
Therapeutic massage for knee osteoarthritis:a systematic review and meta-analysis of randomized controlled trials
2021-10-27 08:27XingHua邢華ShenJiayun沈佳韻GongLi龔利YaoFei姚斐LiJianhua李建華ShaoSheng邵盛ChuYuzhou儲(chǔ)宇舟HePengfei何鵬飛ChenHao陳浩
Xing Hua (邢華), Shen Jia-yun (沈佳韻), Gong Li (龔利), Yao Fei (姚斐), Li Jian-hua (李建華), Shao Sheng (邵盛),Chu Yu-zhou (儲(chǔ)宇舟), He Peng-fei (何鵬飛), Chen Hao (陳浩)
1 Department of Tuina, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200437, China
2 Department of Acupuncture, Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai 201203, China
3 Shanghai University of Traditional Chinese Medicine, Shanghai 201203, China
Abstract
Keywords: Tuina; Massage; Anti-Inflammatory Agents, Non-Steroidal; Osteoarthritis, Knee; Meta-analysis; Systematic Review; Randomized Controlled Trials
Knee osteoarthritis (KOA) is a degenerative disease caused by multiple factors. It is the leading cause of disability among older adults. In China, research has shown that 85% of people over 65 years have KOA[1]. It has a serious impact on the patients’ quality of life and the morbidity has continuously increased due to aging of the population[2].
Therapeutic massage (tuina) is an external therapeutic method in traditional Chinese medicine (TCM) that involves performing manipulations under the guidance of meridian theory[3-4]. Therapeutic massage manipulation is a general term for any type of standardized technique performed on the human body with the use of hands, other parts of the body, specific tools, and appliances[5-7]. It has been widely applied in orthopedic diseases, such as lumbar disc protrusion,cervical spondylopathy, and KOA[8-10]. Many literature works show that therapeutic massage has a great effect on KOA[11-13]. However, due to language limitations, the trials of therapeutic massage for KOA were not included in the study of guidelines, such as the American Academy of Orthopaedic Surgeons (AAOS), Osteoarthritis Research Society International (OARSI), and American College of Rheumatology (ACR).
Medical care should be based on the doctor’s professional judgment, sufficient clinical evidence, and the patient’s circumstances to provide more benefit to the patient[14]. The recommendation of manual therapy was inconclusive in AAOS 2013, and non-steroidal antiinflammatory drugs (NSAIDs) were strongly recommended. However, therapeutic massage was not included in this guideline. There is an urgent need of additional safe and effective treatments for KOA.Therapeutic massage is safer than NSAIDs, and it is a type of physical therapy with a low risk for serious side effects[15-16]. Given its safety, whether therapeutic massage is more effective than NSAIDs in treating osteoarthritis of the knee is a highly relevant question.
The objective of our study was to conduct a systematic review and meta-analysis for evaluating the efficacy of therapeutic massage for KOA, with NSAIDs as the control.
1 Methods
1.1 Data sources and search strategy
Since therapeutic massage is mainly studied in China,we incorporated 4 major Chinese databases into our search strategy. We searched the Chinese National Knowledge Infrastructure (CNKI), Wanfang Academic Journal Full-text Database (Wanfang), Chongqing VIP Database (CQVIP) and China Biology Medicine Disc(CBM), Cochrane Library, and PubMed databases up to September 2019 to identify randomized controlled trials(RCTs), and the key words included tuina, therapeutic massage therapy, manual therapy, manipulation,physical therapy, massage, KOA, NSAIDs, ibuprofen,celebrex, drug, knee osteoarthritis , and knee pain, which were used independently or in combination for full-text retrieval. For example, the search terms used in PubMed are listed in Table 1. Two evaluators individually selected the studies and resolved any disagreements by discussion. After selection, the evaluators analyzed the abstracts of the selected articles to determine whether it should be included.
1.2 Inclusion and exclusion criteria
We only included RCTs published prior to September 1, 2019, with no language restrictions. Patients should have a clear diagnosis of KOA. Trials were required to compare therapeutic massage with NSAIDs, and trials comparing therapeutic massage with any other intervention were excluded. The therapeutic massage therapy should be only based on meridian theory. In addition, the Western Ontario and McMaster Universities osteoarthritis index (WOMAC) and total effectiveness should be included in the outcome measures of the study. We excluded RCTs of therapeutic massage combined with physical therapy or joint mobilization. We considered three outcomes, including pain, stiffness, and function. RCTs were excluded if the publication was only in abstract form.
1.3 Data extraction and quality assessment
We assessed the characteristics of the original research and extracted the data based on our study design. When the data were not provided in publications,we contacted the authors for details. Two reviewers independently extracted the data and assessed the quality of each trial. Inter-rater reliability was satisfactory(r≥90). The methodological quality of the RCTs was evaluated based on the Cochrane Collaboration’s risk of bias tool (Handbook 5.1)[17], which includes selection bias, performance bias, detection bias, attrition bias, and reporting bias, and each item contains three risk levels.
1.4 Therapeutic massage assessment
There is no consensus on how to evaluate therapeutic massage treatment in RCTs. Studies of therapeutic massage standardization have not yet produced a unified result. According to previous research, we used a method evaluating the adequacy of the following three aspects of therapeutic massage treatment: choice of manipulation and acupoints, frequency and duration of treatment, and experience of the doctor. However, this was just based on previous studies, and we used it to preliminarily evaluate therapeutic massage. The evaluation method needs to be improved further[18-20].
1.5 Data synthesis and analysis
WOMAC was treated as a continuous outcome, and total effectiveness as a dichotomous outcome. At the same time, WOMAC was divided into WOMAC pain,WOMAC stiffness, WOMAC function, and WOMAC total score in this review to assess different aspects. Metaanalysis was performed by Review Manager 5.1 computer software whenever there were sufficient data available in the studies. AP-value of less than 0.05 represented statistical significance for the overall effect.AP-value of less than 0.1 indicated statistical significance for heterogeneity between studies. To evaluate statistical heterogeneity,I2tests were used for all outcomes in our study. We consideredI2≤50 as low heterogeneity,I2>50,but <75 as moderate heterogeneity, andI2≥75 as significant heterogeneity. A fixed effects model was used if the heterogeneity was low or moderate; otherwise, we used a random effects model. If there was a lack of statistical significance for an overall effect, the confidence interval (CI) was evaluated for the potential trends that may suggest the tendency for an increase or decrease in the overall effect. If the heterogeneity was significant, we performed sensitivity analysis and explained the potential reasons for heterogeneity. We used risk ratio (RR) for dichotomous data and mean difference (MD) for continuous variables. For continuous variables, we used intra-group differences before and after treatment. When the difference was not available,the following formula was applied (Figure 1).
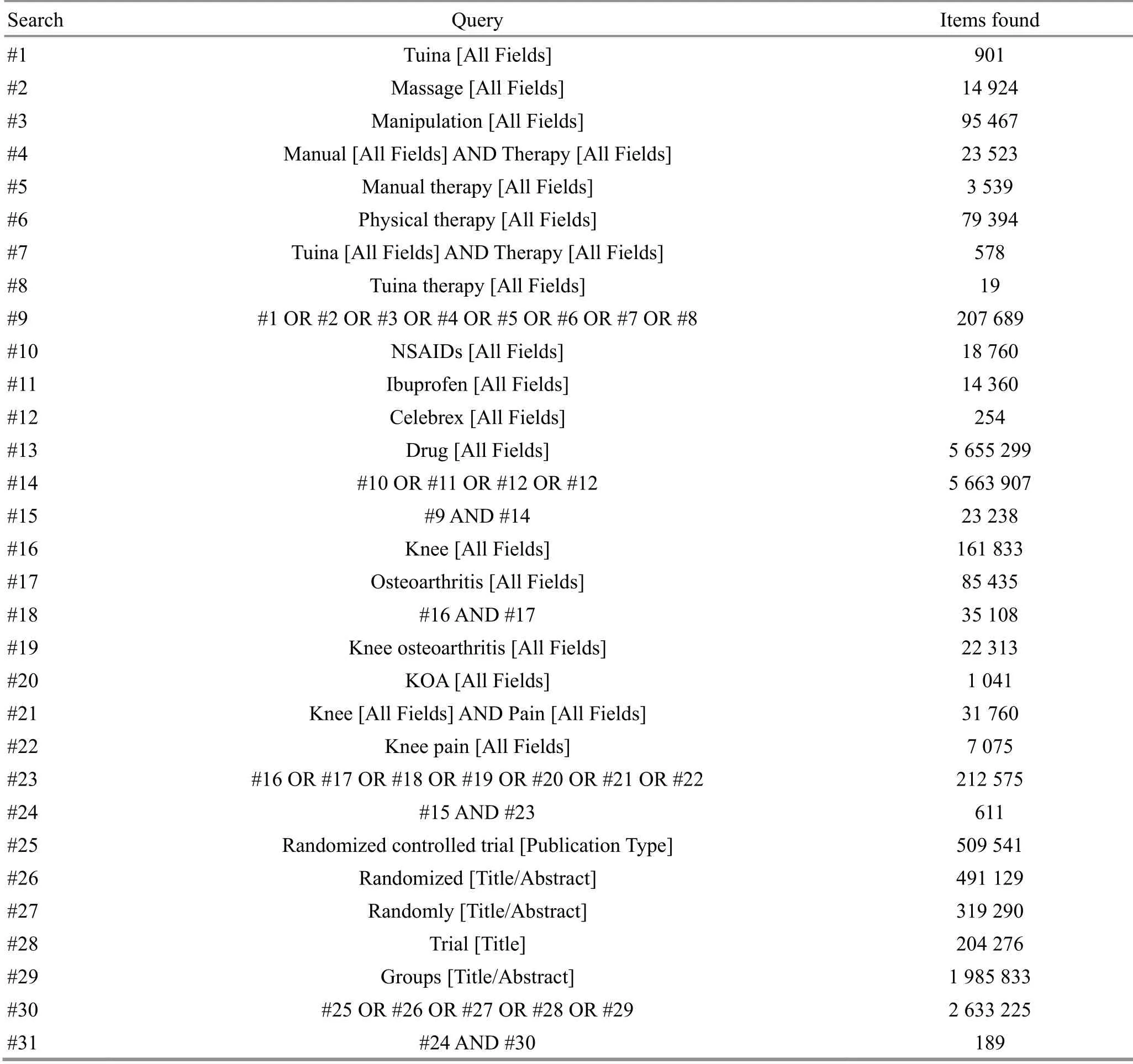
Table 1. Search strategies for PubMed

Figure 1. Formula used when the difference was not available
2 Results
According to our search strategy, a total of 6 710 papers were identified initially, including 1 564 papers from CNKI, 923 papers from CQVIP, 2 833 papers from Wanfang, 971 papers from CBM, 189 papers from PubMed, and 230 papers from Cochrane Library. After removal of duplicates and screening of full-text articles,8 papers were included and all these papers were in Chinese (Figure 2). The characteristics of the included studies are listed in Table 2.
All the studies were published in Chinese, involving a total of 711 participants: 355 in the therapeutic massage(observation) group and 356 in the NSAIDs (control)group (Table 3).
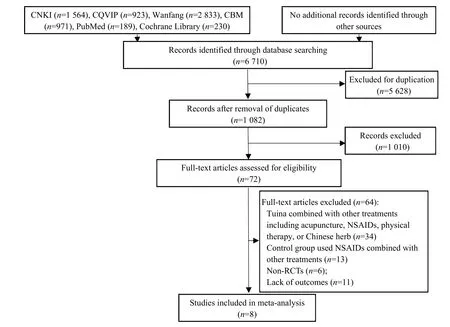
Figure 2. Flow chart of study selection
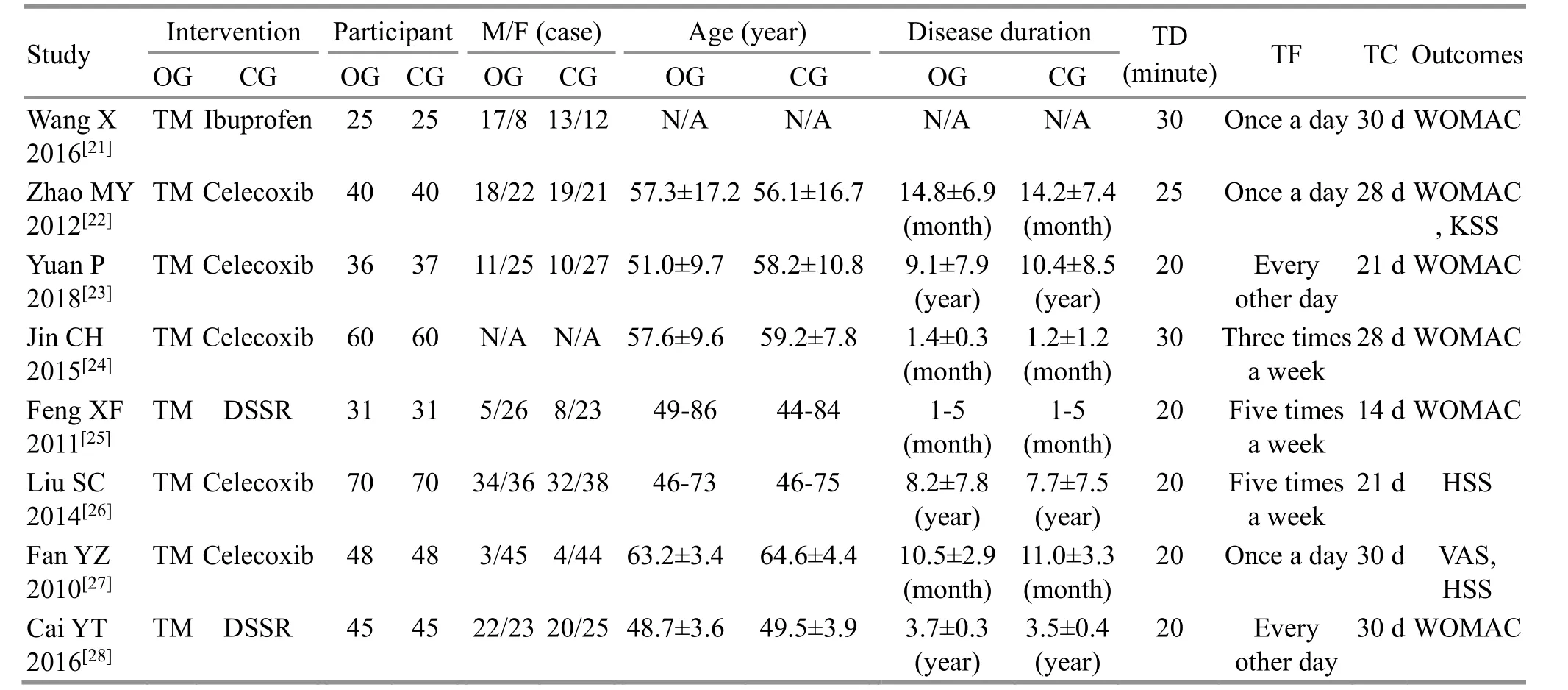
Table 2. Characteristics of the included studies
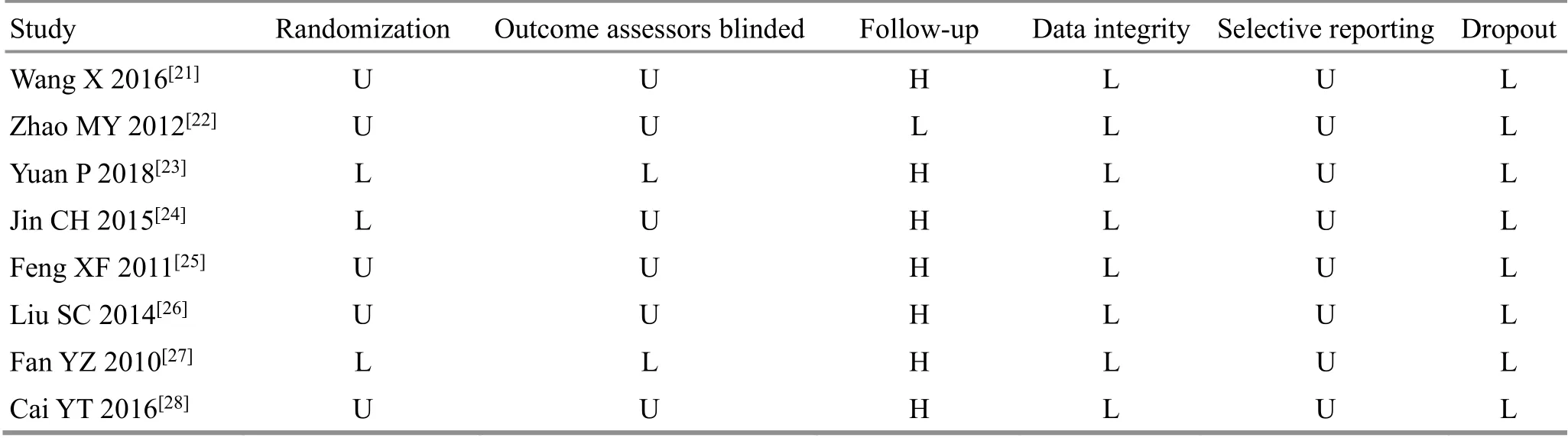
Table 3. Quality assessment of the included studies
The eight included studies were of average quality.Two studies missed describing the baseline data[21,24],while two studies only roughly described the mean age and the duration of disease[25-26]. However, all baseline data were analyzed. Only three of these studies specified the randomization method[23-24,28], and all these studies used the random number table method. Due to its particularity, therapeutic massage was unable to be blinded to the patients. However, two studies mentioned about outcome blinding[23,28]. All studies clearly described the inclusion and exclusion criteria. Dropout and loss to follow-up were not mentioned in any of the studies. All studies reported the outcomes completely.Other sources of bias were unclear (Figure 3 and Figure 4).
2.1 Total effectiveness
Total effectiveness is a professional way to judge the effect of Chinese medicine. It is usually measured using four levels, namely cured, effective, improved, and ineffective. Total effectiveness contains the first three levels, and it is judged based on theCriteria of Diagnosis and Therapeutic Effect of Diseases and Syndromes in Traditional Chinese Medicine[29]. In this article, seven studies[22-28]measured the total effectiveness in a total of 661 participants, 330 in the observation group and 331 in the control group. The meta-analysis did not show significant heterogeneity (I2=0%,P=0.44). Therefore, a fixed effects model was used. The results showed that therapeutic massage was more effective than NSAIDs comparing the total effectiveness [RR=1.14, 95% CI (1.07,1.21),P<0.0001], (Figure 5).
2.2 WOMAC
WOMAC can reflect pain, stiffness, and function of the joint. There are 24 questions in this scale, and it has been widely used to describe the severity of KOA. In this review,we evaluated the effectiveness of therapeutic massage in terms of the three aspects covered by WOMAC. The lower the score, the greater the improvement in symptoms.
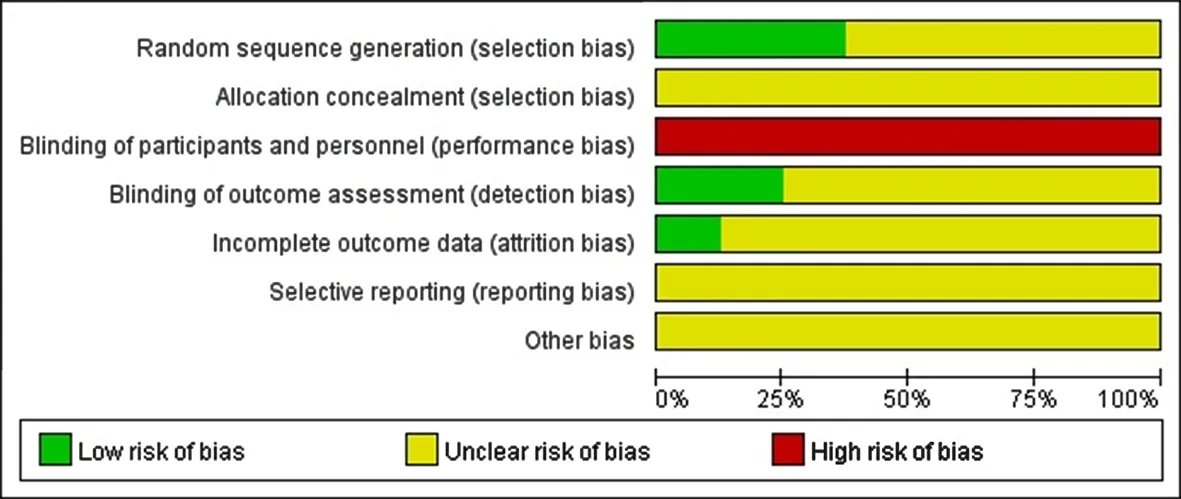
Figure 3. Cochrane risk of bias of the included studies (n=8)
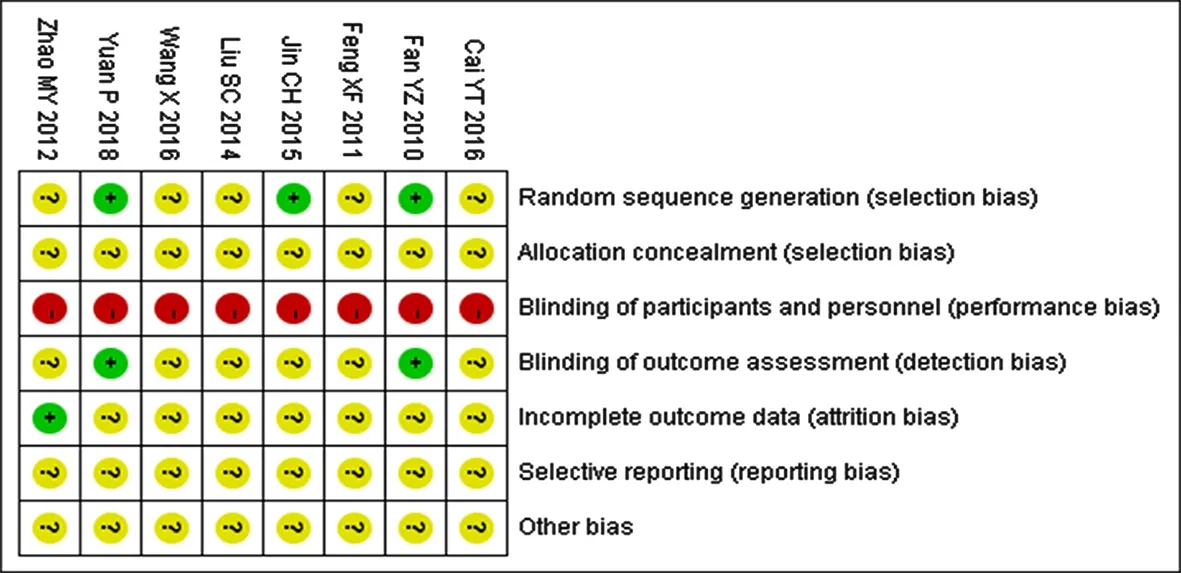
Figure 4. Comparison of the total effectiveness between therapeutic massage and NSAIDs for KOA (661 participants)
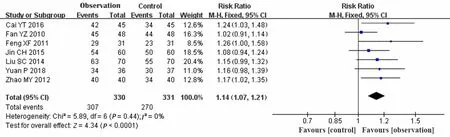
Figure 5. Comparison of the total effectiveness between therapeutic massage and NSAIDs for KOA (661 participants)
2.2.1 Pain
Four articles[23-25,28]reported WOMAC pain score. A total of 345 participants were involved, 172 in the observation group and 173 in the control group. The meta-analysis showed significant heterogeneity (I2=91%,P<0.00001). We considered that the heterogeneity should originate from different pain thresholds of the patients. At the same time we found that the treatment duration also greatly affected the feeling of pain.Therefore, two articles with a treatment period of one month were excluded. The meta-analysis showed low heterogeneity (I2=0%,P=0.71), and thus we used a fixed effects model for analysis. The results showed that therapeutic massage had significant advantage in reducing the pain in KOA compared with NSAIDs[MD=-2.06, 95%CI (-2.75, -1.36),P<0.00001], (Figure 6).Jin CH[24]considered that therapeutic massage contributed equally as NSAIDs, while the other three studies[23,25,28]thought that therapeutic massage was better than NSAIDs.
2.2.2 Stiffness
Four articles[23-25,28]took WOMAC stiffness score as an outcome measure. A total of 345 participants were involved, 172 in the observation group and 173 in the control group. The meta-analysis did not show significant heterogeneity (I2=15%,P=0.32). Therefore, we used a fixed effects model. The results showed that therapeutic massage was more effective than NSAIDs in relieving stiffness in KOA [MD=-0.90, 95%CI (-1.05, -0.75),P<0.00001], (Figure 7).
2.2.3 Function
Three articles[23,25,28]took WOMAC function score as an outcome measure. A total of 225 participants were involved, 112 in the experiment group and 113 in the control group. The meta-analysis did not show significant heterogeneity (I2=0%,P=0.72). Therefore, we used a fixed effects model. The results showed that therapeutic massage was more effective than NSAIDs in improving daily function of patients with KOA [MD=-12.48, 95%CI(-13.91, -11.05),P<0.00001], (Figure 8).

Figure 6. Comparison of the WOMAC pain score between therapeutic massage and NSAIDs for KOA (135 participants)
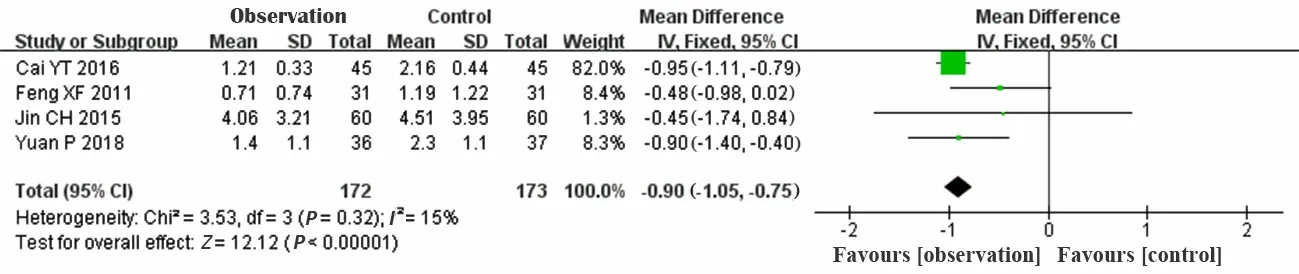
Figure 7. Comparison of the WOMAC stiffness score between therapeutic massage and NSAIDs for KOA (345 participants)

Figure 8. Comparison of the WOMAC function score between therapeutic massage and NSAIDs for KOA (225 participants)
2.2.4 WOMAC general score
Six articles[21-25,28]reported WOMAC general score. A total of 475 participants were involved, 237 in the observation group and 238 in the control group. The meta-analysis showed significant heterogeneity (I2=99%,P<0.00001). Then we did subgroup analyses according to three different treatment times, 20 min, 25 min and 30 min, respectively. The 20 min subgroup showed low heterogeneity (I2=6%,P=0.35) and the 30 min subgroup showed moderate heterogeneity (I2=65%,P=0.09).Therefore, we used a fixed effects model. The results showed that therapeutic massage had significant advantage in improving the symptoms of KOA compared with NSAIDs when the treatment lasted 20 to 25 min[MD=-16.87, 95%CI (-17.68, -16.07),P<0.00001]. When the treatment lasted 30 min, NSAIDs may be better than therapeutic massage regarding the WOMAC general score [MD=3.02, 95%CI (1.78, 4.26),P<0.00001],(Figure 9).
2.3 Sensitivity analysis
Sensitivity analysis was performed by changing the effects model in the software, and WOMAC general scores showed differences afterwards. The difference was considered from the clinic. Everyone has his own evaluation of pain and function, and it will make a big difference for 24 questions in WOMAC scale. At the same time, the treatment plan of therapeutic massage manipulation also varies slightly, which may lead to a different result. This also reflects the necessity of therapeutic massage standardization in research.Another sensitivity analysis showed that each group had a little difference after change of the analysis model. This indicated a low sensitivity, and the small-sample studies had a little effect on the combined effect. The stability of the meta-analysis was high (Table 4).
3 Discussion
KOA causes pain and loss of joint function, leading to decreased quality of life. Because of the high prevalence in China, it has become very urgent to identify an effective treatment for KOA. Up to date, the most common treatment for KOA is NSAIDs, and they are strongly recommended in most of the mainstream guidelines. However, their side effects are serious, as they may affect liver and kidney functions, and some patients cannot take these drugs due to allergy. Studies showed that therapeutic massage could improve the lower limb alignment, increase the strengths of quadriceps and hamstrings to reduce pain, and improve joint function[30-34]. Therapeutic massage has mainly been studied in China, and there are thousands of articles studying therapeutic massage treating KOA in Chinese. Due to the language problem, these trials were not considered in either American or European guidelines. To determine whether therapeutic massage has a reliable curative effect on KOA, this article conducted a systematic review and meta-analysis by searching pertinent RCTs. The purpose of this study was to provide reliable evidence for treating KOA with therapeutic massage.
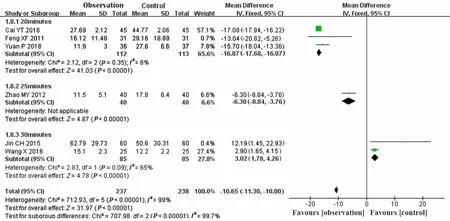
Figure 9. Comparison of the WOMAC general score between therapeutic massage and NSAIDs for KOA (475 participants)
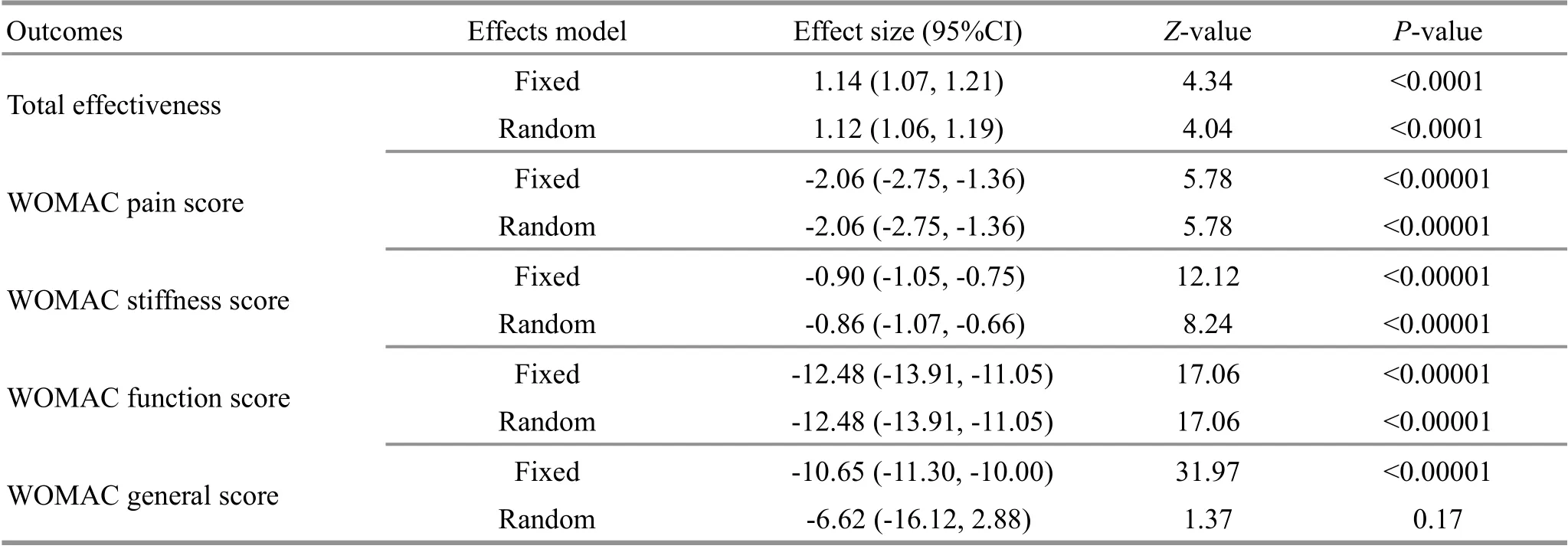
Table 4. Sensitivity analysis
Eight RCTs were finally included in the meta-analysis.All studies were in Chinese and they included a total of 831 participants, 415 in the therapeutic massage(observation) group and 416 in the NSAIDs (control)group. We adopted total effectiveness and WOMAC score as the outcome measures. At the same time, we divided WOMAC into three parts to evaluate the pain,stiffness, and function. Among them, seven studies were included in the meta-analysis total effectiveness; two studies were included in the meta-analysis of WOMAC pain and stiffness scores, and for WOMAC function score,three studies were included in the meta-analysis. Metaanalysis of the total effectiveness showed that therapeutic massage was more effective than NSAIDs. In relieving the pain, stiffness and improving function of the knee, therapeutic massage was superior to NSAIDs.However, the effect may depend on treatment time. This conclusion needs more in-depth research to confirm.
However, the following shortcomings may weaken the above-mentioned conclusion. Firstly, therapeutic massage is difficult to perform blinding, and there may be a placebo effect, causing a performance bias.Secondly, only three trials reported the randomization method, while the remaining trials only mentioned‘randomization’, suggesting that there may be a selective bias. Thirdly, the means to evaluate therapeutic massage has not yet reached any consensus. The quality of therapeutic massage depends on many factors, such as experience, duration, frequency, and force, and thus, the quality of therapeutic massage treatments varied from trial to trial. Fourthly, the publication language of these eight studies was Chinese, suggesting that there may be a publication bias. Fifthly, none of the eight studies reported follow-up, and none of them described whether there were other sources of bias.
The heterogeneity was still moderate in WOMAC, and we could not eliminate the heterogeneity according to the sensitivity analysis and subgroup analysis. Therefore,it was considered clinical. WOMAC is a subjective evaluation of patients’ knee symptoms and everyone’s pain threshold is different. A significant heterogeneity may weaken the conclusion. In future research, we need to include more objective indicators, such as muscle strength, gait analysis, and electromyography, to improve the study quality. Besides, we should develop more stringent inclusion and exclusion criteria to include RCTs of a high quality.
Therapeutic massage is an external therapeutic method in TCM that involves performing manipulations under the guidance of meridian theory. It is also called Chinese massage. Various manipulation techniques have been developed based on the different ways of acting,operation position, direction, intensity, and duration.This treatment option consists of basic manipulation and the selection of acupoints. Therefore, the treatment may be different even for the same disease. It is necessary to develop standardization for therapeutic massage to assess the quality of treatment.
The current research has faced many problems, and more rigorous RCTs are needed in future studying therapeutic massage for KOA. According to this metaanalysis, future investigations should improve the methodological quality from the following aspects:randomize the group and clarify the randomization method; design a placebo group to rule out the placebo effect; both patients and researchers should be blinded to the treatment and outcome measures;standardization of therapeutic massage should be carried out as soon as possible; more details about therapeutic massage should be considered, such as force,frequency, and the experience of doctors; prioritize multi-centered and large sample-sized RCTs with an adequate follow-up. All of these factors will influence the outcome.
4 Conclusion
Therapeutic massage was more effective than NSAIDs comparing the total effectiveness. In relieving pain and stiffness and improving function of the knee, therapeutic massage was superior to NSAIDs. However, the effect may depend on treatment time. More multi-centered and large sample-sized RCTs are needed to verify the result.
Conflict of Interest
All authors declare that there are no conflicts of interest regarding the publication of this paper.
Acknowledgments
This work was supported by the General Project of National Natural Science Foundation of China (國(guó)家自然科學(xué)基金面上項(xiàng)目, No. 8197151584); Three-year Action Plan to Promote Clinical Skills and Clinical Innovation Capabilities of Municipal Hospitals (“促進(jìn)市級(jí)醫(yī)院臨床技能與臨床創(chuàng)新能力” 三年行動(dòng)計(jì)劃, No.SHDC2020CR3096B); the Innovation Ability Project of Shanghai University of Traditional Chinese Medicine (上海中醫(yī)藥大學(xué)研究生創(chuàng)新能力項(xiàng)目, No. Y2019079).
Authors’ Contributions
Xing Hua and Shen Jia-yun contributed equally to this work; Gong Li designed and supervised the study; Xing Hua, Shen Jia-yun, and Li Jian-hua contributed to literature search; Yao Fei, Shao Sheng, Chu Yu-zhou, He Peng-fei,and Chen Hao were responsible for the review and selection of trials and extraction of data. Xing Hua, Shen Jia-yun, Li Jian-hua, Yao Fei, and Chu Yu-zhou contributed to data analysis and interpretation. Xing Hua and Shen Jia-yun wrote the manuscript; Gong Li and Yao Fei revised the paper; all authors approved the final version of this article and the author list.
Received: 6 March 2020/Accepted: 4 August 2020
猜你喜歡
山東中醫(yī)藥大學(xué)學(xué)報(bào)(2022年5期)2022-10-26
陜西中醫(yī)藥大學(xué)學(xué)報(bào)(2022年4期)2022-08-01
中學(xué)生學(xué)習(xí)報(bào)(2022年14期)2022-04-15
化工管理(2021年7期)2021-05-13
信息化建設(shè)(2019年2期)2019-03-27
西安航空學(xué)院學(xué)報(bào)(2018年5期)2018-10-15
中國(guó)氣象科學(xué)研究院年報(bào)(2017年0期)2017-07-19
北方音樂(lè)(2017年4期)2017-05-04
 Journal of Acupuncture and Tuina Science2021年5期
Journal of Acupuncture and Tuina Science2021年5期
- Journal of Acupuncture and Tuina Science的其它文章
- Exploring the effect of acupuncture plus mild hypothermia on miRNA-204 and its target gene expressions in CIRI rat brain tissues based on MAPK signal pathway
- Experimental observation of effects of acupoints,cone numbers and durations of moxibustion with different moxibustion methods on skin surface and inside temperature
- Clinical efficacy observation of ‘Tong Du Yun Pi’manipulation for infantile diarrhea in autumn
- Clinical observation on moxibustion therapy plus tuina in treating children with recurrent respiratory tract infections due to qi deficiency of spleen and lung
- Effects of acupuncture plus language training on language function and cerebral blood flow in patients with motor aphasia after ischemic stroke
- Efficacy and effect on related brain-gut peptides of acupoint sticking therapy for functional dyspepsia