
Scleral tunnel leakage induced by injection of dexamethasone intravitreal implant for recurrent Vogt-Koyanagi-Harada disease: a case report
2021-12-17 02:41YingHuangBingLinLiNaGeXiaoLingLiu
Ying Huang, Bing Lin, Li-Na Ge, Xiao-Ling Liu
Eye Hospital and School of Ophthalmology and Optometry,Wenzhou Medical University, Wenzhou 325027, Zhejiang Province, China
Dear Editor,
We present a case of scleral tunnel leakage induced by injection of dexamethasone intravitreal implant(Ozurdex?) for recurrent Vogt-Koyanagi-Harada (VKH)disease. Written informed consent was obtained by the patient to allow publication of the present case and any related image and this case study is in accordance with the tenets of the Declaration of Helsinki.
VKH is a cell-mediated autoimmune disease that causes granulomatous panuveitis[1]. VKH patients need prolonged corticosteroid and immunosuppressant therapy, especially for recurrent patients[2]. Ozurdex, an approved dexamethasone intravitreal implant, is proved to be effective for VKH[3].A customized drug delivery system (DDS) of Ozurdex is used in our hospital. Basically, a preloaded dose of 700 mg dexamethasone is injected transconjunctivally by a 22-gauge(22G) needle through a small scleral puncture, which is oblique to cause a scleral tunnel into the vitreous cavity, avoiding an additional surgical suturing of the insertion site[4]. The scleral tunnel cannot be well-sealed in this recurrent VKH case; hence an additional suturing is needed to stop the leakage.
A 19-year-old male with a history of VKH presented to our hospital with complaints of blur vision in both eyes for 1mo.Ophthalmic examination revealed that his visual acuity was 0.25 of right eye and 0.1 of left eye. Intraocular pressure was 7.8 mm Hg of right eye and 11.7 mm Hg of left eye. He was then diagnosed as recurrent VKH in both eyes. The patient suffered recurrences for three years ago when he was first diagnosed. A long-term immunosuppressant, and oral and topical corticosteroid therapy were given for the past three years. In this visit, we gave him local corticosteroid eye drops,oral corticosteroid, and cyclosporine. In addition, Ozurdex was intravitreal injected into the left eye through a sclera tunnel 3.5 mm inferotemporal away from the limbus.
Three days later, the visual acuity of the left eye dropped to 0.04, and the intraocular pressure was 1.3 mm Hg. The inferotemporal conjunctiva was flat, no pinhole or edema was found when we pressed it by cotton swab. The anterior chamber was deep. However, in the fundus examination,wrinkles were found in the retina and choroid (Figure 1A).B-ultrasound indicated that the axis of the left eye was short,and the echo of the left eyeball was thickened and sunken(Figure 1B). We then opened the infratemporal conjunctiva for sclera exploration and found the oblique scleral tunnel unsealed (Figure 2). We sutured the scleral tunnel. One day later, the visual acuity was improved up to 0.3, intraocular pressure was 6.4 mm Hg, the retinal and choroidal folds disappeared (Figure 1C), and echo of the eyeball returned to be normal (Figure 1D).
A rapid drop of visual acuity and intraocular pressure after surgery, along with retinal and choroidal folds, leads to three possible diagnoses: choroidal detachment, ciliary body detachment and scleral tunnel leakage. Choroid was attached according to the B-ultrasonography. Ciliary detachment usually causes a shallow anterior chamber, which is not seen in the patient. So, sclera tunnel leakage is the most likely case. Choiet al[5]found that 7.5% patients who accepted 23G vitrectomy needed scleral suture. Kimet al[6]found that the incidence of 23G incision leakage was 6.7%-35%. Lakhanpalet al[7]found 10 of 140 patients with 25G vitrectomy needed to be sutured.Tunnel leakage was not completely avoided in 23G or 25G vitrectomy. Moreover, DDS of Ozurdex is 22G. This case suggested that we should pay close attention to the incision leakage in the short-term follow-up after injection.
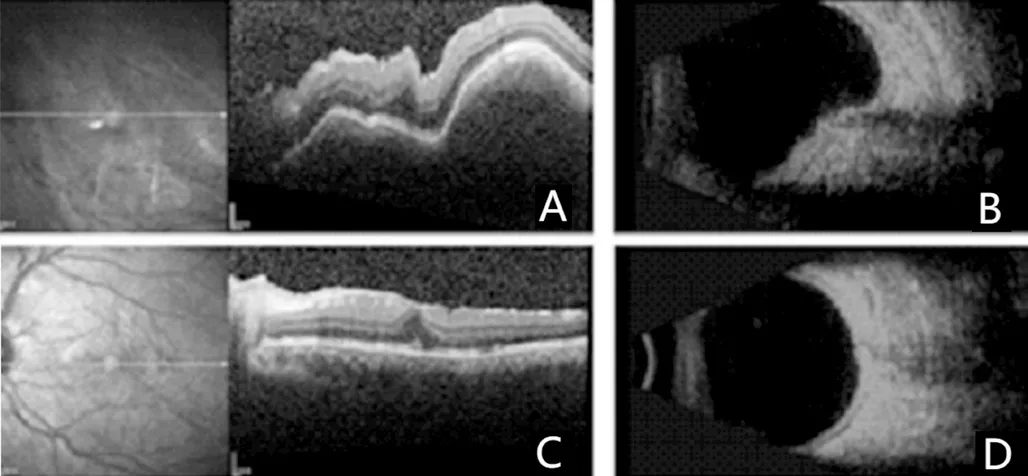
Figure 1 Fundus examination and B-ultrasound A: Wrinkles were found in the retina and choroid; B: B-ultrasound indicated that the axis of the left eye was short, and the echo of the left eyeball was thickened and sunken; C, D: One day later, the retinal and choroidal folds disappeared and echo of the eyeball returned to be normal.
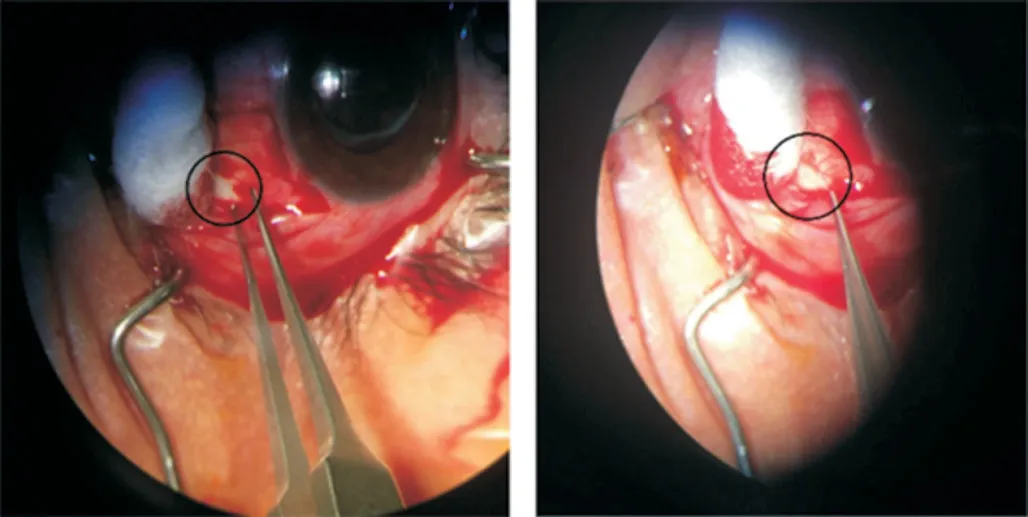
Figure 2 The oblique scleral tunnel unsealed.
A 21-year-old female was reported that suffered scleral malaria after 2y VKH treatment with oral corticosteroid and corticosteroid eye drops[8]. A 38-year-old female patient with Behcet’s disease was reported that suffered scleral malaria due to long-term corticosteroid and immunosuppressive therapy[9].This patient suffered recurrent VKH disease and took oral corticosteroid and local corticosteroid eye drops for a long time. We speculated the following reasons for the unhealed sclera incision: first, the long-term use of corticosteroid inhibits the activity of collagen fiber or fibroblast, which are essential for wound healing. Second, the chronic VKH inflammation may affect mechanical properties of the sclera, and eventually soften the sclera.
ACKNOWLEDGEMENTS
Conflicts of Interest:Huang Y, None; Lin B, None; Ge LN,None; Liu XL, None.
 International Journal of Ophthalmology2021年12期
International Journal of Ophthalmology2021年12期
- International Journal of Ophthalmology的其它文章
- Upregulation of ASPP2 expression alleviates the development of proliferative vitreoretinopathy in a rat model
- Mesenchymal stem cell-derived exosomes inhibit the VEGF-A expression in human retinal vascular endothelial cells induced by high glucose
- Protective effects of umbilical cord mesenchymal stem cell exosomes in a diabetic rat model through live retinal imaging
- New technique for removal of perfluorocarbon liquid related sticky silicone oil and literature review
- Quantitative analysis of retinal vasculature in normal eyes using ultra-widefield fluorescein angiography
- Evaluation of the long-term effect of foldable capsular vitreous bodies in severe ocular rupture