
Chest pain without a clue-ultrasound to rescue occult multiple myeloma: A case report
2020-01-04 07:59:06GopalChawlaNaveenDuttKunalDeokarVirenderKumarMeena
World Journal of Radiology 2019年12期
Gopal Chawla, Naveen Dutt, Kunal Deokar, Virender Kumar Meena
Gopal Chawla, Naveen Dutt, Kunal Deokar, Pulmonary, Critical Care and Sleep Medicine, All India Institute of Medical Sciences, Jodhpur 342008, Rajasthan, India
Virender Kumar Meena, Department of Radiodiagnosis, Geetanjali Medical College and Hospital, Udaipur 342005, India
Abstract
Key words: Case report; Ultrasound; Multiple myeloma; Chest pain
INTRODUCTION
Chest pain is one of the most common symptoms with which a patient presents to a doctor. Etiology is wide, and ranges from acute and life-threatening diseases like acute coronary syndrome and pulmonary embolism to conditions with favorable prognosis like myalgia and costochondritis. It is important to know the relevant etiologies and their respective frequencies.
Bone pain is one of the most common presentations of multiple myeloma (70%-80%), and 90% of cases will present with lumbar spine or rib pain. Plain films are only 80%-90% sensitive at detecting lytic bone lesions, due to an inability to detect lesions with less than 30%-50% trabecular bone loss. By the time this degree of sternal/rib bone loss occurs, patients are at high risk for fracture, which can result in serious complications such as flail chest and acute hypoxic respiratory failure.
Since early treatment with chemotherapy and zoledronic acid reduces vertebral fractures and skeletal events, multiple myeloma is an important disease to keep on a differential for persistent atypical chest pain, especially when anemia and renal injury is present.
CASE PRESENTATION
Chief complaints
A 50-year-old banker presented with complaints of chest pain for 2 mo.
History of present illness
Chest pain was parasternal, non-radiating and continuous in nature. There was no history of trauma, cough, breathlessness, loss of weight, loss of appetite or fever.
History of past illness
There was no major medical or surgical illness in the past.
Physical examination
Results of chest examination were within normal limits, apart from left parasternal tenderness.
Laboratory examinations
The patient had normal hemogram, and erythrocyte sedimentation rate was 35 mm in the first hour. He was worked up for metabolic causes of chest pain, his vitamin D level was within normal limits, and serum calcium was 10.42 mg/dL. Urine examination showed trace proteins. Urine for Bence jones proteins and blood electrophoresis were found to be negative for multiple myeloma.
Imaging examinations
The chest X-ray was within normal limits. The electrocardiograph, 2D echocardiography and treadmill test were also within normal limits. The patient even underwent coronary angiography due to the troublesome nature of his chest pain,which was also normal. Upper gastrointestinal endoscopy was done to rule out reflux disease and gastroesophageal ulcers, which was once again normal. The patient was referred to psychiatry, and underwent cognitive behavior therapy, however this too was of no avail. He was also being worked up for musculoskeletal causes and was started on non-steroidal anti-inflammatory drugs suspecting costochondritis, but he remained uncomfortable (Table 1).
To rule out sternal and rib lesions, he was screened with an ultrasound of the chest wall, which showed cortical irregularities along with a hypoechoic mass in the sternum and left 5rib (Figure 1). Considering the cortical irregularities, differential of bone neoplasms, metastasis and multiple myeloma were kept in consideration. He underwent magnetic resonance imaging (MRI) of the spine, which showed multiple well-defined T1/T2 hypointense lesions of varying sizes in the dorso lumber vertebra at multiple levels, including the body of the sternum and posterior aspect of the left 4rib. A whole body positron emission tomogram (PET scan) was done to rule out any primary, which showed multiple fluorodeoxyglucose avid lesions in the axial andappendicular skeleton (Figure 2). To confirm the diagnosis, bone marrow aspiration and biopsy were performed, which showed increased immature and mature plasma cells. Marrow was slightly hypercellular for age and showed all hematopoietic components. There was a marked interstitial prominence of plasma cells along with a definitive presence of sheets of plasma cells.

Table 1 Timeline
This is a very rare case where chest pain was the only initial symptom of multiple myeloma, and shows how screening ultrasonography helped in leading us to the diagnosis. There is no evidence reported in the literature of any such case where multiple myeloma was diagnosed using ultrasonography.
FINAL DIAGNOSIS
Multiple myeloma.
TREATMENT
He was started on bortezomib, leflunomide and dexamethasone.
OUTCOME AND FOLLOW-UP
After a mere two cycles of chemotherapy, he showed drastic improvement in pain wherein his Visual Analogue Score dropped from 7/10 to 2/10.
DISCUSSION
Chronic chest pain has been broadly classified as cardiogenic and non-cardiogenic chest pain (NCP). The etiology of NCP can be pulmonary, gastrointestinal,musculoskeletal or psychosomatic. At times it becomes very difficult to search the etiology of chest pain.
Multiple myeloma is a clonal condition of B cells that involves uncontrolled proliferation of abnormal plasma cells. Clinical features can either be directly due to proliferation or indirectly due to substances released by these cells. It results in suppression of erythropoiesis along with multiple osteolytic lesions, which results in hypercalcemia, skeletal pain and pathological fractures. It also causes the accumulation of monoclonal immunoglobulins (Igs) along with other regulating substances. These circulating monoclonal Igs or their subunits are the reason behind proteinuria, renal tubular damage and amyloid deposition.
They have varied presentation, 10%-40% are asymptomatic and 50%-70% have bone pain due to lytic lesions and pathological fractures. About 1%-5% cases may not demonstrate Igs or their subunits in serum or urine (non-secretory multiple myeloma).
This is a unique case where initial work-up, consisting of a complete hemogram,serum calcium, erythrocyte sedimentation rate, chest radiology, urine bence jones proteins and serum electrophoresis, was normal. This misguided us to search for other causes of chest pain. However, during later ultrasound screening for a musculoskeletal cause, we came across multiple cortical irregularities over the ribs that helped us in clinching the diagnosis.
Ultrasound of bone has not been frequently used in the past. It has been used as a diagnostic tool in the evaluation of costochondral cartilage deformities in children of the anterior chest wall mass where there was negative radiography, and has been used in bone tumors like chondrosarcoma and fractures where a painful area shows fragmented cortical bone and at times subperiosteal hematoma.
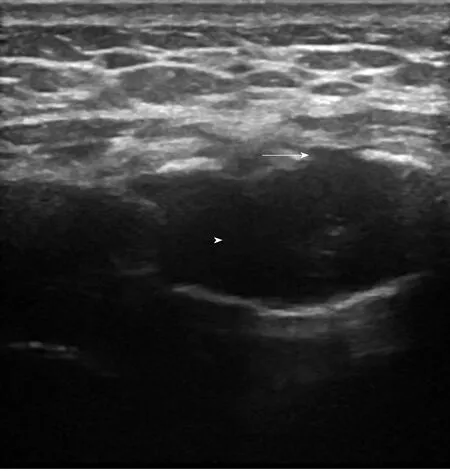
Figure 1 Ultrasound of sternum showing cortical irregularities (arrow) with central hypoechoic area (arrow head).
The chest wall is known to get involved either by direct extension of a tumor mass,metastases or hematologic malignancy like multiple myeloma. In this region,metastases are mainly from breast, thyroid, kidney, lung and prostate cancer along with plasma cell myeloma. The vast majority of such tumors are osteolytic.Ultrasound detection of osseous defects is possible only after the damage of the anterior compact substance.
Paikhas shown ultrasonography to be better than conventional radiography(39%) for the diagnosis of such tumors. These were characterized by cortical defects or an irregular cortical edge or a mass invading local soft tissues, including pleura in some cases. Leecompared a group of patients with rib metastases from renal cancer and prostate cancer metastases, and they showed that the irregular surface of the costal cortex in the absence of fracture or the presence of masses within the soft tissue represented the only sonographic feature of osteoblastic foci of prostate cancer.
While for multiple myeloma it has never been used in the literature, we found cortical irregularities along with focal bone destruction (Figure 1), which was later confirmed with MRI by the presence of multiple osteolytic lesions. PET computed tomography ruled out any contribution from the kidney, thyroid or lung and also helped in assessing disease burden and the identification of extramedullary involvement. Bone marrow biopsy sealed the diagnosis. Apart from atypical presentation and an unconventional way of diagnosing, our case was unique as the patient had normal hemoglobin, absent bence jones proteins and a negative M band on electrophoresis,. the patient was having non-secretory multiple myeloma, which is even difficult to diagnose.
CONCLUSION
Multiple myeloma is notorious to present in atypical ways, and therefore one should have a high index of suspicion for the same. Ultrasound of bone can often help in reaching the diagnosis indirectly if not directly. As a non-invasive, bedside and easily available investigation, it is truly a patient-friendly approach to finding clues in difficult cases.
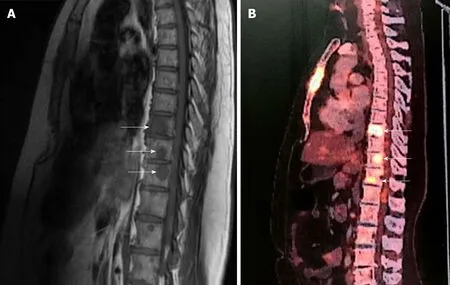
Figure 2 Magnetic resonance imaging and positron emission technology scan.
ACKNOWLEDGEMENTS
I would like to thank Dr. Govind Patel from Clinical Hematology for his valuable inputs and Dr. Nupur Abrol for Pain and Palliative care.