
Effect of 8-week and 12-week triple therapy (doxycycline, rifampicin,and gentamicin) on brucellosis: A comparative study
2020-07-23 00:27:18AfsanehKaramiAhmadrezaMobaienManizheJozpanahiAmirhosseinMoghtaderMojdehiMonaJavaheri
Journal of Acute Disease 2020年4期
Afsaneh Karami, Ahmadreza Mobaien, Manizhe Jozpanahi, Amirhossein Moghtader-Mojdehi,Mona Javaheri
Department of Infectious Diseases, School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran
ABSTRACT Objective: To compare the effect of 8-week and 12-week of triple therapy (doxycycline, rifampicin, and gentamicin) on brucellosis.Methods: This parallel clinical trial was conducted on 339 brucellosis patients who were divided into 2 groups. The first group(175 patients) received doxycycline (100 mg/12 h) for 8 weeks,rifampicin (600 mg/d) for 8 weeks, and gentamicin (5 mg/kg/d) for 7 d, while in the second group (164 patients), doxycycline and rifampicin treatment were prolonged to 12 weeks, along with gentamicin therapy for 7 d. The patients were followed-up for six months after the treatment. Baseline information, clinical manifestations of the patients were collected, and serological tests for brucellosis were performed after the treatment.Results: The mean age of the patients was (45.95 ± 18.65) years,and 56.9% of the patients were male. In total, 73.5% of the patients were residents in rural areas and the majority of them were farmers and ranchers (34.6%). The 3-month relapse rates of the two groups were 11.42% and 6.70%, respectively (P=0.132). Moreover,the 6-month relapse rate of the two groups was 6.3% and 2.4%,respectively (P=0.085). In the two groups, both treatments could reduce serological titers based on Wright and 2ME tests (P<0.05).Conclusions: The efficacy of 8-weeks and 12-weeks triple therapy (doxycycline, rifampicin, and gentamicin) is similar in terms of brucellosis relapse. The 8-week triple therapy including doxycycline, rifampicin, and gentamicin can be considered as an effective approach for the treatment of brucellosis.
KEYWORDS: Brucellosis; Treatment duration; Relapse
1. Introduction
Brucellosis is a zoonotic disease, which is caused by a Gramnegative coccobacillus known asBrucella[1]. This bacterium lives intracellularly as a non-spore-forming and non-motile genus[2].Brucellosis in humans is predominantly caused by four species ofBrucella, includingBrucellamelitensis,Brucellasuis,Brucella
abortus, andBrucellacanis[3]. Brucellosis transmits to humans through oral, cutaneous, and respiratory contact with infected animals or the animal products. Nevertheless, the person-to-person spread of brucellosis is extremely rare[4,5]. According to the statistics released by the World Health Organization, brucellosis affects more than half a million individuals each year in 100 countries[6,7].
With the brucellosis incidence of 4 000 cases per year, the main hyperendemic regions for this infectious disease include Peru and Mexico in Latin America; Spain and Greece in Europe; and Iraq,Iran, Jordan, and Kuwait in central Asia[8]. In Iran, the incidence of brucellosis has been estimated at 29.8%[9] that varied from 7 to 276 per 100 000 in Qom and Kermanshah province, respectively[10].The highest prevalence of brucellosis in Iran has been reported in Hamadan Hamadan (25%) followed by Markazi (24.7%) and Mazandaran (22.5%)[9]. Moreover, another estimation reported that the highest incidence of brucellosis was in Hamadan (107.5 per 100 000), Kurdistan (83.5 per 100 000), west Azarbaijan (71.4per 100 000)[11], and Zanjan (67.1 per 100 000)[6]. The clinical presentations of brucellosis may be acute, subacute, or chronic.Furthermore, recurrent brucellosis is commonly reported sinceBrucellais an intracellular bacterium[3,12]. The most frequent symptoms of brucellosis include fever, chills, night sweats, anorexia,fatigue, and weight loss[10,11].
Post-treatment follow-up is essential in patients with brucellosis due to the risk of relapse, which has been reported to occur in 5%-30% of the patients[13]. The serological titer decreases over one year after the treatment. Despite the low mortality rate of brucellosis(2% inBrucellaendocarditis), the recovery course is reported to decelerate after the application of antibiotic therapy[14]. However,there is a lack of consensus on the duration of brucellosis treatment.While some researchers consider 6 weeks to be sufficient, other experts believe 12 weeks of treatment to be more effective due to the risk of disease relapse[3,15].
Brucellosis is a disease with a thousand faces, which may have several clinical manifestations, ranging from fever to septicemia and multi-organ involvement. Due to the diverse clinical manifestations of this infection, the diagnosis of brucellosis is quite challenging,which may lead to delayed treatment and increased risk of complications[8,16]. Based on the observed clinical symptoms and serological tests, brucellosis patients are prescribed with 2-3 months of treatment regimens[8,13,15]. Given the importance of the treatment duration in terms of the long-term drug tolerance of brucellosis patients and the complications of the treatment, it is essential to compare the 8-week treatment course with 12-weeks regarding the risk of the relapse. As a result, it could be determined whether increasing the duration of treatment from 9 to 12 weeks could be more effective in patients with brucellosis. The present study aimed to compare the 8- and 12-week of triple treatment regimen(doxycycline, rifampicin, and gentamicin) addressing brucellosis relapse.
2. Materials and methods
2.1. Participants
This study was registered in Iranian Registry Clinical Trial Center (IRCT20180817040819N1). Altogether, 339 patients with brucellosis were included in this clinical trial. The diagnosis of brucellosis was confirmed based on the clinical and serological symptoms of the selected patients (Wright>1.80; 2ME>1.40).
The inclusion criteria of the study were as follows: (1) Age >12 years; (2) Confirmed diagnosis of brucellosis; (3) Absence of complications; (4) Admission to the infectious diseases ward of Valiasr Hospital. ??
The exclusion criteria were (1) Allergic reactions to the prescribed medications; (2) History of renal diseases; (3) Hearing and balance disorders.
The patients were selected by convenience sampling method and after obtaining informed consent, the eligible patients were assigned into two groups using block random allocation with four-part blocks.
2.2. Intervention
In the first group (175 patients), the patients received treatment with three drugs: doxycycline tablets (100 mg twice daily for 8 weeks),rifampicin (600 mg/d for 8 weeks, and gentamicin (5 mg/kg/d for 7 d).In the second group (164 patients), the patients received the same three drugs (doxycycline tablets and rifampicin for 12 weeks and gentamicin (5 mg/kg/d) for 7 d). The patients were followed-up for six months after the treatment, and serological tests for brucellosis were performed on all the patients before and after the treatment course. The patients were re-examined 1 month, 3 months, and 6 months after the treatment. Relapse was defined as the recurrence of the clinical symptoms of brucellosis as confirmed by the serological tests (increased 2ME and Wright compared to the post-treatment serology).
2.3. Statistical analysis
Data analysis was performed using SPSS version 20 (SPSS Inc.,Chicago, IL, USA). Frequency, percentage, and mean ± standard deviation were used for description of data. Moreover,Chi-square and Wilcoxcon test was used for comparison of the two groups regarding the symptoms and relapse incidence at different times after treatment. The significant level of the test was set atα=0.05.
3. Results
In total, 339 patients with brucellosis were analyzed in this study,which was divided into two groups with 175 patients in the first group receiving the treatment for 8 weeks and 164 patients in the second group receiving the treatment for 8 weeks. The mean age of the patients was (45.95 ± 18.65) years, and 56.9% of the patients were male. Among the patients, 73.5% of cases resided in rural areas. In terms of occupation status, 32.4%, 26.0%, 14.1%,13.9%, and 13.6% of the patients were farmers and ranchers,housewives, unemployed and students, self-employed, and employed, respectively. No significant differences were observed between the two groups in terms of gender (P=0.338), place of residence (P=0.532), occupation status (P=0.478), and education level (P=0.894). Besides, 321 (94.7%) patients had a history of brucellosis treatment while 18 (5.3%) patients had not (Table 1).The mean interval since the manifestation of the disease symptoms to the onset of the treatment was 30 (21-56) d.
The most common clinical manifestations of brucellosis before treatment were fever (81.1%), sweating (65.8%), myalgia (69%),arthralgia (56.9%), headaches (14.5%), lethargy (46%), loss of appetite (44.5%), coughs (8%), diarrhea (4.1%), and dysuria(13.6%). The prevalence of hepatomegaly, splenomegaly,meningitis, spondylitis, arthritis, sacroiliitis, and orchitis was estimated at 1.2%, 0.3%, 0.9%, 3.8%, 5.6%, 16.5%, and 1.5%,respectively. In addition, the symptoms of the two groups were shown in Table 1. At the beginning of the treatment course, 71.1%of the patients had a normal white blood cell (WBC) count, while 19.5% and 9.4% had leukopenia and leukocytosis, respectively.Moreover, 62.8%, 36.0%, and 1.2% of the patients had normal hemoglobin (HB), anemia, and polycythemia, respectively.On the other hand, 80.5% of the patients had normal platelet(PLT) count, while 16.5% and 2.9% had thrombocytopenia and thrombocytosis, respectively. Among the studied patients, 72.9%and 84.1% had high erythrocyte sedimentation rate (ESR) and higher C-reactive protein (CRP) than the normal level, respectively.The results indicated no significant differences between the two groups in terms of WBC count (P=0.700), HB (P=0.972), PLT count (P=0.840), ESR (P=0.271), and CRP (P=0.528) before the treatment.
After the treatment, 95.6% of the patients had normal WBC, 3.8%had leukopenia, and 0.6% had leukocytosis. Additionally, 91.7%of the patients had normal HB, while 8.3% had anemia. On the other hand, 97.1% of the patients had normal PLT count, 2% had thrombocytopenia, and 0.9% had thrombocytosis. It is also notable that 1.8% of the patients had high ESR, and 0.9% had higher CRP than the normal level. Comparison of the 2ME and Wright tests before and after the treatment indicated the significance of the treatment in both groups of 8-week (P<0.001) and 12-week treatment (P<0.001), which denoted the positive effect of the treatment on the reduction of serological titers (Table 2).
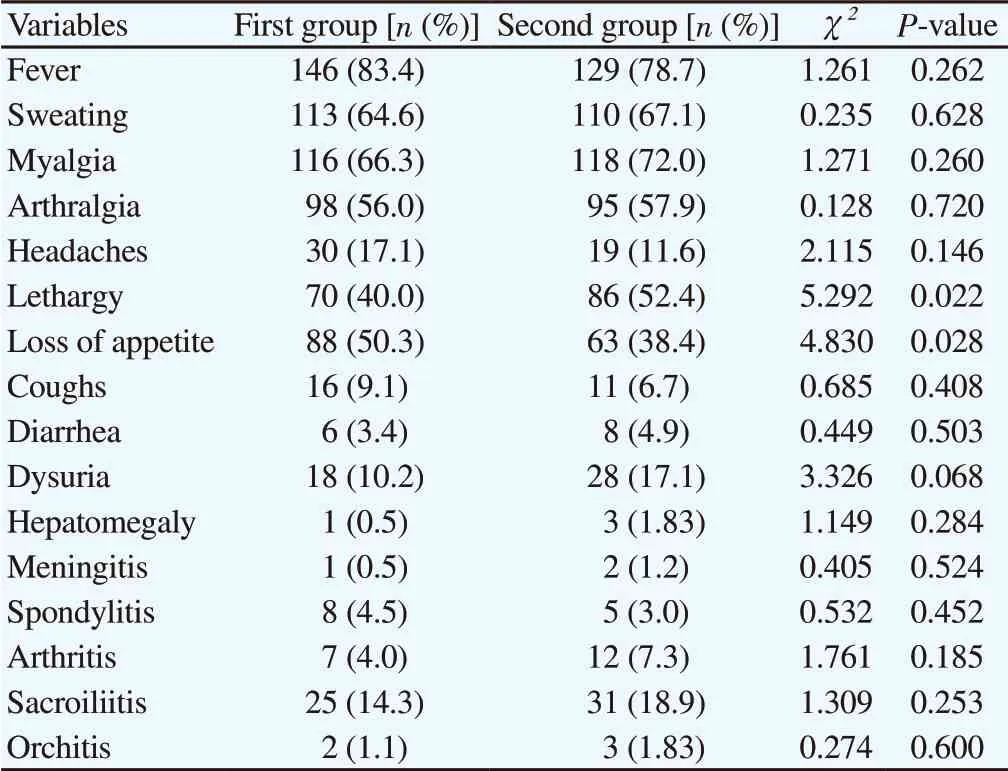
Table 1. Comparison of clinical symptoms and complications between 8-week and 12-week treatment group.

Table 2. Results of 2ME and Wright test before and after the treatment in the two groups.

Table 3. Comparison of the relapses between 8- and 12-week treatment.
No significant differences were observed between the groups in terms of the relapse 1 month (P=0.162), 3 months (P=0.132), and 6 months (P=0.085) after the treatment (Table 3). The relapse rates 3 months after treatment were 11.42% and 6.7% in 8-week and 12-week treatment (P=0.132). Moreover, the relapse symptoms 6 months after treatment were 6.3% and 2.4%, respectively(P=0.085).
In addition, no significant difference was denoted in the WBC count (P=0.432), HB (P=0.829), PLT count (P=0.219), ESR(P=0.936), and CRP (P=0.170) after the treatment. In conclusion,both 8-week and 12-week triple therapy (doxycycline, rifampicin,and gentamicin) have the same positive effect on brucellosis.
4. Discussion
In the present study, 73.5% of the patients lived in rural areas, which indicated the higher prevalence of brucellosis in these regions. In addition, 34.6% of the patients were ranchers and farmers, and 68.3% were male, which could be justified considering the higher prevalence of the disease in villages, as well as the more important role of men in agriculture and farm tasks compared to women. In a research conducted by Sofianet al.,approximately 62.5% of brucellosis patients were rural residents,while only 37.5% lived in urban areas[17]. In another study, a significant association was observed between animal husbandry and incidence of brucellosis[18], which is consistent with the findings of other studies[11,18,19].
According to the current research, the most common clinical symptoms of brucellosis were fever (81.1%), myalgia (69.0%),sweating (65.8%), and arthralgia (56.9%). In the research by Sofianet al., arthralgia and sweating were reported to be the most common symptoms of brucellosis[17]. On the other hand, pain and fever were reported to be the most common clinical symptoms of brucellosis in another study[18]. Similar results showed in a systematic review, in which fever, joint pain, and sweating were the most common manifestations of brucellosis among 65.7%, 58.1%and 55.3% of Iranian patients, respectively[20].
According to the findings of the current research, the three-drug treatment could reduce the serological titers ofBrucellain both study groups. In this regard, another study showed that treatment with gentamicin for 5 d plus doxycycline for 8 weeks is not superior to that of streptomycin for 2 weeks plus doxycycline for 45 d[21]. The results of the present study indicated no significant difference between the groups receiving 8 weeks and 12 weeks of treatment in terms of brucellosis relapse. It is notable that data is scarce regarding the assessment of brucellosis relapse after various treatment periods, and most of the studies in this regard have only compared the type of prescribed drugs for these patients.
Another study concluded that the doxycycline-streptomycin combination is the first-line regimen for the treatment of brucellosis, recommend doxycycline-rifampin and ofloxacinrifampin combinations as the second-line regimens[22]. Moreover,adding levofloxacin to doxycycline-rifampin for acute/subacute brucellosis could increase the efficacy of treatment and lower the brucellosis relapse[22]. Another study compared the relapse rate of gentamicin-doxycycline and streptomycin-doxycycline treatment and showed the relapse rate was 2.4% and 6.1%, respectively.Moreover, the efficacy of the gentamicin-doxycycline regimen was 95.12% and the streptomycin-doxycycline regimen was 89%[21].Nevertheless, in the clinical trial by Sofian,et al., no significant difference was reported between the two patient groups receiving treatment with a combination of three drugs and two treatment periods in terms of the disease relapse[17], which is in line with the findings of the current research.
While the recommended standard regimen is a two-drug therapy within 6 weeks, the 8-week treatment course for brucellosis is preferred in many patients due to the high prevalence and recurrence of the disease in developing countries. Nonetheless,some cases of disease relapse are still reported. The increased treatment course of brucellosis is important in terms of long-term drug tolerance and treatment complications.
According to the results, there was no significant difference in brucellosis relapse between 8 and 12 weeks of treatment.Therefore, it could be inferred that 8 weeks of brucellosis treatment could effectively reduce treatment costs and prevent drug sideeffect in brucellosis patients. It is notable that longer treatment durations are recommended in the complicated cases of brucellosis.Further investigations in this regard should be performed on larger sample sizes in order to confirm this finding.
Conflict of interest statement
The authors report no conflict of interest.
Acknowledgments
Hereby, we extend our gratitude to the Vice Chancellor of Research and Technology at Zanjan University of Medical Sciences, Iran for the financial support of this research project(IRCT20180817040819N1).
Authors’ contributions
A.K.: Contributions to the conception or design of the interpretation of data for the work; and Final approval of the article; A.M.:Contributions to the conception or design of the interpretation of data for the work; and Final approval of the article; M.J.; Contributions to the conception or design of the work and Final approval of the articles; A.M.; Contributions the acquisition and analysis of data for the work and Drafting the article; M.J.; Contributions to the conception or design of the work analysis, or interpretation of data for the work; and Final approval of the article.
 Journal of Acute Disease2020年4期
Journal of Acute Disease2020年4期
- Journal of Acute Disease的其它文章
- Intensive care outcomes of refugee patients in Turkey between 2013 and 2019: A retrospective descriptive study
- Adult-onset Still's disease: A case report
- Cope’s sign and complete heart block secondary to acute cholecystitis: A case report
- Open reduction and internal fixation for radial head fractures: A prospective observational study
- Prevalence and antimicrobial susceptibility patterns of bacteria in ICU patients with lower respiratory tract infection: A cross-sectional study
- Incidence of Enterobius vermicularis in acute appendicitis: A systematic review and meta-analysis