
Clinical features and radiological manifestations of COVID-19 disease
2020-12-15 08:00:34PedroLandeteCarlosAndrQuezadaLoaizaBeatrizAldaveOrzaizSusanaHernndezMuizAntonioMaldonadoEnriqueZamoraAllanCharlesSamCernaEliadelCerroRaquelCanoAlonsoFelipeCouago
World Journal of Radiology 2020年11期
Pedro Landete, Carlos Andrés Quezada Loaiza, Beatriz Aldave-Orzaiz, Susana Hernández Mu?iz, Antonio Maldonado, Enrique Zamora, Allan Charles Sam Cerna, Elia del Cerro, Raquel Cano Alonso, Felipe Cou?ago
Abstract
Key Words: COVID-19; Coronavirus; Natural history; Clinical features; Pathogenesis;Radiology images
INTRODUCTION
Coronavirus disease 2019 (COVID-19) was first discovered when unexplained cases of viral pneumonia began to emerge in Wuhan, China early December 2019. The coronavirus belongs to the Coronaviridae family of single-stranded RNA viruses, which together with the Roniviridae and Arteriviridae families, comprise the Nidoviruses order.Coronavirus owes its name to the crown-like glycoprotein spikes on its surface,evident on examination with electron microscope.
Coronaviruses are found in various animal species, including birds, livestock, and other mammals such as camels, bats, mice, cats, and dogs. Coronaviruses are widely distributed and highly infectious, making it a potent pathogen. Human pathogenic subtypes of coronavirus are associated with mild clinical symptoms; however, two notable exceptions are the coronaviruses associated with Middle East Respiratory Syndrome (MERS-CoV) and severe acute respiratory syndrome (SARS-CoV).
The current outbreak began as pneumonia of unknown etiology in Wuhan, China.Laboratory studies identified the causal factor as a new strain of coronavirus, initially called 2019-nCoV; later the International Committee on Taxonomy of Viruses changed the name to SARS-CoV-2. Subsequently, on 11 February 2020, the World Health Organization (WHO) denominated the disease caused by this new virus COVID-19.The ongoing outbreaks of coronavirus around the world represent an important public health threat. Moreover, due to changes in the world’s ecosystem and climate in recent decades, new outbreaks are more likely to occur in the future.
From December 30, 2019 to March 20, 2020, more than 200000 people were diagnosed with COVID-19 worldwide. Disease progression is rapid and some patients develop severe respiratory failure shortly after disease onset. Our understanding of COVID-19, including clinical manifestations, pathogenesis, and treatment comes mainly from recently-published research studies and clinical observation during the period of acute infection.
SARS-CoV-2 is primarily transmitted from person to person. Although asymptomatic individuals can transmit the virus, symptomatic individuals are the most common source of transmission, which occurs mainly through the propagation of respiratory droplets by means of coughing or sneezing. The virus can be transmitted between individuals who are in close contact, with a greater risk in enclosed spaces due to high concentrations of aerosols. Given that aerosol droplets generally fall to the ground within a few meters, there is a lower likelihood of transmission when people maintain a distance of at least 2 metres. SARS-CoV-2 has a basic reproduction factor of 2.2, meaning that one patient will, on average, infect an additional two people. Current data suggest that the incubation period for the virus ranges from three to seven days. In the present mini review, we evaluate the clinical manifestations and imaging findings of COVID-19 infection.
NATURAL HISTORY OF COVID-19 DISEASE
Symptoms
The COVID-19 pandemic has numerous psychological, socioeconomic, and medical consequences. COVID-19 is among the most significant threats that society has had to confront in the current century to date. Therefore, it is crucial to understand the pathophysiology and clinical implications of this disease, as well as the development of novel preventive and therapeutic strategies.
Based on currently available data, males and older people have a higher risk of infection and mortality. The virus has a high capacity to enter and infect lung cells,where it causes interstitial pneumonitis. It can also affect other organs, potentially leading to multiorgan failure, in very severe cases, potentially involving the cardiovascular system.
Individual response to the virus is highly heterogenous, suggesting that COVID-19 should probably not be considered, phenotypically, a single disease. It is more probable that certain, still unknown characteristics of the host explain the variable course of disease, which can range from mild to severe, which may include cytokine release syndrome (CRS) and multiorgan failure.
The main clinical symptoms are respiratory, frequently associated with severe pneumonia. However other organs are commonly affected. The patient may present disseminated intravascular coagulation and/or pulmonary embolism, as evidenced by elevated levels of D-dimers and fibrin breakdown products.
COVID-19 primarily affects the lungs but can also involve the immune system.Pathologic examination of COVID-19 victims reveals the presence of splenic atrophy in which lymphocytes and neutrophils are significantly reduced, with the presence of necrosis and hemorrhage.
Blood tests reveal elevated levels of several ILs (IL-2, IL-6, IL-7), granulocyte colonystimulating factor (G-CSF), chemokine 10, and tumor necrosis factor-α alpha (TNF-α),the presence of which is characteristic of cytokine release syndrome. The development of CRS in COVID-19 is associated with disease severity, reminiscent of the cytokine profile observed in hemophagocytic lymphohistiocytosis. Patients who develop CRS frequently present high levels of serum IL-6. In fact, a retrospective,multi-site analysis in Wuhan found that IL-6 Levels were predictive of COVID-19-associated mortality.
The cytokine storm and elevated IL-6 signalling detected in these patients could have severe consequences for the cardiovascular system, potentially leading to tachycardia, left-ventricular dysfunction, and hypertension. CRS-associated cardiotoxicity-mainly conduction abnormalities, atrial fibrillation, and elevated levels of brain natriuretic peptide and troponins-has also been described.
Disease spread
The incubation period between contact and symptom onset generally ranges from 1 to 14 d, although this can reach 24 d in some cases. The median (mean) time between recorded exposure and symptom onset is 5.1 (6.1) d. Elimination of viral nucleic acids requires from 8 to 34 d (median, 20 d) after the appearance of the initial symptoms.
Seven different coronaviruses can infect humans: HCoV-NL63 and 229E are alphacoronaviruses associated with mild disease in adults; MERS-CoV and SARS are betacoronaviruses associated with severe respiratory disease; and OC43 and HKU1,associated with mild disease. COVID19 is caused by a new betacoronavirus that likely originated in bats after gain-of-function mutations in the receptor-binding domain.
Coronavirus receptors bind through the spike (S) protein, which is encoded by structural gene S. This has two subunits [subunits 1 (S1) and subunits 2 (S2)]. S1 mediates binding while S2 (a trimeric stem) mediates fusion with the infected cell. The receptor-binding S1 contains the N-terminal domain and the C-terminal domain.These two domains are capable of mediating binding to a variety of cell receptors that contain carbohydrates and proteins. SARS-CoV, SARS-CoV-2, and alpha-coronavirus HCoV-NL63 bind through S1-CTD to angiotensin-converting enzyme 1 (ACE1).Compared to SARS-CoV, the novel SARS-CoV-2 has a higher affinity for ACE2,involving a greater number of interaction sites in the binding process. For the SARS-CoV-2 to bind ACE2, the S protein must first be cleaved by the transmembrane protease, serine 2 (TMPRSS212). Replication occurs by means of RNA-dependent polymerase RNA and involves discontinuous transcription of the subgenomic mRNA that code for 6 key open reading frameworks common to all known coronaviruses.
Importantly, transmission of SARS-CoV-2 is associated with infected persons with a high viral load (up to 1 billion copies of RNA per millilitre of sputum) and with the virus’ capacity to remain viable for long periods of time on contaminated surfaces.SARS-CoV-2 is more stable on certain surfaces (e.g., stainless steel, plastic) than on others (e.g., cardboard), and the virus may be present and viable for three days (72 h)on these surfaces. The viral load tends to be higher in severe cases, who require an extended period to eliminate the virus.
Morbidity and mortality
A recent study in China (through January 28, 2020) found that 16% of cases may present severe disease, with an estimated overall mortality rate of 1.4% for reported cases, vs the 4.61% rate reported by the WHO. In some geographic regions, for reasons that remain unclear, the mortality rate may be even higher, with current estimated rates in Italy of 11.9% and 9.0% in Spain. In this regard, it is important to be cautious when attempting to calculate mortality rates based on current data, as these may be overestimated-due to inadequate community testing-or underestimated as a consequence of to the prolonged time period between a positive test and death, or to major differences between countries in the criteria used to classify COVID-related mortality. Healthcare systems that have been overwhelmed by a surge in patients requiring invasive or non-invasive mechanical ventilation must also be considered as a potential source of inter-country discrepancies in mortality rates.
PATHOPHYSIOLOGIC FRAMEWORK OF SARS-COV-2 AND THERAPEUTIC STRATEGY
Various studies have established that the pathogenesis of COVID-19 begins with the recognition of an angiotensin receptor (ACE2), especially common on the surface of type 2 alveolar cells and capillary endothelial cells. These cells are infected by the SARS-CoV-2 virus, assisted by the viral protease TMPRSS212, thus allowing the virus to replicate easily.
The optimal therapeutic strategy remains an open question, in part because this depends on the stage of the infection. Most of the studies published to date have focused on antiviral drugs (e.g., remdesivir, lopinavir/ritonavir, favipiravir,oseltamivir) or immunomodulators (corticosteroids, immunoglobulins, monoclonal antibodies), as well as other treatments such as chloroquine, nitric oxide,extracorporeal membrane oxygenation, among others. To date, no treatment has proven to be safe and effective against COVID-19, thus management of these patients should focus on preventing infection and life support measures.
COVID-19 disease can be considered to have three distinct phases, in which the therapeutic strategy will vary according to the phase and disease severity (Figure 1).
Viral phase
The initial phase begins at infection, and includes the incubation period and the onset of non-specific symptoms (general malaise, fever, nonproductive cough). During this phase, SARS-CoV-2 uses the ACE2 receptor to enter and establish itself in the host cellmainly alveolar cells and vascular endothelial cells-after which it begins to replicate,leading to a mild respiratory infection and general symptoms.
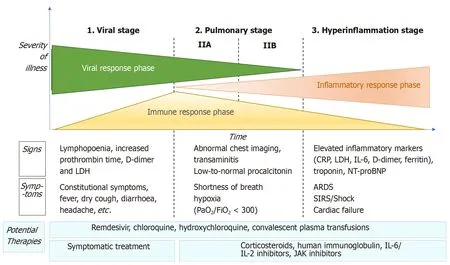
Figure 1 Adaptation of Siddiqi et al[29] the phases of coronavirus disease 2019 disease, including signs, symptoms, and potential therapeutic targets for each phase. CRP: C-reactive protein; LDH: Lactate dehydrogenase; BNP: Brain natriuretic peptide; ARDS: Acute respiratory distress syndrome; SIRS: Systemic inflammatory response syndrome; IL: Interleukin; JAK: Just another kinase.
Diagnosis in this phase is made by reverse transcription polymerase chain reaction(RT-PCR), serology for SARS-CoV-2 (IgG and IgM), radiology [computed tomography(CT) or, if unavailable, chest X-ray], and blood tests, including a complete blood count(in which lymphopenia and neutrophilia are common), liver function markers, and acute-phase reactants. The aim of treatment during this phase is symptom control.
Pulmonary phase
In this phase, the virus continues to replicate, leading to pulmonary involvement (viral pneumonia with or without hypoxemia, 2A or 2B respectively). CT and chest X-ray imaging reveal bilateral infiltrates and ground-glass opacities, while blood test findings are characterized by lymphopenia, elevated transaminases, and markers of systemic inflammation. Most patients in this stage require hospitalization, whose main purpose is to closely monitor the patient to ensure that early treatment will be available in case of significant clinical worsening. Treatment consists of life-support measures and anti-viral agents, such as remdesivir, which has been available for compassionate use.
Patients in stage 2 who do not present significant hypoxia should not receive corticosteroids due to the risk of bacterial superinfection. However, in patients with significant hypoxemia and/or the need for non-invasive respiratory support, antiinflammatory treatment (corticosteroids) is recommended.
Hyperinflammatory phase
Only a few patients with mild to moderate infection will develop a severe form of the disease, manifesting as extrapulmonary systemic inflammatory response syndrome.These patients will present elevated serum levels of markers of systemic inflammation such as C-reactive protein or fibrinogen. Various studies have demonstrated that inflammatory markers such as cytokines, ILs (IL-2, IL-6, IL-7), G-CSF, TNF-α, PCR,ferritin, and/or D-dimer are significantly higher in patients with more severe forms of the disease.
This phase is characterized by the following: (1) development of severe respiratory failure requiring respiratory support; (2) shock; and (3) organ failure (including myocarditis) due to severe systemic inflammation. To reduce the effects of the systemic inflammatory cascade and the risk of multiorgan failure in patients at this stage, the following treatments are recommended: Immunomodulating agents such as high-dose corticosteroids, tocilizumab (an IL-6 inhibitor), anakinra (an IL-1 receptor antagonist), or intravenous immunoglobulins. The prognosis and likelihood of recovery in patients at this stage are poor, which is why early diagnosis and treatment are essential.
Radiologic manifestations (chest X-ray and CT)
Simple chest X-ray and CT both play a key role in the diagnosis of SARS-CoV-2 pneumonia, follow-up, and detection of complications. These imaging tests can also help to determine disease severity. The main radiologic manifestations are groundglass opacities and areas of consolidation (generally bilateral), similar to the characteristics observed in other coronaviruses such as SARS-CoV and MERS-CoV.
Chest X-ray has a low sensitivity to detect pulmonary infiltrates during the initial phases of infection and in mild forms of the disease. Nonetheless, the wide availability of X-ray makes it a valuable tool to establish the radiologic suspicion of pneumonia,especially in limited resource settings. The main role of chest X-ray is to monitor the course of pulmonary lesions in patients with severe disease, including those admitted to intensive care. A study involving 64 patients diagnosed with SARS-CoV-2 found that basal consolidations were the most common finding on X-ray, which were normal in 20% of cases(Figure 2).
The mains signs of COVID-19 on CT (Table 1) have been widely described. There are several common signs, which are usually most evident from 10-12 d from symptom onset. The most common and characteristic manifestation is multifocal ground-glass opacities, of variable extension and morphology, with peripheral/subpleural distribution (including perifissural regions).
The following findings will vary according to the stage of the infection:Asymptomatic patients may present pulmonary opacities but with limited extension. In the first two days from symptom onset, CT findings are normal in just over 50% of cases.
During the early phase (first week) ground-glass opacities are common, with or without vascular dilatation. Rapid progression of these opacities and/or consolidations is common. Ground-glass opacities with reticulation (“crazy-paving pattern") have been associated with more advanced disease (Figure 3).
Later (at 2-3 wk from infection) signs of organized pneumonia can be seen(linear/curved consolidation patterns, perilobular pattern, reverse halo sign)(Figure 3). As the disease begins to resolve, there is a decrease in alveolar opacities and subpleural lines begin to emerge.
The long-term clinical course is unknown, but it is expected that some patients with severe pneumonia will develop pulmonary fibrosis, as occurred with SARS (2003), in which a small percentage of patients presented signs of fibrosis with reticulation associated with traction bronchiectasis. Some findings are rare, including nodal involvement, tree-in-bud pattern, cavitation, lobar/segmental consolidation, and significant pleural effusion. The presence of such findings should suggest a different diagnosis or the presence of complications, such as a bacterial superinfection.
The differential diagnosis includes infectious and non-infectious processes. To discriminate SARS-CoV-2 pneumonia from other viral pneumonias, the most common findings are subpleural pulmonary opacities and the microvascular dilation sign.
The Radiological Society of North America (RSNA) proposes standardizing the radiologic report to improve communication with clinicians to facilitate patient management. The RSNA suggests that there are four main CT findings relative to the diagnosis of COVID-19: (1) compatible with viral pneumonia; (2) indeterminate; (3)atypical (suggestive of other diagnoses); and (4) no evidence of pneumonia.
CT allows us to determine the extent of the lung disease, which correlates with clinical severity. The presence of extensive areas of consolidation usually indicates a poor prognosis, especially in the elderly. CT is also useful to assess suspected complications, particularly pulmonary thromboembolism, whose incidence is higher in patients with severe disease.
Various guidelines have described the indications for performing imaging tests in patients with suspected SARS-CoV-2. However, the role of CT for diagnosis and screening for SARS-CoV-2 has been questioned, although some authors have emphasised its diagnostic value, especially when RT-PCR is unavailable. However,in a review of the literature, Raptis et alfound that the limited data (mostly from retrospective studies) do not substantiate the use of CT as a diagnostic test for COVID-19. In addition, in the meta-analysis carried out by Kim et al, the sensitivity of CT was greater than 90% but the specificity was low, leading those authors to conclude that, given the high false positive rate of CT, this imaging technique should not be used for screening in geographic regions where the disease prevalence is low (< 10%).Therefore, although certain radiologic findings and patterns are common in SARSCoV-2 pneumonia, the definitive diagnosis requires a positive RT-PCR test result.
The Fleischner Society recommends the following that imaging tests not be performed in cases of community transmission and mild infection (no hypoxemia,mild or no dyspnea), except in patients with risk factors (diabetes, obesity,hypertension, etc). By contrast, this society recommends performing imaging tests in cases with moderate to severe infection (hypoxemia, moderate-severe dyspnea),regardless of the findings of RT-PCR. CT is indicated in patients who present functional abnormalities and/or hypoxemia after the recovery phase, while RT-PCR is indicated if incidental findings on CT suggest the presence of viral pneumonia.
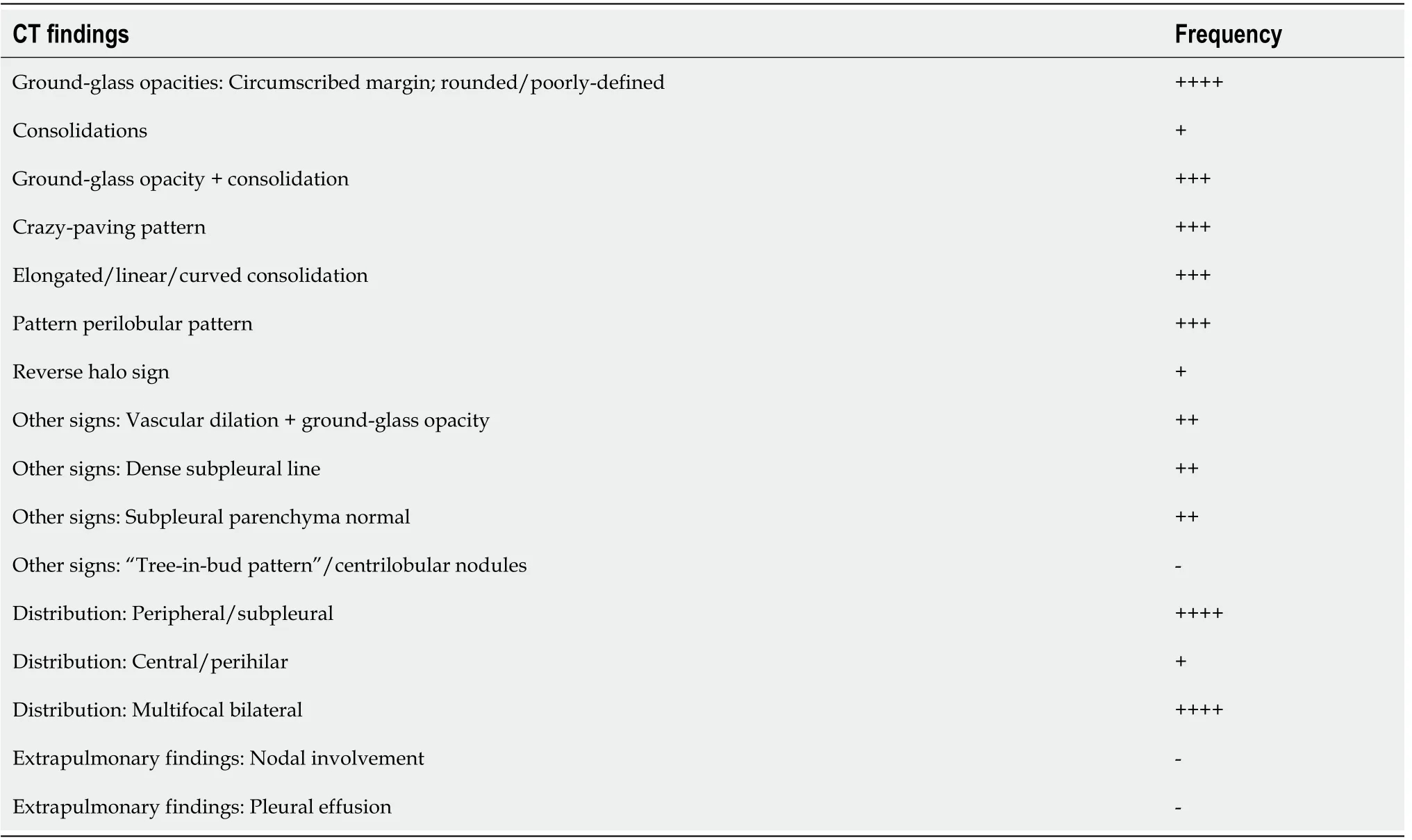
Table 1 Computed tomography findings, the most common findings are bolded
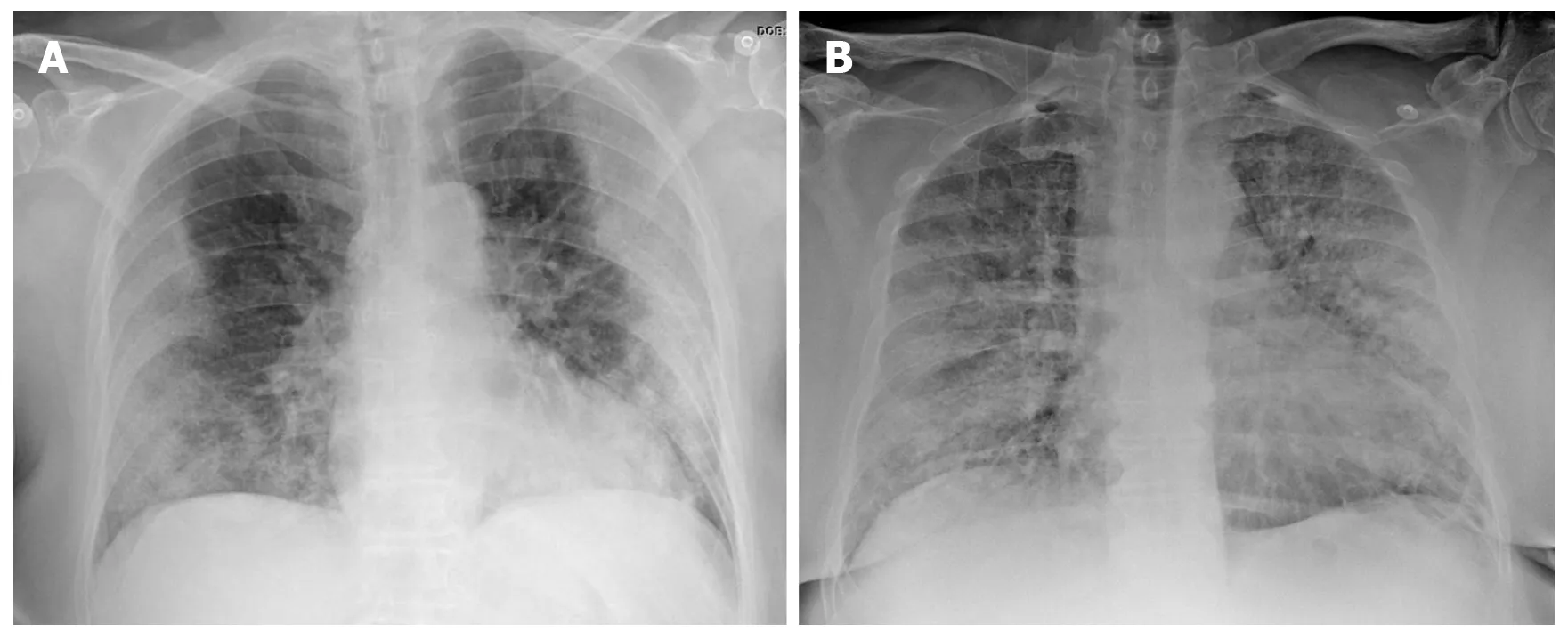
Figure 2 Chest X-ray findings in two patients with confirmed severe acute respiratory syndrome coronavirus 2 pneumonia (positive reverse transcription polymerase chain reaction test). A: 73-year-old diabetic woman. General malaise, myalgia and diarrhea of 8 d clinical course.Dyspnea in the last 2 d, no fever. AP X-ray: Peripherally-distributed bilateral lung opacities; B: 60-year-old man, fever and cough, progressive dyspnea. The patient presented at the emergency department with acute respiratory failure requiring admission to intensive care. AP X-ray: Alveolar infiltrates and diffusely-distributed,bilateral ground-glass opacities.
FLUORODEOXYGLUCOSE-POSITRON EMISSION TOMOGRAPHY METABOLIC IMAGING IN COVID-19
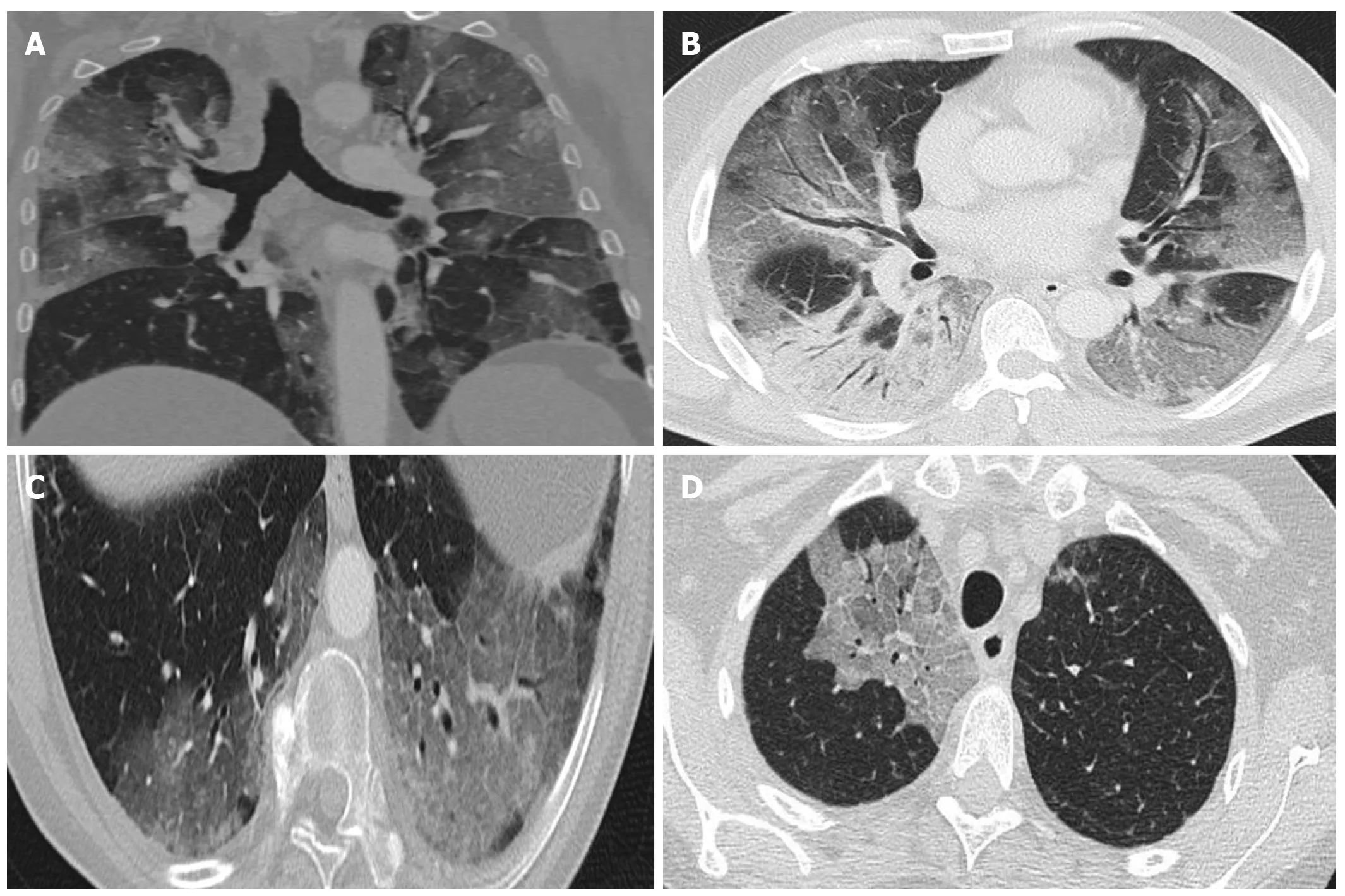
Figure 3 Computed tomography findings. A: Extensive bilateral ground-glass opacities, one with poorly-defined margins and another with clearly defined borders; B: Multilobar ground-glass opacities and consolidation with air bronchogram in the right lower lobe. Band of subpleural parenchyma respected in the left lung; C: Microvascular dilation sign in the middle of ground-glass opacity in the left lower lobe; D: Crazy-paving pattern in the right upper lobe.
Positron emission tomography-CT (PET-CT) imaging with fluorodeoxyglucose (FDG)(18F-fluorodeoxyglucose) is a highly useful diagnostic tool for inflammatory or infectious pulmonary diseases in general, as it can not only demarcate the affected areas, but it can also be used to evaluate treatment response and monitor the clinical course. However, only a few published studies have assessed the utility of 18F-FDGPET-CT metabolic imaging in COVID-19 patients, although the first reports support the value of this FDG-PET to evaluate lung areas with inflammation/infection.
Although FDG-PET imaging should not be routinely used in COVID-19 patients,the first published studies suggest that metabolic data provided by this imaging technique can provide important complementary data in these patients. In particular,FDG-PET metabolic imaging can be of value in the following areas: (1) as a diagnostic tool in asymptomatic patients for the differential diagnosis and to diagnosed patients with a normal CT scan; (2) to monitor treatment response, in combination with CT; (3)as a potential prognostic factor for recovery from the disease; and (4) to evaluate systemic extrapulmonary involvement.
Utility of metabolic imaging in asymptomatic patients
Several preclinical studieshave found that FDG-PET imaging may be useful to assess the immune response to viral infection. FDG-PET imaging can detect lymph node involvement by showing the presence of increased cellular activity in the mediastinum and axilla (drainage of damaged lung tissue), even in individuals without pathologic findings on CT or clinical manifestations after exposure to the virus. Studies in animal models have found a discreet increase in circulating monocytes in the affected lymph nodes, showing elevated cellular activity on day 5 of viral exposure. This finding is related to the role of monocytes in the immune response to viral infections. PET metabolic imaging with other non-FDG tracersmight provide information about which strains are involved in COVID-19 infection.
In animal models, some authors have found that FDG uptake is elevated in various lymph node stations before large-scale viral replication occurs. This finding suggests that FDG-PET imaging could be an especially useful diagnostic tool to detect early changes in the immune response to infection in asymptomatic patients, potentially playing a particularly important role in early phases of the disease and in the differential diagnosis.
Monitoring metabolic response to treatment
Another potential application of FDG-PET in COVID-19 patients is the potential to monitor treatment response and predict recovery time. Some correlation has been observed between high uptake of FDG in pulmonary lesions associated with SARSCoV-2 and recovery time for these patients. For example, patients with a standard uptake value (SUV) of 4.6 have been shown to recover in 17 d after symptom onset, vs 26 d in patients with a higher SUV (SUV = 12.2). However, a larger series of patients is needed to confirm the predictive value of SUV values for clinical recovery. In this regard, it would be valuable to quantitatively determine the relation between the SUV value and the expected recovery time.
Evaluation of systemic involvement
FDG-PET imaging can also be particularly useful in patients with SARS-CoV-2 to detect the presence of alterations in other organs, including the gastrointestinal tract,heart, kidneys, brain, and/or bone marrow. In some cases, a diffuse increase has been observed in bone marrow metabolic activity after COVID-19 infection. The chronic inflammation associated with COVID-19 has also been shown to affect both the brain and heart.
Complementary role of FDG-PET imaging to confirm morphologic abnormalities evidenced on CT
Various studies have found a correlation between morphologic abnormalities observed on CT with metabolic data obtained by FDG-PET imaging (Figure 4).However, the possible association between the topographic distribution of lesions observed on CT and the intensity of FDG metabolism needs to be evaluated in larger series of patients. It would be particularly useful to evaluate the possible relation between metabolic uptake and lung areas with greater or lesser ventilation(Figure 5). It appears that areas with greater ventilation are more likely to present higher infiltration of inflammatory cells.
CONCLUSION
There is much we still do not know about the pathophysiology and clinical course of COVID-19 infection. However, the presence of certain patterns on CT and PET-CT scans may facilitate diagnosis and help to select the appropriate treatment.
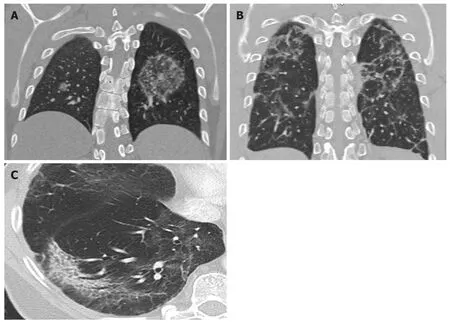
Figure 4 Computed tomography findings late stage disease. A: Reverse halo or atoll sign: Rounded opacity in the left lung with ground-glass attenuation in the center demarcated by a denser, fine ring. Small, homogeneous rounded opacity in the right lung; B: Bilateral perilobular pattern: Polygonal (irregular, linear or band-like) peripheral opacities in secondary pulmonary lobules; C: Peripheral, elongated, curved consolidation in the right lower lobe containing dilated bronchi.

Figure 5 A 65-year-old patient with a history of invasive lepidic-predominant adenocarcinoma (stage pT1bNxM0) treated with surgery,chemotherapy and radiotherapy. A: Coronal computed tomography showing the crazy-paving pattern (with interstitial septal thickening and increased density of ground-glass opacities) with a markedly asymmetric bilateral distribution, mainly affecting the right side; B: Positron emission tomography-computed tomography(PET-CT) coronal section; C: Metabolic PET; D: Volume rendering 3D PET-CT; E: MIP, PET; B-E: Reveals increased cellular activity [standard uptake value (SUV) 4-6] related to the associated inflammatory process. PET-CT pattern of bilateral coronavirus disease 2019 (COVID-19) viral pneumonitis, predominantly right-sided; F:Axial computed tomography showing crazy-paving pattern (with interstitial septal thickening and increased ground-glass density) with a bilateral, but markedly asymmetric distribution, predominant right-sided; G and H: Axial section and 3D volume rendering from PET-CT metabolic imaging that reveals increased cellular activity (SUV 4-6) related to the associated inflammatory process. PET-CT pattern of bilateral, predominantly right-sided, COVID-19 viral pneumonitis.
 World Journal of Radiology2020年11期
World Journal of Radiology2020年11期
- World Journal of Radiology的其它文章
- Multimodality imaging in COVID-19 patients: A key role from diagnosis to prognosis