changes [OR = 2.31, 95% CI (1.15, 4.60),= 0.54] and KPS score [MD = 6.50, 95% CI (4.32, 8.68),= 0.20] were showed in Figure 6 and Figure 7. I2< 50%,fixed effect model was adopted.
Immune function
Three articles [11, 12, 19] reported the effects of moxibustion on differentiation antigen of T cells including CD3, CD4, CD8 and NK cells in patients with CRF. The results showed that the number of differentiation antigen of T cells including CD3 [MD = 7.82, 95% CI (3.14, 12.49),= 0.01] and CD8 [MD = -3.15, 95% CI (-11.36, 5.06),< 0.001] as well as the number of NK cells [MD = 5.88, 95% CI (3.56, 8.20),= 0.01] were increased (Figure 8). I2> 50%, random model was adopted.
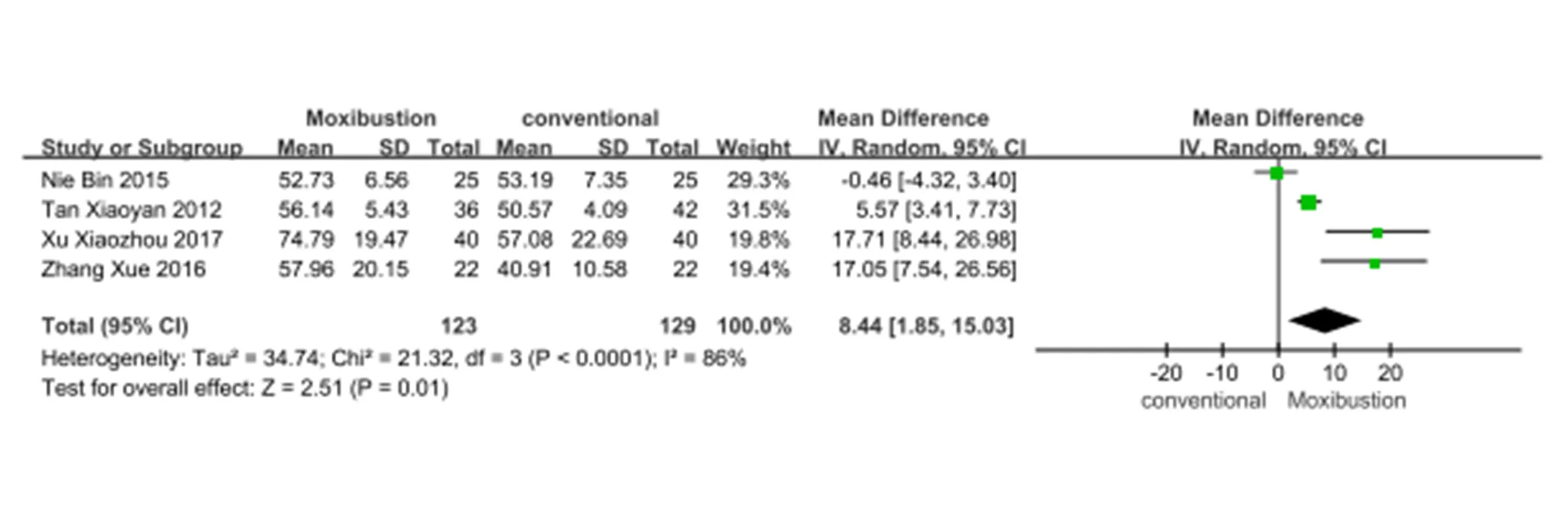
Figure 5 Forest map of quality of life
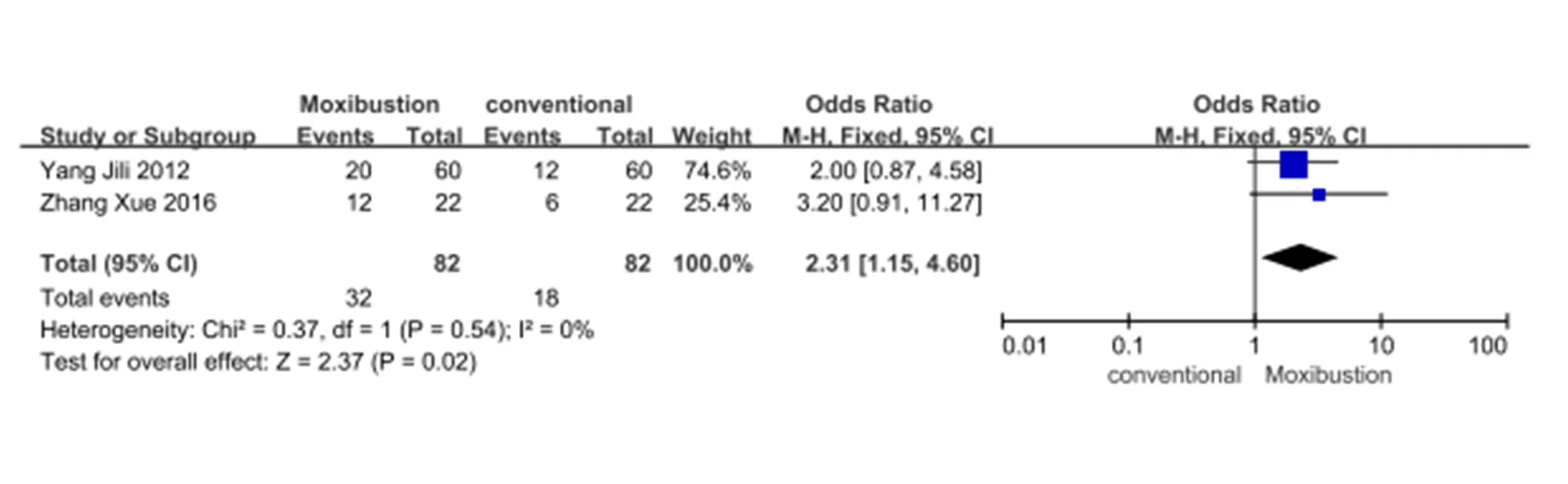
Figure 6 Forest map of KPS changes
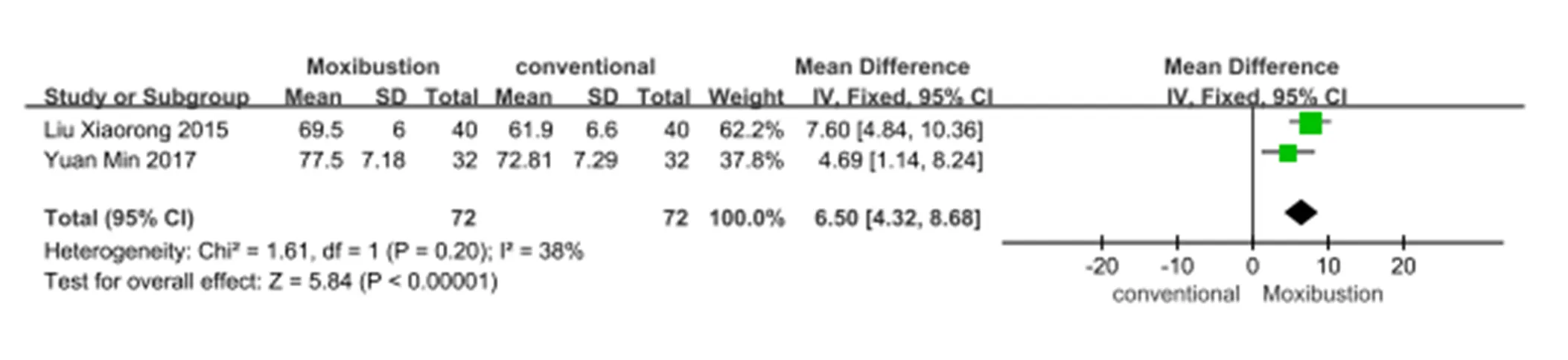
Figure 7 Forest map of KPS score
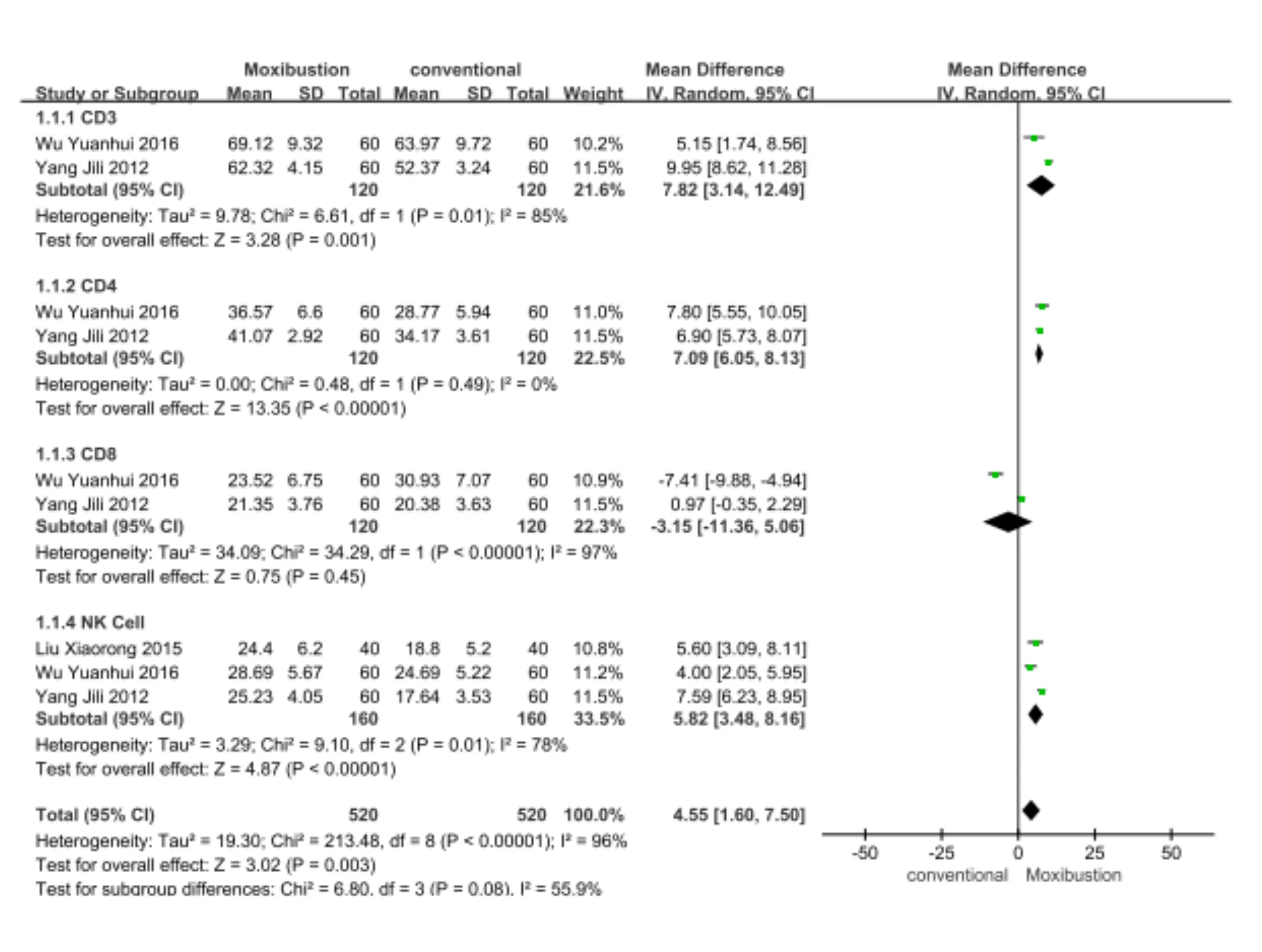
Figure 8 Forest map of immune-system cellular antigen and NK cells
Discussion
Treatments for Cancer-related fatigue currently namely includes non-pharmacological treatment and drug treatment. It has reported that non-pharmacological interventions are more effective than drug interventions [20]. NCCN (2018) CRF guidelines point out that exercise is an effective way to improve CRF [1]. Aerobic exercise can stimulate the secretion of β-endorphin from the pituitary gland. The nervous system produces micro-electric stimulation, which can relieve muscle tension and depression, relieve fatigue. A meta-analysis results show that psychological, sports, psychological and sports joint intervention are more effective for CRF, which recommend exercise and psychological intervention as the first-line treatment of CRF; family function and sleep cognitive behavioral therapy can effectively alleviate the psychological stress of patients, improve the quality of sleep, improve the fatigue of cervical cancer patients, and improve the QOL [21-23]. Transcutaneous electrical nerve stimulation can also effectively improve the fatigue of cancer patients [24]. However, most patients are weakness, and lack of knowledge of CRF, resulting in poor exercise compliance; what is more, psychological intervention, family function and sleep interventions and other methods have no uniform standards, and the effects are affected by nurses' human resources, family members' education level, hospital environment,Central stimulants and corticosteroids are the common drug treatments for patients with CRF. But the effects are weak and the adverse reactions such as blood pressure, cardiovascular risk, fever, and muscle breakdown cannot be ignored [22-24].
TCM methods such as moxibustion, soup [25], acupuncture [26], Chinese medicine foot bath [27],has been widely used in the treatment of cancer-related fatigue with good curative effects. However, for its time-consuming and painful characters, it is difficult to be widely accepted. Benefits of acupuncture treatment for cancer-related fatigue has been proved, but for it is an invasive operation, most patients don’t want to try it. TCM foot bath, as an auxiliary treatment, is easy to operate, but its effect is weak.
An ancient book of Chinese medicine formed during 722 BC ~ 221 BC namedhas recorded that "The needle is not the place, the place of moxibustion". Song Diancai had mentioned that "for life-saving, moxibustion is the most important method, followed by herbs, the aconite roots came the third. Bian Xinshu has recorded that " moxibustion can be used for any disease that is not well treated by medicine or acupuncture. The ancient literature classifies the pathogenesis of CRF as follows: congenital deficiency, acquired dysfunction,Yin and Yang imbalance, Qi and blood fluid loss, visceral gas deficiency, overwork injury, diet, emotional inconsistency, sinister poisoning,Therefore, for CRF treatment, it should balance the Yin and Yang, supplement the Qi and blood, tonify spleen and kidney [28]. The benefit of acupuncture, decoction, acupoint has been proved in the treatment of CRF, especially when combined with modern medicine [29]. This meta-analysis found that moxibustion could reduce fatigue score [MD = -2.04, 95% CI (-4.06, -0.33),< 0.001], but had no effects on the change of fatigue degree [OR = 2.27, 95% CI (1.63, 3.16),= 0.06]. The reason for the analysis may be different from the scale used between the different studies, and the selected acupoints are different. It could improve QOL in some extent as the QLQ-C30 score was improved [MD = 8.44, 95% CI (1.85, 15.03),< 0.001], but had no significant effects on the KPS score [MD = 6.50, 95% CI (4.32, 8.68),= 0.2]. Moxibustion had some effects on immune function as the number of differentiation antigen of T cells, including CD3 [MD = 7.82, 95% CI (3.14, 12.49),= 0.01], CD8 [MD = -3.15, 95% CI (-11.36, 5.06),< 0.001] and NK cells [MD = 5.88, 95% CI (3.56, 8.20),= 0.01] were increased after moxibustion. The clinical efficacy rate of moxibustion intervention has improved after moxibustion [OR = 3.34, 95% CI (1.30, 8.62)], but the difference had not statistical significance (= 0. 09). Reason for analysis: the KPS scale focuses on the assessment of physical status. Patients are affected by the disease itself, and even if the fatigue is improved, the physical recovery may be relatively slow.
In this study Guanyuan (CV4), Qihai (CV6), Zusanli (ST36) and Dazhui (GV14) were the most used acupoints. These acupoints have the effect of cultivating the yuan, strengthening the yang, nourishing the spleen and tonifying the spleen. The essential points, with the help of moxibustion, make the subcutaneous local capillaries dilate, improve the body's blood circulation, warm the meridians, Qi and blood, cultivate vitality, enhance immunity and more prominent. Some studies found that the strength of immune function is closely related to the incidence of CRF [30-33]. The enhancement of immune function can strengthen the body and enhance the anti-fatigue degree. The moxibustion Shenque (CV8) point can strengthen the spleen and kidney, and restore the body, thus improving the body immune function. Studies have shown that fatigue is associated with tumor-related symptoms such as sleep, pain, anxiety, and nutrition [30]. Tumor patients have decreased fatigue, increased immune function, pain and anxiety relief, improved sleep, and increased nutrition, thereby improving their QOL.
This study shows that moxibustion can improve the degree of CRF, reduce fatigue score, improve their QOL, and enhance their immune function. But the conclusion has some limitations as there exist few but rigorous RCTs and no trials in English, they were all from China. Much more high-quality studies with adequate design and power are in need urgently, and on account of methodological limitation, much more systematic investigations in depth are also necessary to confirm the therapeutic value of moxibustion for CRF profoundly.
1. NCCN Clinical Practice Guidelines in Oncology: Cancer-Related Fatigue.
2. Xu YM, Cheng C, Yang G,Clinical characteristics of cancer-related fatigue and TCM syndromes in patients with lung cancer. Zhonghua J Tradit Chin Med 2017, 32: 4746-4749.
3. Wang BQ, Wang XH, Li ZG. Research progress in the treatment of lung cancer with traditional Chinese medicine. J Tradit Chin Med 2018, 33: 371-374.
4. Wang YT, Wang ST. Research progress in the application of moxibustion in tumor therapy. J Guangxi Univer Tradit Chin Med 2018, 21: 76-78.
5. Sun C. Clinical study on moxibustion for treatment of cancer-related fatigue. Anhui University of Tradit Chin Med 2018, 12: 334-338.
6. Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions version London: The Cochrane Collaboration, 2011.
7. Cochrane handbook for systematic reviews of interventions. Chichester: Wiley-Blackwell, 2008.
8. Yu L, Jing NC, Yang JL,Analysis of clinical characteristics of cancer-related fatigue and observation of the effect of moxibustion treatment. Chin Med Guide 2012, 10: 591- 593.
9. Liu CY, Bao QH, Liang ZW. Effect of moxibustion on cancer-related fatigue in patients with lung cancer chemotherapy. Massage Rehabilitation Med 2013, 22: 155.
10. Yang JL, Yu L, Xu L,Therapeutic effect of moxibustion on cancer-related fatigue in elderly patients with advanced cancer. Chin J Gerontol 2012, 32: 4408- 4410.
11. Liu XR. Observation on the therapeutic effect of moxibustion on cancer-related fatigue in elderly patients with advanced tumors. Sichuan J Tradit Chin Med 2015, 33: 181-183.
12. Xu XZ, Zhu YF, Xia LM. Clinical study on moxibustion for treatment of spleen and kidney deficiency type cancerous fatigue. J Tradit Chin Med and Pharm 2017, 29: 712-715.
13. Yuan M, Zhang GB, Li M,Treatment of cancer due to chemotherapy in patients with colorectal cancer after chemotherapy. J Nurs 2017, 32: 8-10.
14. Nie B, Li ZM, Zhong XM,Clinical observation of Fuyang fire moxibustion on treatment of yang deficiency type cancerous fatigue. Shanghai J Acu and Mox 2015, 34: 527-530.
15. Tan XY, Liu ZH. Clinical study on the treatment of cancer-related fatigue in patients with advanced cancer by abdominal warm moxibustion. J Tradit Chin Med 2012, 27: 273-274.
16. Lu L, Li WH, Guo XC,Zhen Ci Yan Jiu 2018, 43: 110-113.
17. Zhang X, Huang WJ, Xu TS. Effects of wheat moxibustion on cancer-related fatigue and quality of life in patients with malignant tumors. Shanghai J Acu and Mox 2016, 35: 659-662.
18. Wu HY, Guo HF, Xu T,Effect of thermal moxibustion intervention on cancer-related fatigue in patients with advanced lung cancer. J Clin Acu and Mox 2016, 32: 52-54.
19. Mustian KM, Alfano CM, Heckler C,Comparison of pharmaceutical, psychological, and exercise treatments for cancer-related fatigue: a meta-analysis. JAMA Oncol 2017, 3: 961- 968.
20. Huang HL, Li J. The effect of spouse home visit on emotional status and cancer-related fatigue in patients with cervical cancer. Contemp Nursing 2018, 25: 109-112.
21. Xie XD, Zhang YY. The latest development of cancer-related fatigue-Interpretation of NCCN guidelines for cancer-related fatigue. Chin J Clin Oncol 2018, 45: 817-820.
22. Fu T, Guang HJ, Gao XZ. Percutaneous nerve electrical stimulation for fatigue caused by chemotherapy for cervical cancer. Medicine 2018, 97: e12020.
23. Yu JH, Zhao G, Feng L,Chinese medicine intervention for lung-yin deficiency syndrome due to cancer fatigue. J Tradit Chin Med 2018, 33: 2060-2063.
24. Zhou J, Tian HQ, Zeng BY,Clinical observation of fatigue-induced three-needle treatment for cancer-related fatigue in patients with breast cancer. J Tradit Chin Medi 2018, 33: 950-953.
25. Tang MF, Lu Y. Effect of moxibustion combined with traditional Chinese medicine foot bath on cancer-related fatigue in patients with gastrointestinal cancer chemotherapy. Integr Chin West Med Nurs 2018, 4: 63-66.
26. Chen LY. A study of the academic thoughts and fangzheng of zhongjing's theory of treating fiction. Beijing Univer Chin Med 2015, 23: 56-61.
27. Zou JX, Pan XF. Research progress of Chinese medicine intervention on cancer-related fatigue. Hunan J Tradit Chin Med 2017, 33: 154-156.
28. Cao Y. Effect of acupoint moxibustion on cancer-related fatigue in patients with cervical cancer concurrent radiotherapy and chemotherapy. Nanjing Univer Tradit Chin Med 2017, 56: 23-31.
29. Lin W, Hu Y. Cancer-related fatigue: conceptual analysis. Foreign Med Nurs Sci 2005, 77: 318-321.
30. Zhu GD, Zhang B, Jiang FN,Shenqi Fuzheng injection ameliorates fatigue-like behavior in mouse models of cancer-related fatigue. Biomedicine Pharmaco 2019, 11: 111.
10.12032/TMRND201902013
Jia Y, Yang SY, Guo LM,. Effects of moxibustion on cancer-related fatigue: a meta-analysis. TMR Non-Drug Therapy 2019, 2(2): 62-70.
3 June 2019,
Submitted: 12 March 2019,
Online: 6 June 2019.
*Corresponding to:Fan-Jie Meng, Tianjin University of Traditional Chinese Medicine, 314 Anshanxi Road, Nankai District, 300193, Tianjin, China. Email: mfj1127@126.com
- TMR Non-Drug Therapy的其它文章
- The effects of TCM nursing intervention on the life quality of cancer patients with pain: a review of recent research
- Kinematic improvement after the external-application herbs combine rehabilitation in upper-limb spasticity due to stroke
- Non-drug interventions for cancer-related fatigue: an updated review
- Kinesio tape in the treatment of postoperative lymphedema of breast cancer
- Progress in clinical application of Kinesio taping