
Community-acquired pneumonia with Acinetobacter radioresistens bacteremia in an immunocompetent host: A case report
2019-07-13 01:45:26YiHernTanLishanJessicaQuahHumairaShafi
Yi Hern Tan, Lishan Jessica Quah, Humaira Shafi
1Department of Respiratory and Critical Care Medicine, Changi General Hospital, 529889, Singapore
2Department of Infectious Diseases, Changi General Hospital, 529889, Singapore
Keywords:Case report Acinetobacter baumanii BlaOXA-23 gene Carbapenem-hydrolyzing oxacillinases Rare respiratory infections
ABSTRACT Rationale: Acinetobacter radioresistens is a non-fermentative Gram-negative coccobacillus that is environmentally ubiquitous and is an uncommon cause of pneumonia in an immunocompetent patient with no known chronic medical illness.Patient concerns: A middle-aged Asian male with a smoking history presented with fever and cough. Physical examination was unremarkable. Chest imaging was consistent with pulmonary parenchymal infection and blood culture grew Acinetobacter radioresistens.Diagnosis: Community acquired pneumonia with Acinetobacter radioresistens bacteremia.Interventions: The patient received a combination of intravenous and oral ampicillinsulbactam over 2 weeks.Outcomes: Repeat blood cultures showed resolution of bacteremia. Completion of antimicrobial treatment saw resolution of respiratory symptoms and radiological pneumonic changes.Lessons: Acinetobacter radioresistens causing community-acquired pneumonia in an immunocompetent host has never been described before. It may be a novel emerging infectious agent in pulmonary infections. Its clinical course in this immunocompetent patient appears to be relatively benign.
1. Introduction
Acintobacter species are aerobic, oxidase-negative, Gram-negative coccobacilli. There are more than 30 species belonging to this genus,of which Acinetobacter (A.) baumanii is most frequently isolated and well known for its ability to cause outbreaks in drug-resistant health care associated infections[1]. A. radioresistans, a less known species of this genus, is an environmentally ubiquitous organism. It may be present in hospital environments and has been isolated in a pseudooutbreak involving contamination of the pneumatic transport system of a hospital[2]. There have been 4 prior reports of its isolation from human clinical samples where it has caused respiratory tract infections and bacteraemia in immunocompromised hosts[3-6].Here, we describe an immunocompetent patient who presented with cough and fever. He was found to have A. radioresistens bacteraemia secondary to community-acquired pneumonia.
2. Case report
2.1. Presenting concerns
A 55-year-old male patient of Malay ethnicity with no known medical history presented to the emergency department with 2 weeks of cough that was productive of yellowish sputum. He had intermittent fever with temperatures up to 38 degrees Celsius.Associated symptoms included unintentional weight loss of 5 kilograms over 2 weeks with generalized lethargy and weakness.Review of systems was unremarkable. He worked as an aircraft technician and had a smoking history of 40 pack-years.
2.2. Clinical findings
Initial examination showed an alert, comfortable and thin-built patient. He was afebrile at presentation with a temperature of 37.2 ℃, blood pressure was 120/71 mmHg and heart rate was 98 beats per min. He was maintaining oxygen saturations of 96% to 100% on room air. Physical examination was unremarkable with normal lung sounds. Posteroanterior and lateral chest radiographs showed retrocardiac tubular densities that were indeterminate for early infective changes and may be prominent bronchovascular markings.
Initial blood investigations showed haemoglobin 12.0 g/dL, total white cell count 14.1×103/uL with 79% neutrophils, platelet count 595×103/uL. C-reactive protein was elevated at 59.7 mg/L. Serum procalcitonin was not elevated at 0.07 ug/L. Liver and renal function tests were within acceptable parameters. Blood cultures were drawn,and treatment commenced with empiric intravenous amoxicillinclavulanic acid 1.2 g thrice daily and oral clarithromycin 500 milligrams twice daily.
2.3. Diagnostic focus and assessment
One of the two blood cultures isolated A. radioresistens that was sensitive to ampicillin-sulbactam, ciprofloxacin, gentamicin and piperacillin-tazobactam. The pathogen was identified with MALDITOF MS (VITEK MS, bioMérieux, Inc) and antibiotic susceptibilities were evaluated with the VITEK 2 system (bioMérieux, Inc). A computed tomography scan of the thorax, abdomen and pelvis was performed to evaluate for the source of bacteraemia. The thorax sequences showed patchy ground-glass densities in the posterior basal segments of the bilateral lower lobes and anterior basal segment of the right lower lobe (Figure 1).
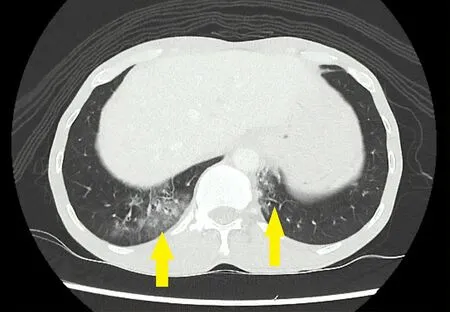
Figure 1. A 55-year-old man with fever and cough. Blood cultures showed Acinetobacter radioresistens. CT Thorax transverse section shows bilateral lower lobe ground-glass infiltrates and centrilobular nodules (arrows).
This was associated with tree-in-bud pattern centrilobular nodules with no cavitation. Background emphysematous changes were noted.The abdomen and pelvis sequences showed no other foci of infection.Sputum examination for acid fast bacilli smears and cultures were non-yielding. To evaluate for possible immunocompromised states,human immunodeficiency virus serological testing was performed and was negative. History, physical examination and clinical investigations did not suggest underlying undiagnosed autoimmune diseases or acquired immunodeficiencies.
2.4. Therapeutic focus and assessment
A repeat set of blood cultures drawn 2 d after the initial culture showed no persistent bacteraemia after initiation of antibiotics. The patient progressed favourably in the ward with good oral intake,remaining hemodynamically stable. His fever defervesced after 24 h.Antimicrobial therapy consisted of 1 week of intravenous ampicillinsulbactam 3 g 6 hourly followed by 1 week of oral ampicillinsulbactam 750 milligrams twice daily.
2.5. Follow-up and outcomes
An outpatient review 4 months after treatment saw clinical resolution of cough and sputum. A repeat computed tomography scan of the thorax performed 3 months following the initial presentation showed near complete resolution of the pulmonary ground glass opacities and tree-in-bud pattern centrilobular nodules seen in the initial scan (Figure 2). At 6 months from the initial evaluation, there was no evidence of any delayed presentation of autoimmune diseases, malignancies or acquired immunodeficiencies.
The patient returned to his prior physical fitness level and daily activities.
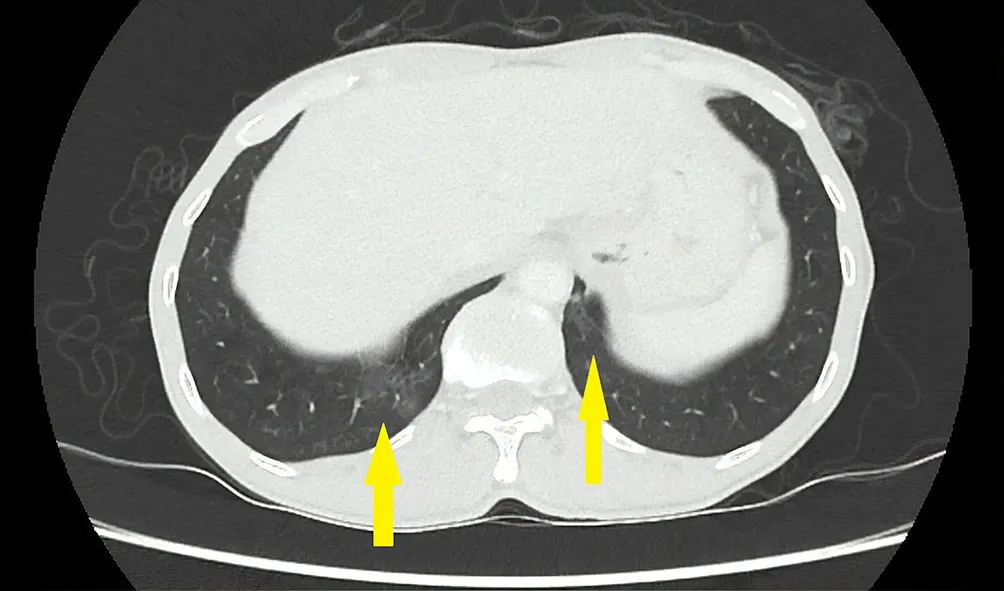
Figure 2. A 55-year-old man with fever and cough. Blood cultures showed Acinetobacter radioresistens. The patient received 2 weeks of ampicillinsulbactam. A repeat CT Thorax was performed 3 months after the initial scan. Transverse section shows near complete resolution of bilateral lower lobe ground-glass infiltrates and centrilobular nodules.
3. Discussion
Organisms from the genus Acinetobacter are described as Gramnegative, aerobic coccobacilli that are oxidase-negative and catalase-positive. They are environmentally ubiquitous and are possible emerging infective agents in the critically ill and immunocompromised patients[7]. A. radioresistens has been described as a commensal organism of the skin of healthy individuals and its role in causing disease in humans is unclear[8]. Communityacquired pneumonia with A. radioresistens bacteremia is rare, and to our knowledge, it has been reported in 4 case reports describing 5 patients who were immunocompromised[3-6]. The clinical samples that isolated A. radioresistens in these case reports were from blood and respiratory secretions. The clinical courses of these patients described were that of severe infections, with 2 resultant mortalities.
The significance of A. radioresistens as a human pathogen may lie in its ability to harbour a chromosomally encoded blaOXA-23oxacillinase gene, which may result in the expression of acquired carbapenemhydrolyzing oxacillinases. It is proposed that genetic exchange between A. radioresistens and A. baumanii via plasmids may occur in humans, thus leading to carbapenem resistance in A. baumanii.Carbapenem-hydrolyzing enzymes are well described as the main mechanism of carbapenem resistance in A. baumannii, which is a clinically significant pathogen in nosocomial infections[9]. However,A. radioresistens intrinsically carries the blaOXA-23gene, this organism is usually susceptible to carbapenems, suggesting that blaOXA-23is constitutionally expressed at low levels and may serve as a potential reservoir for drug-resistance[10].
This case report highlights the potential of A. radioresistens to cause symptomatic disease in an otherwise immunocompetent individual.The authors acknowledge the limitation and possibility that this organism may potentially be a contaminant in the blood culture given the growth in single bottle and the presence of organism in the environment. However, given the rarity of isolation of this organism in human clinical samples, we caution against dismissing its significance and would like to raise awareness on the potential evolving pathogenicity of this organism.
Conflict of interest statement
We declare that we have no conflict of interest.
 Asian Pacific Journal of Tropical Medicine2019年6期
Asian Pacific Journal of Tropical Medicine2019年6期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Optimized combinations of statins and azoles against Acanthamoeba trophozoites and cysts in vitro
- Anticancer activity of Mahonia leschenaultii methanolic root extract and berberine on Dalton’s ascitic lymphoma in mice
- Symptoms of dengue at the acute and post-infection stage in the Western Province, Sri Lanka: A cross-sectional study
- Epidemiology and immunodiagnostics of Strongyloides stercoralis infections among migrant workers in Malaysia
- Laboratory diagnosis of schistosomiasis mansoni: Current status and future trends