
Therapeutic observation on herbal cake-partitioned moxibustion for dysmenorrhea due to deficiency cold
2020-06-22 09:51LuLi陸麗WangYafang王亞芳ZhangYan張琰LuWang魯望DengHaiping鄧海平ZhaoHaiyin趙海音
Lu Li (陸麗), Wang Ya-fang (王亞芳), Zhang Yan (張琰), Lu Wang (魯望), Deng Hai-ping (鄧海平), Zhao Hai-yin (趙海音)
1 Shanghai University of Traditional Chinese Medicine, Shanghai 201203, China
2 Longhua Hospital Shanghai University of Traditional Chinese Medicine, Shanghai 200032, China
Abstract
Keywords: Moxibustion Therapy; Indirect Moxibustion; Herbal cake-partitioned Moxibustion; Thermal Box Moxibustion; Point, Shenque (CV 8); Point, Zhongji (CV 3); Point, Zigong (EX-CA 1); Dysmenorrhea
Dysmenorrhea refers to the periodic lower abdomen pain that occurs in women during, before or after menstruation. Patients may experience pain that radiates toward the lumbosacral area, or even fainting due to severe pain[1]. Epidemiological study showed that 80% of women worldwide had different degrees of dysmenorrhea, of which about 75% had an impact on work and study[2]. At present, Western medicine mainly uses oral analgesics and contraceptives for dysmenorrhea, and considers surgical treatment for those who don’t respond to conservative treatments. However, the oral medications for primary dysmenorrhea (PD) have a quick onset, short effect and more adverse reactions in long-term use. Surgery may have high risk and complexity, and it is not the first choice for the treatment of PD[3-5].
In recent years, studies have confirmed the effect of traditional Chinese medicine, especially acupuncture on dysmenorrhea[6]. Dysmenorrhea is mainly caused by pathogenic cold. The two most common patterns are intermingled deficiency and excess, and blood stasis due to cold retention. Therefore, the treatment strategies are to warm meridians and remove cold[7]. Moxibustion can warm and unblock meridians, circulate qi and blood, remove cold and resolve dampness. Studies have shown that moxibustion is safe and effective for PD. It addition, it has fewer adverse reactions[8-10].
Numerous studies on moxibustion for dysmenorrhea are undergoing in China. However, few clinical studies compared the effects of different moxibustion methods. In order to explore a better moxibustion therapy for dysmenorrhea, based on literature researches and results of previous study[11], we applied herbal cake-partitioned moxibustion and mild moxibustion for patients with dysmenorrhea between 2016 and 2018, and observed the changes of visual analog scale (VAS) and COX menstrual symptom scale (CMSS) scores, and assessed the clinical efficacy.
1 Clinical Materials
1.1 Diagnostic criteria of Western medicine
This study referred the diagnostic criteria of dysmenorrhea in theObstetrics and Gynaecology(8th Edition)[12]: lower abdominal pain and down-bearing distention occurs during, before or after menstruation, accompanied by soreness in the low back or other uncomfortable symptoms that seriously affect the quality of life; PD is more common in adolescent women, and usually occurs within 1-2 years after menarche; most of the pain appears after menstruation, and the earliest appears in 12 h before menstruation, with the most severe pain appearing on the first day of menstruation, lasting for 2-3 d and then relieved. The pain is usually spasmodic, located in the pubic bone of lower abdomen and can radiate to the lumbosacral area and inner thigh; may be accompanied by nausea, vomiting, diarrhea, dizziness and fatigue, and presenting with pale complexion and cold sweating in severe cases; no abnormal findings in gynecological examination.
1.2 Criteria for syndrome differentiation of traditional Chinese medicine (TCM)[13]
Cold pain in lower abdomen during menstruation, ameliorated by warmth and pressure, thin menstrual flow with dark purple blood and clots, accompanied by aversion to cold with cold limbs, clear urine in large amount, pale complexion, white tongue coating, and fine or sunken tight pulse.
1.3 Inclusion criteria
Those who met the above diagnostic criteria and the syndrome differentiation criteria in Chinese medicine; who had lower abdominal pain during menstruation or 1 week before or after menstruation with a certain period; had or had no other discomforts; aged 12 to 45 years old; had no other therapy for this disease in the last menstrual cycle; agreed to participate in this clinical trial and signed informed consent.
1.4 Exclusion criteria
Those with severe pain had to use analgesic drugs, or who could not stop other therapy for this disease; those with severe primary diseases of cardiovascular, liver, kidney, or hematopoietic systems, or those had mental diseases; those with extremely irregular menstrual cycles; those who received other related treatments at the same time that might interfere with the results of this study; those who were allergic or unbearable to the smell of moxa; who were not suitable for moxibustion, such as those with ulcers at the moxibustion site, with scar diathesis, allergic constitution, fever, or tumors, or pregnant women.
1.5 Elimination criteria
Those who were misdiagnosed; who did not follow the treatment protocol; those with poor compliance or dropped out during the treatment; with incomplete clinical examination or evaluation data closely related to this study.
1.6 Statistical methods
Microsoft Excel 2010 was used to establish the database, and all data were statistically analyzed by the IBM SPSS Statistics 22 statistical software, and statistical charts were drawn. Chi-square test was used for the comparison of general data. As to the data of clinical efficacy assessments, VAS and CMSS scores were expressed as median (inter quartile range) [M (IQR)] since they were in non-normal distribution, and non-parametric test was applied: Wilcoxon rank-sum test was applied to the comparison of intra-group data, and Mann-WhitneyUtest was applied to the comparison between groups. Rank-sum test was used to evaluate the overall clinical efficacy. The test level ofα=0.05 was used for a two-sided test.P<0.05 was considered to indicate a statistically significant difference.
1.7 General data
A total of 70 patients were enrolled, collected from the Clinic of TCM Department of Longhua Hospital (Pudong Branch), Shanghai University of Traditional Chinese Medicine, all due to deficiency cold. All patients were randomly divided into a herbal cake-partitioned moxibustion group and a mild moxibustion group by the random number table according to the visiting sequence, with 35 cases in each group. There were no statistically significant differences in the general data between the two groups (allP>0.05), indicating that the two groups were comparable (Table 1).

Table 1. Comparison of the general data between the two groups
2 Treatment Methods
2.1 Mild moxibustion group
Points: Shenque (CV 8), Zhongji (CV 3), and bilateral Zigong (EX-CA 1).
Moxibustion appliances: BX-A002 Baixiao moxibustion produced by Chongqing Happyall Medical Equipment Co., Ltd., with 4 cm×8 cm of the moxibustion tube size, and 1.5 cm×1.5 cm of the moxibustion cone size; the size of the packaging box was 30.5 cm× 21.5 cm×5.8 cm.
Methods: Point locations referred to theNomenclature and Location of Acupuncture Points(GB/T12346-2006)[14]. The patient took a prone position. The physician fixed the moxibustion tube with the medical tape attached to the Baixiao moxibustion device, making the groove at the bottom of the moxibustion tube stuck on the skin opposite to the moxibustion area. Then the physician attached the magnetic block of the moxibustion cone to the cover of the moxibustion tube, ignited the moxibustion cone and buckled it with the moxibustion tube. The size of the air inlet was adjusted by rotating the moxibustion tube to raise and lower the height of the moxibustion tube cover, so as to maintain the appropriate temperature for moxibustion (took slight thermal pain of the skin at the moxibustion site as the measure, generally about 43 ℃). Each point was treated with one moxa cone, and the treatment ended after the moxibustion cone burned out and cooled down, which was about 25 min.
2.2 Herbal cake-partitioned moxibustion group
Points: Same as those in the mild moxibustion group.
Moxibustion appliances: Same as those in the mild moxibustion group.
Ingredients and preparation of herbal cake: Equal portions ofTu Si Zi(Semen Cuscutae),Bu Gu Zhi(Fructus Psoraleae),Ai Rong(Moxa Floss),Rou Gui(Cortex Cinnamomi),Chuan Xiong(Rhizoma Chuanxiong),Bai Shao(Radix Paeoniae Alba) andHuang Qin(Radix Scutellariae) were ground into fine powder and mixed evenly, sealed and stored. Before moxibustion, took appropriate amount of powder added with some chitosan solvent to prepare the herbal cake (2.5 cm in diameter, 0.5 cm in thickness). At the center of the herbal cake, 5 small holes of the same size were pricked by a stainless-steel acne needle with a diameter of 0.2 cm for heat penetration.
Methods: The herbal cake was embedded in the groove of the Baixiao moxibustion tube near the skin, and fixed on the moxibustion point with medical tape together with the moxibustion tube. The rest steps were the same as those in the mild moxibustion group. After moxibustion, the herbal cake was fixed on the points with sterile dressing for 4 h, and then removed by the patient himself.
2.3 Treatment course and cautions
Both groups were treated starting from 1 week before menstruation. The moxibustion was applied once every other day, with 5 times as a course of treatment. The treatment continued for 3 menstrual cycles. The patient was required to avoid wind-cold, keep good mood and have regular diet during the treatment.
3 Therapeutic Efficacy Observation
3.1 Observation items
The VAS and CMSS were scored before and after treatment, and also at the end of the 3rd menstruation after treatment.
3.1.1 VAS score
The VAS was marked with 0 at one end, indicating ‘no pain’, recorded as 0 point, and 10 at the other end, indicating ‘most painful’, recorded as 10 points. The higher the score, the more severe the pain.
3.1.2 CMSS score[15]
The CMSS consists of 21 items, and is divided into 4 grades. Scoring criteria: A for no; B for a small amount of time; C for a considerable amount of time; D for most of time or always. Positive scoring questions A, B, C, D scored 0, 1, 2, 3 points, respectively; and the reverse scoring questions (2 questions marked with * in total)scored 3, 2, 1, 0 point. Less than 32 points indicated mild dysmenorrhea, 33-47 points indicated moderate dysmenorrhea, and 48 points or above indicated severe dysmenorrhea. The higher the score, the more severe the dysmenorrhea and the concomitant symptoms.
3.2 Criteria of curative efficacy
According tothecriteriaof curativeefficacy for dysmenorrheaintheGuiding Principles for Clinical Study of New Chinese Medicines[13], the curative efficacy was assessed. According to the VAS score, the analgesic effect was evaluated.
Cured: After treatment, the VAS score was reduced to 0, without abdominal pain and other symptoms, and there was no recurrence in 3 menstrual cycles.
Markedly effective: After treatment, the VAS score decreased to less than 1/2 of that before treatment.Abdominalpain was significantly reduced, and other symptoms wereimproved.Thepatient wasableto continue working without taking painkillers.
Effective: After treatment, the VAS score decreased to1/2-3/4 of that before treatment. Abdominal pain was relieved, and other symptoms were improved. The patient was able to keep on working without painkillers.
Invalid: No changes of the degree of pain and other symptoms.
3.3 Results
3.3.1 Comparison of the clinical efficacy
After treatment, the clinical efficacy was evaluated at the end of the 3rd menstrual cycle after treatment. The totaleffectiveratewas88.6% intheherbal cake-partitioned moxibustion group and 74.3% in the mildmoxibustiongroup.Therewas nosignificant difference in the total effective rate between the two groups(P>0.05),indicating that theoverallclinical efficacy of thetwo groups wasequivalent,butthe herbalcake-partitionedmoxibustiongrouphadthe tendency to be superior to the mild moxibustion group(Table 2).

Table 2.Comparison of the clinical efficacy between thetwogroups(case)
3.3.2 Comparison of the VAS and CMSS scores
Comparisons of theVAS andCMSS scoresbetween before andafter treatmentinthesame group:After treatment,theVAS andCMSS scores of bothgroups decreasedsignificantly (allP<0.05),indicating that both moxibustionmethodscouldsignificantly relievethe painandtheconcomitant symptoms inpatientswith dysmenorrhea.At thefollow-upafter 3menstruation cycles fromtheendof thetreatment,theVAS and CMSS scoresof bothgroups weresignificantly lower thanthosebeforetreatment(allP<0.05).Atthe follow-up,theVAS scoresinbothgroups hadno statisticaldifferences fromthose after treatment (bothP>0.05);theCMSS scoresinthetwo groupswere significantly lower thanthoseafter treatment (bothP<0.05),(Table3and Table 4).
Comparisons of theVAS andCMSS scoresbetween the twogroupsat the sametimepoint:Therewereno significant differencesintheVASandCMSSscores betweenthetwogroupsbeforetreatment(bothP>0.05).After treatment andat the follow-upafter 3 menstruationcyclesfromtheendof thetreatment,there werenosignificant differencesintheVAS score betweenthetwo groups(bothP>0.05).After treatment,theCMSSscoreintheherbalcake-partitioned moxibustiongroupwaslower thanthat inthe mild moxibustion group,andthedifferencewas statistically significant(P<0.05).At thefollow-up,there was no significant differenceintheCMSS scorebetweenthe two groups(P>0.05),(Table 3and Table 4).
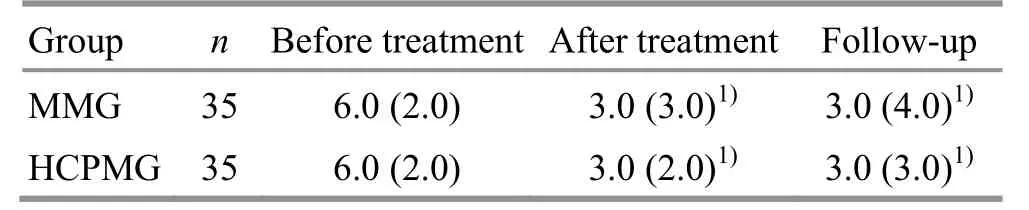
Table 3.Comparison of the VASscorebetween thetwo groups[M (IQR),point]
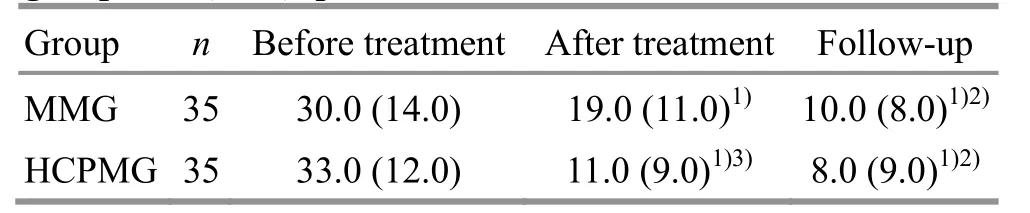
Table 4.Comparisonof the CMSSscore between the two groups[M (IQR),point]
4 Discussion
Chinese medicine believes that the dysmenorrhea is closely relatedtotheThoroughfareandConception Vessels,andtheuterus.Itismainly causedby constitutionaldeficiency or/anddeficiency cold.The insufficient nourishment of uterusandthe ThoroughfareandConceptionVessels lead to ‘when there is malnutrition, there is pain’. Cold may obstruct the flow of qi and blood, and ‘when there is obstruction,thereis pain’.Therefore,inthis study,weselected dysmenorrhea patients due to deficiency cold.
Moxibustioncanwarmandunblock meridians,regulate qi and blood, remove cold and reinforce the body. In this study, Shenque (CV 8), Zigong (EX-CA 1)andZhongji(CV 3)arecommonly usedtotreat dysmenorrhea. Shenque (CV 8) and Zhongji (CV 3) are important points for the treatment of dysmenorrhea,becausethey arethe key points of the Conception Vessel.The ConceptionVesselistheseaof yin meridians,anditgoverns fetuswithplacentaand umbilicalcord,closely relatedto menstruationof women and reproduction of human. Zigong (EX-CA 1) is located at 4 cunbelow umbilicus,3cun aside from Zhongji(CV 3).It is commonly usedto treat reproductive diseases for women.
Westernmedicinebelieves that themechanism of dysmenorrhea is the increased contraction of uterine smooth muscles and small arteries, and the ischemia and hypoxia of uterus causes pain. Studies have found that moxibustion can significantly improve the uterine microcirculationinpatients withdysmenorrhea,increasethebloodflow velocity of theuterus,and reduce vascular resistance[16-17]. The near-infrared rays inthe burning processof moxibustionhavestrong penetrating power, which candirectly penetrateinto the deeper partsof the humanbody,dilatelocal capillaries,improve bloodcirculation,reduce neural excitation,andexert analgesic effect.Animal experiment studiesshowedthat moxibustioncan regulate the behavior,nerve-endocrine-immunity and other aspects indysmenorrheaanimalmodel,thus relieving the symptoms of dysmenorrhea. Among them,theeffect of herbalcake-partitionedmoxibustionat umbilicus was superior tomoxa stick moxibustion at umbilicus, and moxa stick moxibustion at umbilicus was superior to medicinalsticking at umbilicus[18-19].The herbalcake-partitionedmoxibustionisacommon moxibustiontherapy.Studies havefound that it has consistent infrared radiation spectrum with the points of the human body, which may be the material basis for theeffects of theherbalcake-partitioned moxibustion[20-21]. Compared with the mild moxibustion,the herbalcake-partitionedmoxibustionis combined with moxibustion and medicine.By transdermal drug delivery, the medicinal ingredients penetrate into the body by the synergism of warm effect through the skin of point.It not only exerts thestimulation effect of moxibustion and medicine on acupuncture points, but also exertsthepharmacologicaleffect of medicine absorbedby humanbody.Comparedwiththeoral drugs,theherbalcake-partitionedmoxibustioncan prevent the liver and various digestive enzymes from decomposing and destroying the effective ingredients of the medicine on one hand, and at the same time can eliminatethepossibleadversereactionsdueto gastrointestinaltractstimulationcausedby the medicine.
The results of this study indicated that both herbal cake-partitionedmoxibustionandmildmoxibustion could significantly reduce the pain severity in patients withdysmenorrhea,andherbalcake-partitioned moxibustionhadabetter effect inimproving concomitant symptoms than mild moxibustion. To sum up, it is safe and convenient and has few toxic or side effects.

Conflict of Interest The authorsdeclarethat thereisnoconflict of interest.Acknowledgments This work wassponsored by National BasicResearch Program of China (973Program,國(guó)家重點(diǎn)基礎(chǔ)研究發(fā)展計(jì)劃項(xiàng)目, No.2015CB554505).Statement of Informed Consent Informed consent wasobtained from allindividual participants.
Received:19September 2019/Accepted:24October 2019
猜你喜歡
中國(guó)體育科技(2019年12期)2019-02-28
勞動(dòng)保護(hù)(2018年5期)2018-06-05
小天使·一年級(jí)語數(shù)英綜合(2017年7期)2017-08-04
今日重慶(2017年2期)2017-03-04
小天使·一年級(jí)語數(shù)英綜合(2017年2期)2017-02-16
小天使·一年級(jí)語數(shù)英綜合(2017年2期)2017-02-16
小天使·五年級(jí)語數(shù)英綜合(2017年1期)2017-02-08
中國(guó)火炬(2015年2期)2015-07-25
 Journal of Acupuncture and Tuina Science2020年3期
Journal of Acupuncture and Tuina Science2020年3期
- Journal of Acupuncture and Tuina Science的其它文章
- Therapeutic observation on lung-clearing and spleen-strengthening tuina in children with exogenous cough
- Effects of electroacupuncture plus drug anesthesia on pain and stress response in patients after radical surgery for stomach cancer
- Therapeutic effect of heat-sensitive moxibustion plus medications for senile osteoporosis and its effect on serum BMP-2 and OPG levels
- Clinical observation on heat-sensitive moxibustion plus lactulose for postoperative constipation of mixed hemorrhoid due to spleen deficiency
- Therapeutic efficacy observation on auricular point sticking therapy for cardiac syndrome X in women
- Therapeutic observation of manipulation plus exercise therapy in treating upper crossed syndrome postures of primary school students