
Validation of the Persian version of the Compassionate Care Assessment Tool
2021-02-28 09:49AlikrVisiRygniAsghrDlvndiKinNouroziAsEdiMhdiRhgozrRostmJlliNderSlriAlirezAdi
Alikr Visi-Rygni ,Asghr Dlvndi ,Kin Nourozi ,As Edi ,Mhdi Rhgozr ,Rostm Jlli ,Nder Slri ,Alirez Adi ,*
a Department of Nursing,School of Nursing and Midwifery,Kermanshah University of Medical Sciences,Kermanshah,Iran
b Nursing Department,University of Social Welfare and Rehabilitation Sciences,Tehran,Iran
c Behavioral Sciences Research Center,Life Style Institute,Baqiyatallah University of Medical Sciences,Teheran,Iran
Keywords:Compassionate care Iran Nursing care Psychometrics Statistical factor analysis
ABSTRACT Objectives:The present study aimed to translate and determine the psychometric properties of the Persian version of the Compassionate Care Assessment Tool (CCAT) ?.Methods:The study was carried out to translate and validate of the CCAT?.After securing permission from the designer of the tool and translating it,the psychometric properties were determined through examining face validity,construct validity,internal consistency,and test/retest reliability.With regard to construct validity,confirmatory factor analysis was used so that 300 patients in internal and surgery wards were selected by a simple random sampling method from three hospitals.Data were analyzed using SPSS (v.24.0) and LISREL statistical software version 8.8.Results:The results of the confirmatory factor analysis supported the validity and reliability of the Persian version of the CCAT?and its four factors.The reliability of the tool and internal consistency were confirmed through test/retest method with two weeks’ interval.At the two areas of importance and provision of compassionate care,Cronbach’s α coefficient equaled to 0.918 and 0.933 and intraclass consistency equaled to 0.848 and 0.907 respectively.Conclusion:The results showed that the Persian version of the CCAT? was adequately valid and reliable for Iranian patients.Given the acceptable psychometric parameters of the tool,using it in future studies to measure importance and provision of compassionate nursing care to Iranian patients at internal and surgery wards is recommended.
What is known?
·Nursing care of patients should be holistic and compassionate care is a fundamental part of nursing care that named as the art of nursing.
·The Compassionate Care Assessment Tool(CCAT)?by Burnell is one of the tools specially designed to assess compassionate nursing from the patient’s perspective.
What is new?
·This study confirmed the validity and reliability of the Persian version of the CCAT?,which provides an instrument to evaluate compassionate care in viewpoints of patients in Iran.
1.Introduction
Companionate is the nursing profession’s foundation;indeed it is one of the professional standards of nursing performance[1].The American Nurses Association (ANA) defines compassion as a vital element and feature of nursing and a requisite for improvement of nursing care quality and patients’ recovery[2].
Compassion may have direct influence on the quality of care for the patient and the patients’ assessment of the nursing services is usually based on the compassion they feel in the care [3-5].Because of this,the terms“compassion”and“compassionate care”are usually used interchangeably in nursing literature to highlight the same meaning [6].Emotional compassion develops as a result of witnessing others’ pain and hardship and leads to attempts to help[7].Compassion begins with empathy and accomplishes with willingness and taking measure to decrease or remove the pain and suffering of others[5].It is defined as perception and awareness of others’ pain and willingness to remove it [8,9].
Compassion is not a mere feeling in nursing; it is a connection between the nurse and patient that may lead the measures and decisions taken by the nurse so that the outcome will be an outstanding clinical performance by the nurse[10].Compassionate nursing care means perceiving the pain and suffering of the patient and taking measures to decrease or remove the pain by adopting proper nursing intervention consistent with cultural backgrounds of patients and nurses[11].Gordon notes that compassionate care is a patient-centered process to examine the situation and program the care[12].Perry maintains that signs of compassionate nursing include being considerate and accurate in dealing with the patient’s problems,being committed to recognizing the patient,and attempting to remove the patient’s pain along with keeping a respectful relationship with the patient [13].
Thereby,compassionate nursing care is not limited to demonstrating empathy and dealing with the disease but also encompasses empowerment of patients along with providing appropriate nursing care through perceiving physical and emotional needs and emotional problems of patients [14-16].Compassionate nursing care may lead to establishing an effective relationship between the provider and receiver of the care,which results in faster recovery of the patient and better therapeutic results[17,18].It may also lead to higher satisfaction in the patients,safer care services,time and cost-saving,satisfaction in the personnel,sense of usefulness,higher self-confidence,and development of coping behavior in patients [17,19].Lack of compassion in providing care is an imperfection and a sign of the low quality of health care [20].Some consider it as the best and most valuable gift that a nurse can give a patient in health systems [9,21].It entails recognizing and perceiving the patients’ needs and expectations with compassionate care [22-24].Without patients’ feedback,nurses risk providing care only based on their professional perception and presumptions and neglecting patients ’ attitudes and viewpoints[25].Without feedback from patients as the receivers of care and failing to determine characteristics and behaviors perceived as compassionate nursing,it is not possible to supervise and assess compassionate nursing or determine its effectiveness[5,26,27].The Royal College of Nursing in the UK and the American Nursing Association (ANA) have emphasized supervising and assessing compassionate care provision as a priority for professional development,even if it challenges the status quo [2,28].
Wear and Zarconi believed that rather than the patient,nowadays,more emphasis is put on the diseases,and naturally,this approach leads to negligence of attitudes and needs of the patient[29].As recommended by research works,despite the importance and role of compassionate care in nursing,today’s nursing is unfortunately mostly based on quantitative evidences and clinical skills,while ethics and compassion are less emphasized [30-32].
Therefore,this aspect of nursing has been neglected and deemphasized as moral and arbitrary aspects of nursing [33]; so that this key need of the patient has been overshadowed [34].In this spirit,about 50% of patients in the USA in 2010 noted that compassion is a missing element of care services [10].
There are several hurdles in the way of promoting compassionate care and probably one of the most important of them is the absence of a valid and reliable tool to assess and monitor provision of compassionate care[34,35].It is essential to develop a valid and reliable tool to assess and monitor compassionate care in clinical settings [28,35].Several tools are available to assess compassion[2]; however,there are a limited number of tools to measure compassion in health personnel and provided care and in particular the care provided by nurses.One of the tools specially designed to assess compassionate nursing from the patient’s perspective is the Compassionate Care Assessment Tool (CCAT) ? by Burnell.The reason for choosing this tool was that it is specifically focused on assessing the importance and provision of compassionate care from the viewpoint of patients hospitalized in internal and surgery wards.In addition,the subscales of the tool provide better coverage of the concept of compassionate nursing care[34,35].The tool was designed by Burnell in 2011 with 28 statements to assess compassionate nursing care in cancer patients.Afterward,Burnell and Agen(2013)examined the tool’s validity for patients in the USA in internal and surgery wards.The new tools consist of 20 statements and four factors,including meaningful connection (eight statements),patients’ expectations (five statements),caring attributes (four statements),and capable practitioner (three statements) [9].
Despite the evidence about the direct relationship between low quality of care and lack of compassion and the weight of compassionate care as a construct in the nursing field that can be manipulated [34],it has been rarely dealt with in Iran.Explanations for this include the subjective and multi-aspect nature of the concept and the fact that is a function of cultural ground of the society.In addition,Iranian nurses are not completely familiarized with the concept,and there is no normalized and valid tool to measure it in Iran.This highlights the need for a valid and reliable tool to assess and survey the provision of compassionate nursing care in clinical settings.The present study is an attempt to translate and validate of the CCAT?for Iranian patients hospitalized in internal and surgery wards.
2.Material and methods
The study was carried out during May 2017 to September 2018 as a methodological work to translate the CCAT? into Persian and validate the tool for the patients hospitalized in internal and surgery wards.The study population was the patients hospitalized in three educational Kermanshah-based hospitals affiliated with Kermanshah University of Medical Sciences.Kermanshah city is home to the largest hospitals in the west of Iran and hosts patients from four neighboring provinces.To examine the validity of the tool,300 patients were selected through random cluster method from three hospitals in Kerman city.
Inclusion criteria were age range 18-65 years,minimum hospitalization term of three days,consent to participate in the study,Persian speaking and understanding abilities,no pain,and stable condition.The questionnaires not fully completed were excluded.
The proposed method by Wild et al.was followed to translate and validate the tool [36].At first,a written permission from the designer of the tool was secured,and then two translators translated it from English into Persian.Then the two versions of the questionnaire were compared and combined to obtain on translation.Afterward,the Persian version was translated into English by three translators (one of them was a native English speaker).The three English versions were compared by a supervisor and consistency with the original tool was confirmed.The designer also received a copy of the translated tool for confirmation.With confirmation by the designer of the CCAT?,the Persian version of the tool was examined in terms of face validity,construct validity,internal consistency,and test/retest reliability.Qualitative face validity of the tool was examined based on cognitive questions from 15 patients hospitalized in Kermanshah-based hospitals.The translated tool was provided to 15 patients,including both genders who had been hospitalized for at least three days in internal and surgery wards.They were asked to state their opinions about clarity,ease of understanding,and understandability of the statements.The Persian version passes this stage with minor alterations before confirmatory factor analysis.
For construct validity stage,the patients were first briefed about the objective and method of the study and an informed letter of consent was signed by them.Afterward,they were asked to fill out a demographical information form(age,gender,education,marital status,ward,the term of hospitalization,and hospitalization occasions in the past year).Then they were asked to fill out the CCAT?; each questionnaire was filled out in 25-30 min.The participants were asked to rank each one of 20 statements of the tool in terms of importance and provision of cares from the aspect covered by the statements.The statements were designed based on Likert’s four-point scale(not important till extremely important in term of importance and never to all of the time for provision of care).Confirmatory factor analysis was performed for both aspects of importance and provision of care.
Construct validity of the tool was examined in LISREL statistical software version 8.8 using confirmatory factor analysis to examine the goodness of fit of the tool’s factors.Several goodnesses of fit indices are available for this purpose,and it is recommended to use more than one index [37,38].Here,Squared-chi,Minimum Discrepancy Function by degrees of freedom divided (CMIN/DF),root mean square error of approximation (RMSEA),adjusted goodness of fit index (AGFI),incremental fit index (IFI),and comparative fit index (CFI) were used.
Internal consistency and test/retest reliability were examined in SPSS (v.24).To determine internal consistency,Cronbach’s α coefficient was computed for the whole tool and the subscales.To examine test/retest reliability and interclass consistency coefficient,30 patients hospitalized in internal and surgery wards of the three educational hospitals in Kermanshah City who met the inclusion criteria were selected to fill the tool two times in two weeks’ interval.These participants did not participate in the structural validity stage.
3.Results
Following translation and confirmation of the translation by the designer,face and structural validity construct validity were examined.In the case of face validity,the tool was examined by the patients in terms of clarity and simplicity.In construct validity,the collected data from 300 patients hospitalized in internal and surgery wards at three educational hospitals in Kermanshah city were analyzed.The mean age of the patients was 43.6±13.66 years with age range of 18-65.Among the patients,63.7%were men,56.3%did not have high school diplomas,and 51.0%were at the internal ward.Demographic characteristics of the participants are listed in Table 1.
About construct validity and confirmatory factor analysis for a tool with four factors in two areas of importance and provision of the services,the results showed that squared-chi to the degree of freedom (df) ratios were 2.768 and 2.464 respectively (P < 0.001)and RMSEA values were 0.083 and 0.070 respectively.For the rest of the indices including AGFI,CFI,NFI,IFI,and SRMR,goodness of fit was at acceptable level.Notably,these indices were higher in the area of importance of the services.Concerning AGFI,the goodness of fit was not acceptable in none of the areas (Table 2).The conceptual model of provision and importance of compassionate care is provided in Figs.1 and 2.
Examining internal consistency of the Persian version of the CCAT? in the two areas of importance and provision of compassionate services from the participants’point of view indicated good internal consistency of the whole tool in the area of importance of services (Cronbach’s α=0.918).All the aspects except for “competent practitioner” had a high internal consistency,higher than 0.7;this might be due to the small number of statements (three statements).In the area of provision of services,the tool had an excellent internal consistency(Cronbach’s α=0.933).In addition,all the three subscales had good internal consistency higher than 0.7(Table 3).
The results of test/retest with two weeks’ interval showed intraclass consistency coefficient in the areas of importance and provision of compassionate cares were 0.848 and 0.907 respectively(Table 4).
4.Discussion
In this study,the validity and reliability of the Persian version of the CCAT?were supported.Confirmatory factor analysis results for the CCAT? supported acceptable goodness of fit of the tool in the two areas of importance and provision of services.Thus,the Persian version of the CCAT? with four factors and 20 statements is supported in terms of structural validity.
With regard to the reliability of the tool,stratified internal consistency index -i.e.,an estimate of consistency of scores from two or more evaluations to measure a quantitative index -indicated that the tool and the four factors had an acceptable consistency in the two areas of importance and provision of services from the patients’ point of view.In addition,the internal consistency of the whole CCAT? and its four factors was acceptable based on Cronbach’s α coefficient in the two areas of importance and provision of services.These findings are consistent with Burnell’s study(2013),which obtained Cronbach’s α > 0.7 for the whole tool and four factors[9].
Sinkler et al.(2017) evaluated the compassionate assessment tools in health services and showed that one of the weaknesses of the available tools is the lack of validation in different societies and cultures [34].The present study deals with this disadvantage.As the results showed,the CCAT? is a reliable,valid,and replicable tool.Since providing care with compassion is part of nurses’ job,provision of compassionate services is a key element in satisfaction of patients with nursing cares and provision of quality health services to patients [39-42].Assessing patients’ satisfaction with compassionate nursing care is a reliable way to enable nurses to understand patients’ needs and expectations with regard to cares.This measure constitutes the centerpiece in the provision of proper and timely services [43-45].
A literature review showed that compassion is a function of culture [46],and the dominant culture in society affects how compassionate behaviors are formed [47].Therefore,nurses’ behaviors are a function of culture so that compassionate behaviorsand behavioral specifications that demonstrate compassion in nurses are affected by traditions,customs,culture,values,beliefs,and sociopolitical structure of the society [18,33,48,49].The dominant culture in Iran is Iranian-Islamic culture,and nursing is assumed as worshiping.There are verses in the Holy Quran and hadiths about the value of looking after patients,which is the main job of nurses.That is,when a nurse provides cares with religious intentions to a patient,their job becomes a holy and heavenly job and resemblance of the best deeds.Therefore,it is highly fruitful to examine and perceive the aspects and specifications of compassionate nursing care in clinical settings based on cultural and social differences between Iranian-Islamic and Western societies and highlight the deep effects of these differences on the perception and expectation of patients with compassionate care.This highlights the need for and recommends conducting qualitative studies to better understand different and unknown aspects of the concept of compassionate nursing.Among the limitations of the present study was the lack of a suitable tool for Iranian society to conduct criterion-related validity examination.
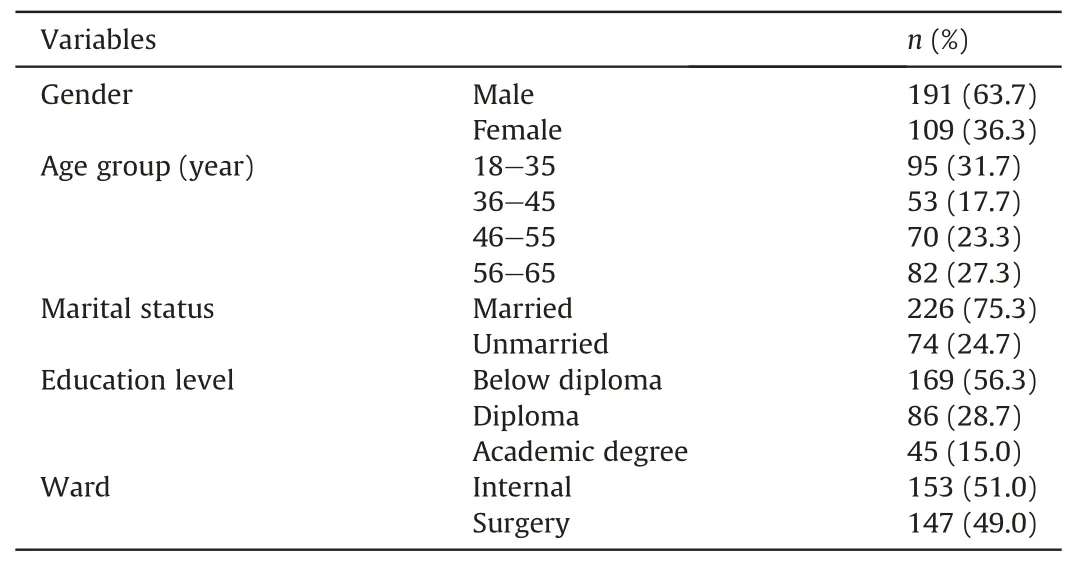
Table 1 Demographic characteristics of the participants (n=300).

Table 2 Goodness of fit indices of confirmatory factor analysis of the Persian version of the Compassionate Care Assessment Tool.
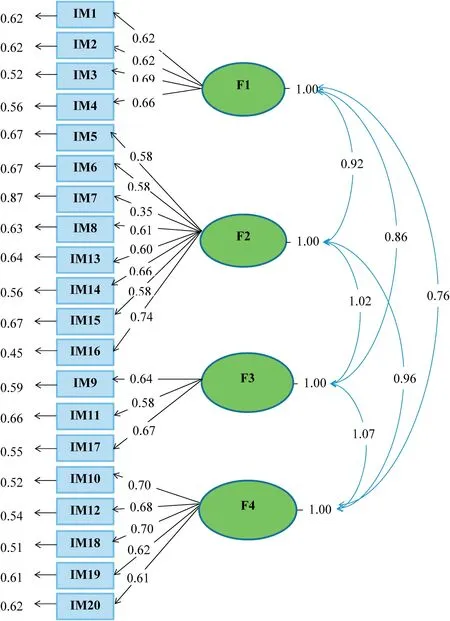
Fig.1.The conceptual model of the importance of compassionate care.F=Factor.IM=Importance.

Fig.2.The conceptual model of the provision of compassionate care.F=Factor.PR=Provision.
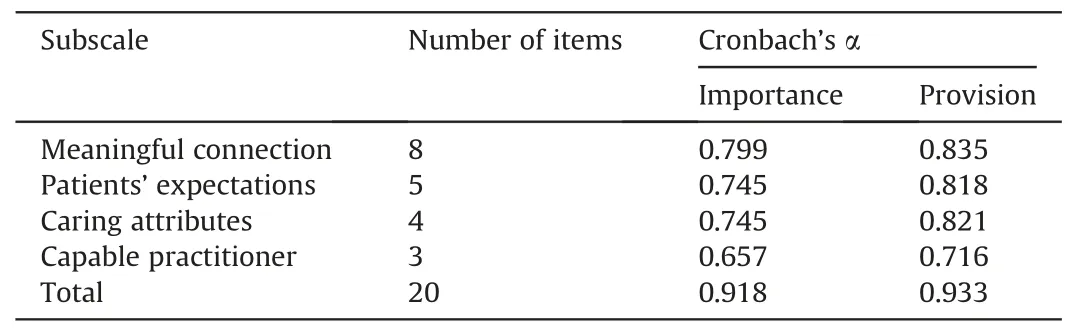
Table 3 Internal consistency of the Persian version of the Compassionate Care Assessment Tool and subscales in the area of provision and importance of compassionate care.
5.Conclusion
This study confirmed the cultural validation of the CCAT.As to the advantages of the tool examined in this work,it is notable that provision of compassionate nursing care was evaluated by the patients at internal and surgery wards.Thus,the collected information helps us gain deeper understanding of the needs and expectations of patients with reception of compassionate cares and the amount of such services to meet the needs and expectations of patients.
Ethics approval and consent to participate
The study is confirmed by research ethics committee of University of Social Welfare and Rehabilitation.(IR.USWR.REC.1396.250).
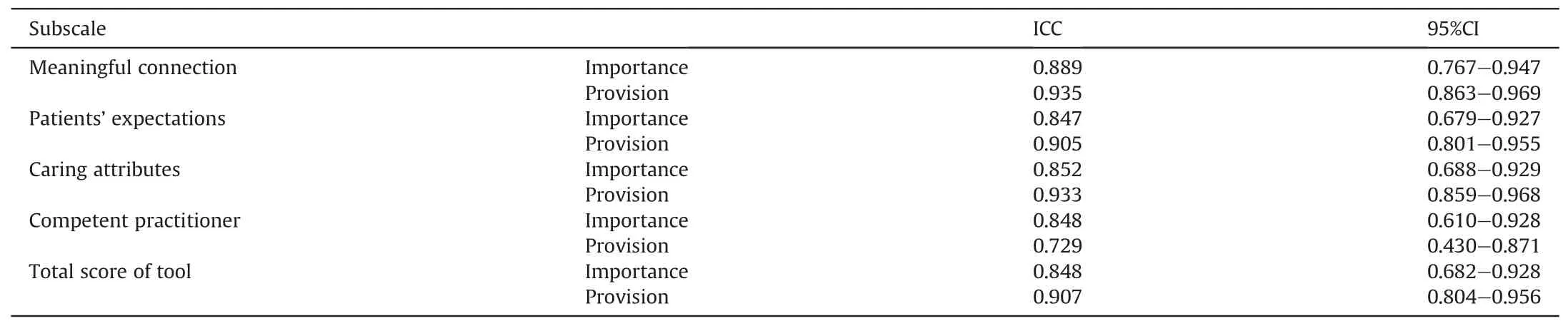
Table 4 Intraclass correlation of the Persian version of the Compassionate Care Assessment Tool and subscale.
Availability of data and material
Data available by contacting the corresponding author.
Funding
The study was funded by the University of Social Welfare and Rehabilitation.
CRediT authorship contribution statement
Aliakbar Vaisi-Raygai:Conceptualization,Data Curation,Methodology,Writing Original Draft,Writing-Review& Editing.Asghar Dalvandi:Supervision,Conceptualization,Methodology,Writing Original Draft.Kian Nourozi:Conceptualization,Methodology,Writing Original Draft.Abbas Ebadi:Conceptualization,Methodology,Writing Original Draft,Validation,Formal Analysis.Mahdi Rahgozar:Conceptualization,Methodology,Writing Original Draft,Validation.Rostam Jalali:Conceptualization,Methodology,Writing Original Draft,Validation.Nader Salari:Conceptualization,Methodology,Writing Original Draft,Formal Analysis,Software.Alireza Abdi:Conceptualization,Methodology,Writing Original Draft,Data Curation,Writing-Review& Editing,Software.
Declaration of competing interest
The authors declare that they have no conflict of interest.
Acknowledgement
The present paper is part of a PhD dissertation in nursing approved by the University of Rehabilitation Medical Sciences.The authors wish to express their gratitude to all participating patients for their contribution and the Department of Research of Tehran University of Social Welfare and Rehabilitation for their support of the study plan.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2020.12.004.
 International Journal of Nursing Sciences2021年1期
International Journal of Nursing Sciences2021年1期
- International Journal of Nursing Sciences的其它文章
- Focuses and trends of the studies on pediatric palliative care:A bibliometric analysis from 2004 to 2018
- Relationship between negative emotions and perceived support among parents of hospitalized,critically ill children
- The effect of digital health technologies on managing symptoms across pediatric cancer continuum:A systematic review
- Effectiveness of animal-assisted therapy on pain in children:A systematic review and meta-analysis
- Effects of creative expression program on the event-related potential and task reaction time of elderly with mild cognitive impairment
- Struggling to live a new normal life among Chinese women after losing an only child:A qualitative study