
Muscular involvement of extranodal natural killer/T cell lymphoma misdiagnosed as polymyositis:A case report and review of literature
2020-04-25 02:38LiHuiLiuQingHuangYunHaiLiuJieYangHanFuLinJin
World Journal of Clinical Cases 2020年6期
Li-Hui Liu,Qing Huang,Yun-Hai Liu,Jie Yang,Han Fu,Lin Jin
Abstract
Key words: Lymphoma; Extranodal natural killer/T cell lymphoma; Muscular;Polymyositis; Muscle swelling; Case report
INTRODUCTION
Natural killer (NK)/T cell lymphoma is a rare disease in non-Hodgkin's lymphoma(NHL),accounting for about 5%-18% of NHL[1].It most commonly presents as destructive lesions in the nasal cavity and other midline facial structures.About 1/3 of these occur in nonnasal areas[2],also known as extranodal types and including the skin,testicles,liver,and spleen; however,it is rarely found in skeletal muscle[3-5].Herein,we report a case with calf muscle swelling as the unique initial manifestation,showing progressive development with a final diagnosisviamuscle biopsy as NK/T cell lymphoma.We also discuss the cause of the initial misdiagnosis of polymyositis and review the relevant literature about extranodal NK/T cell lymphoma-affected muscles.
CASE PRESENTATION
Chief complaints
A 42-year-old man presented with bilateral calf swelling for 5 mo,as well as left facial swelling for 4 mo.
History of present illness
At 1 mo prior,the patient had presented to a local hospital with bilateral calf and left facial swelling.During the hospital visit,the patient had intermittent low fever.The laboratory examination showed that the erythrocyte sedimentation rate was 31 mm/h.Electromyography indicated that there were more positive phases and fibrillation potential in the left gastrocnemius muscle,thus hinting at the possibility of myogenic damage.Magnetic resonance imaging of calf muscles indicated abnormal signals in the bilateral gastrocnemius and soleus muscle.Therefore,the first muscle biopsy was considered,and the pathological result of the left gastrocnemius muscle revealed a large amount of spindle cell infiltration,accompanied by necrosis and regeneration of individual muscle fibers (unfortunately,the results of immunohistochemistry were missing).The patient was considered for "polymyositis"and treated with methylprednisolone for 10 d,and the swelling of both the calf and face was slightly improved.However,1 mo later,the patient developed drooping of the right eyelid.
History of past illness
The patient had a good health record.
Personal and family history
The patient had no relevant personal or family history.
Physical examination upon admission
A physical examination showed both calves were swollen,the left facial region had slightly intumescentia compared to the contralateral side,and there was right eyelid swelling and drooping.
Laboratory examination
Serum lactate dehydrogenase was elevated (379-901 U/L,reference:120-250 U/L),Epstein-Barr virus (EBV) and DNA was significantly increased (3.13-5.19 × 105IU/mL,reference:< 400 IU/mL).Serum creatine kinase was normal (105-220 U/L,reference:50-310 U/L).
Imaging examinations
Cranial magnetic resonance imaging scan enhancement was reported for the subcutaneous soft tissue masses in the left cheek and forehead,as well as thickening of the right levator palpebrae superioris.Whole-body positron emission tomography/computed tomography (PET/CT) showed multiple areas of muscle swelling,with decreased muscle density and increased metabolic dispersion (Figure 1).The left portion of the posterior wall and the left wall of the oropharynx showed soft tissue masses,with abnormally increased metabolism.Finally,puncture biopsies of the left calf muscle and left pharyngeal side wall were completed.Examination of the left leg revealed a small amount of tissue that was mainly necrotic,but the tumor could not be excluded.The pathological diagnosis of the left side pharyngeal wall showed NK/T cell lymphoma,and immunohistochemistry showed CD20 (-),CD3 (+),CD30(+),CD56 (-),EBER (+),Ki67 (60%),TIA-1 (+) and CD68 (±) staining (Figure 2).
FINAL DIAGNOSIS
The patient was diagnosed with extranodal NK/T cell lymphoma.
TREATMENT
The patient received a chemotherapy regimen of methotrexate,dexamethasone,etoposide,and pegaspargase.
OUTCOME AND FOLLOW-UP
The swelling of both the calf and face of the patient was rapidly and significantly improved (Figure 3).Additionally,the swelling of the right eyelid improved and could be slightly raised.Over the following 8 mo,the patient received chemotherapy five more times,and still had intermittent fever,but the muscle swelling did not worsen.
DISCUSSION
Extranodal NK/T cell lymphoma is a malignant tumor,strongly associated with EBV and a poor prognosis.The typical pathological features include diffuse lymphocytic infiltration,showing angiodestruction as well as angiocentric growth,and is often accompanied by fibrinoid changes in blood vessels and coagulative tissue necrosis[6].The typical immunohistochemical characteristics are as follows; CD2(+),cytoplasmic CD3(+),CD56(+),EBV(+) and cytotoxic granule-associated protein(+) staining,which include granzyme B,TIA-1 and perforin[7].
This patient initially presented with swelling in the bilateral gastrocnemius and soleus.In a recent review of the literature,only about seven cases of extranodal NK/T cell lymphoma had been reported with an initial manifestation of myopathic symptoms[4,8-13],and these were primarily diagnosed initially as myositis (Table 1).Two cases was considered to be granulomatous myositis[8,11],two cases were diagnosed as polymyositis[4,12]and one as phlegmonous myositis[10].In only one of these cases,the presence in gastrocnemius and soleus muscle was initially diagnosed as peripheral eosinophilia[13].Our patient was diagnosed as polymyositis by his first attending physician in the local hospital,and the reasons for this could be as follows:Multiple muscle swelling,low fever,lactate dehydrogenase,and erythrocyte sedimentation rate elevation.Furthermore,electromyography indicated myogenic damage was possible,and muscle biopsy showed necrosis and regeneration of the individual muscle fibers.Thus,the patient received methylprednisolone treatment,but the muscle swelling continued to progress.Subsequently,he came to our hospital,and the diagnosis of “polymositis” was called into question by our attending physician.Firstly,the muscle swelling did not improve,but instead increased after methylprednisolone therapy.Secondly,the muscle swelling in this patient was mainly localized in the distalvsproximal limb.Lastly,the laboratory examination revealed that the EBV DNA quantitation was significantly elevated,and there was a lack of testing for myositis-related antibodies.Therefore,we planned to arrange for this patient to complete myositis antibody and whole-body PET/CT examination,however he only chose the whole-body PET/CT.The results showed multiple sites of muscle damage throughout the body.Thus,the relevant tissue biopsies were tested,and the diagnosis of NK/T cell lymphoma was confirmed by lateral pharyngeal biopsy.
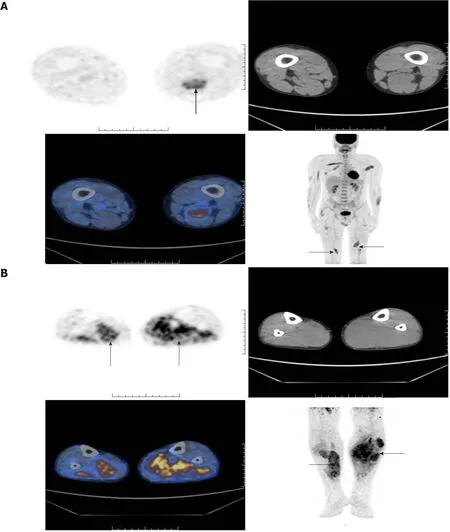
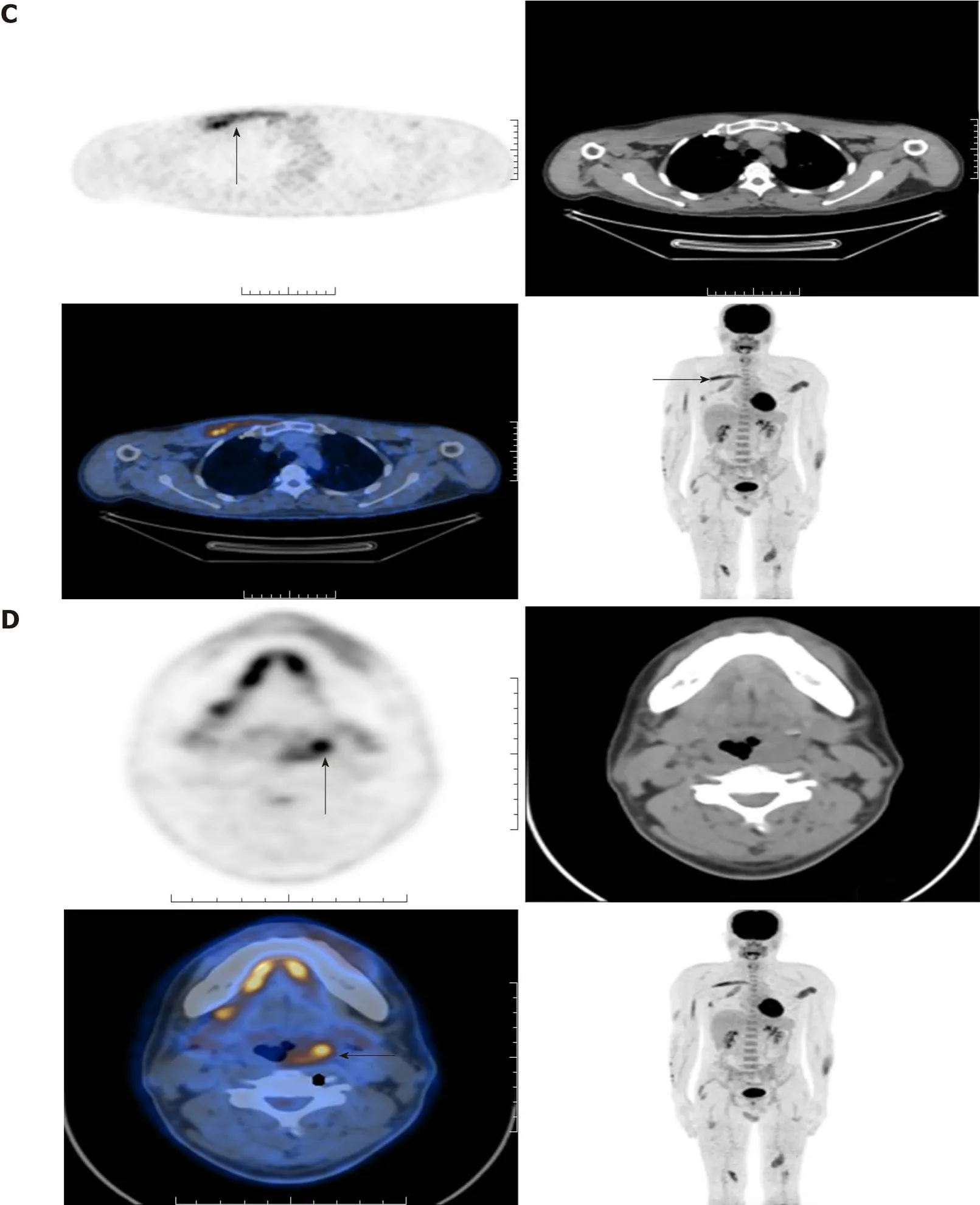
Figure 1 Positron emission tomography/computed tomography scans.
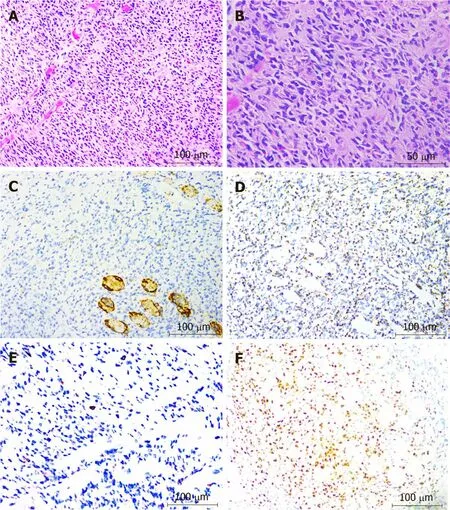
Figure 2 lmmunohistochemical staining.
The lateral pharyngeal biopsy showed diffuse heterotropic lymphocytic infiltration,consistent with NK/T cell lymphoma.Immunohistochemistry showed that the lymphoid cells were CD20 (-),CD3 (+),CD30 (+),CD56 (-),EBER (+),Ki67 (60%),TIA-1 (+) and CD68 (±).In contrast with typical extranodal NK/T cell lymphoma immunohistochemical characteristics,the CD56 in this patient was negative and CD30 was positive.It is known that while CD30 is closely related to anaplastic large cell lymphoma,its expression in extranodal NK/T cell lymphoma is infrequent[14].There have been literature reports that EBV is believed to be a key component in the etiology of extranodal NK/T cell lymphoma,and can induce CD30 expression by the infection and transformation of lymphocytes[15].We thus think that the CD30 positivity in this patient was associated with the high expression of EBV.The literature suggests that CD3+CD56+EBV+is an important clue to diagnose NK/T cell lymphoma[16],but there have been studies that demonstrate that CD56 is not a specific biomarker for NK cells,and can be expressed on other blood cells,such as T cells[17].Finally,the patient received a chemotherapy regimen of methotrexate,dexamethasone,etoposide and pegaspargase.The muscle swelling improved,and conditions were stable over the next five additional rounds of chemotherapy.
CONCLUSION
It is extremely rare for extranodal NK/T cell lymphoma to be involved in skeletal muscle.This disease is difficult to diagnose and highly invasive,usually leading to delays in treatment.This should be included in the differential diagnosis of progressive and unexplained muscle swelling.A definitive diagnosis always requires adequate viable tissues for pathological and immunocytochemical characterizations.Finally,selecting the appropriate chemotherapy regimen can significantly improve symptoms or delay the development of disease.
Table 1 Comparisons with previous cases of extranodal natural killer/T cell lymphoma with manifested myopathic symptoms

Figure 3 Calf circumference before and after chemotherapy treatment.
ACKNOWLEDGEMENTS
We thank professor Zheng-Hao De of the pathology department and professor Wei-Hua Liao of radiology for technical assistance.
 World Journal of Clinical Cases2020年6期
World Journal of Clinical Cases2020年6期
- World Journal of Clinical Cases的其它文章
- Repair mechanism of astrocytes and non-astrocytes in spinal cord injury
- Study on the correlation and predictive value of serum pregnancy-associated plasma protein A,triglyceride and serum 25-hydroxyvitamin D levels with gestational diabetes mellitus
- Significance of 125I radioactive seed implantation on growth differentiation factor and programmed death receptor-1 during treatment of oral cancer
- Computed tomography-based score model/nomogram for predicting technical and midterm outcomes in transjugular intrahepatic portosystemic shunt treatment for symptomatic portal cavernoma
- Efficacy of totally laparoscopic compared with laparoscopic-assisted total gastrectomy for gastric cancer:A meta-analysis
- Allograft artery mycotic aneurysm after kidney transplantation:A case report and review of literature