
Qualitative study on influencing factors of refusal of gastric tube placement in stroke patients with dysphagia
2022-02-15 04:54AoYangLiDongPangYangLiuLuSiWangYuHuanZhang
Nursing Communications 2022年13期
Ao-Yang Li, Dong Pang, Yang Liu, Lu-Si Wang, Yu-Huan Zhang*
1the Second Affiliated Hospital of Harbin Medical University, Heilongjiang 150086, China.
Abstract Objective: To explore the influencing factors of patients with dysphagia after stroke who refuse to accept gastric tube implantation, and to provide intervention basis for improving the compliance of patients with gastric tube implantation. Methods: A semi‐structured interview method was used to conduct in‐depth interviews with 11 patients who refused gastric tube placement, and the interview data were analyzed by Colaizzi analysis method. Results: The influencing factors of patients with dysphagia after stroke can be summarized into the following three themes: patient factors (patient's cognition of disease, patient's subjective pain perception and fear), family factors (patient's caregiver's cognition of disease, economic conditions) and medical factors (trust in medical staff, medical education methods).Conclusion: Medical staff should understand the influencing factors of dysphagia after stroke and take positive measures to improve the compliance of patients with gastric tube placement and ensure the treatment effect.
Keywords: stroke; dysphagia; gastric tube insertion; treatment decision; qualitative research
Background
Dysphagia is a common complication of stroke, and its incidence rate is 37% to 78.0% [1].in new onset patients, with a mortality rate of 29% to 37% [2]. Studies have shown that early gastric tube implantation can improve the nutritional status of patients, reduce stress ulcer, pulmonary infection and other complications, improve the prognosis of patients, and reduce the length of hospital stay [3, 4].However, after clinical investigation, we found that patients with dysphagia after stroke refused gastric tube placement, and the rejection rate was as high as 75.2% (167/222). However, there is no research on the influencing factors of gastric tube refusal in patients with dysphagia after stroke, which cannot help or effectively promote the treatment decision of gastric tube insertion in patients with dysphagia after stroke. Therefore, this study uses qualitative research,through personal in‐depth interviews to collect data, to explore the influencing factors of gastric tube placement in patients with dysphagia after stroke, and to provide reference for the construction of intervention scheme for the treatment decision of gastric tube placement in patients with dysphagia after stroke suitable for China's national conditions.
Object and method
Research objects
This study used the method of purposive sampling, selected patients with dysphagia after stroke from December 2020 to January 2021 in a tertiary hospital in Harbin, Heilongjiang Province as the research object. Inclusion criteria: ① stroke patients; ② According to the diagnosis, the score of Wa Tian drinking water test was 3 or above; ③Age > 18 years old; ④ Normal spirit, clear consciousness, can communicate with people normally; ⑤ Volunteer to participate in this study. Exclusion criteria: Patients with obvious physiological defects and major diseases, such as severe heart stroke, nervous system disease and motor organ disease. In this study, the basic information of patients was obtained through the electronic medical record system, and the interviewee's name was replaced by serial number.The sample size was no new topic, and the information reached saturation.
Research methods
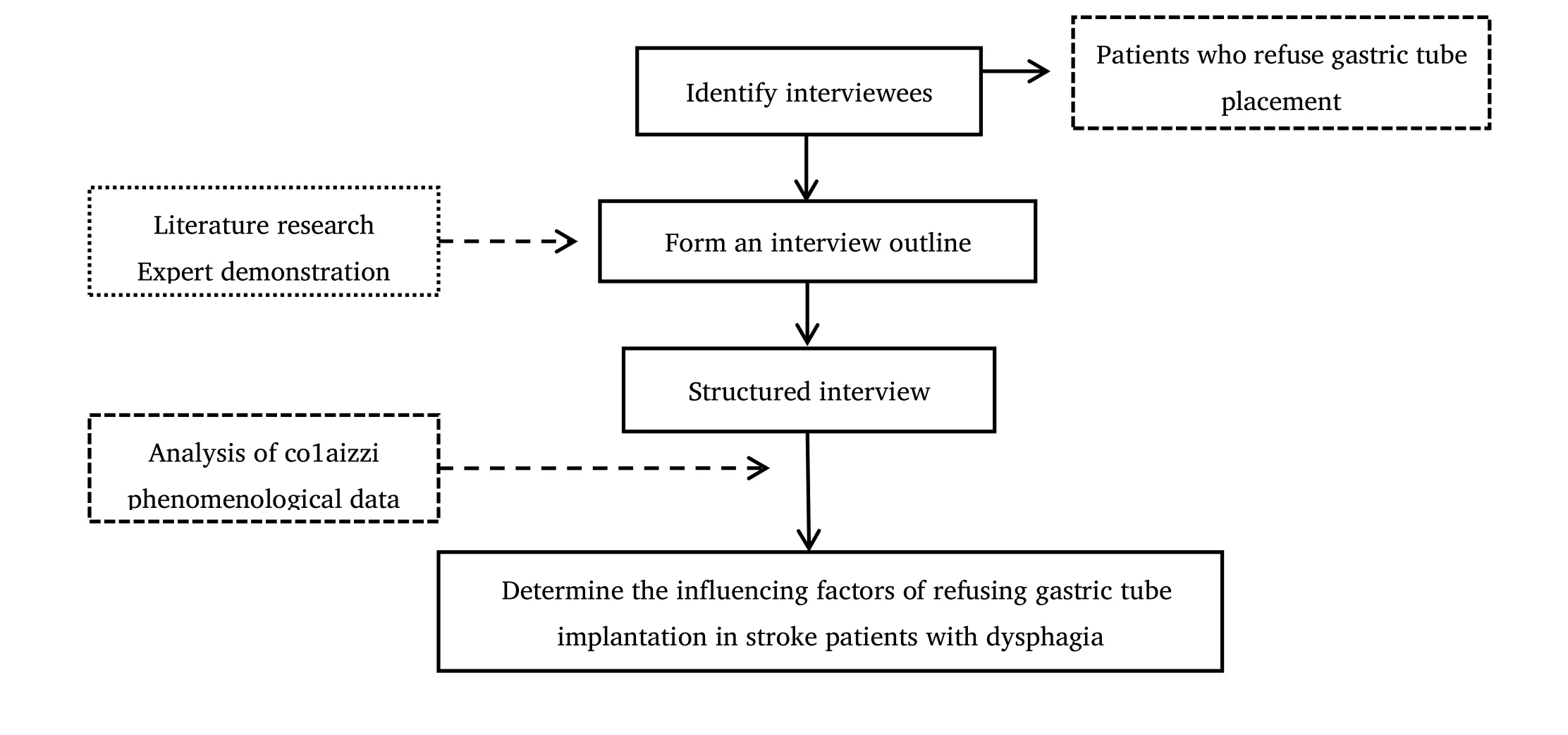
Data collection methods This study uses semi‐structured interviews to collect data. Face to face interview was used to explain the purpose, significance and process of the study to the subjects before the interview. All patients signed the informed consent. Record the whole process of the interview, and promise the patient that the interview recording is only used for academic research, and his personal privacy will be strictly confidential.
In order to ensure the scientificity and effectiveness of the interview, an experienced clinical nurse (supervisor nurse, 17 years of clinical work experience, three‐level psychological counselor) was selected. After obtaining the permission of the research object, the interview was conducted in a quiet place with the method of individual in‐depth interview, and the interview content was recorded synchronously. Before the interview, the interview outline was compiled according to the literature review and expert opinions. Two patients were selected for pre interview to adjust and determine the interview outline. The outline is as follows: can you understand the medical staff's information about gastric tube? Do you know the corresponding disease risk caused by refusal of gastric tube? What causes you to refuse to have a gastric tube? What was your family's attitude when you refused to take down the gastric tube?
Data analysis and collation
Within 24 hours after the end of the interview, the recording was transcribed into text information, and the text materials were sorted out and improved. Data analysis adopted co1aizzi's 7‐step analysis method of phenomenological data. An interviewer and another researcher familiar with qualitative research checked the transcription and collation of the original data and data, coded and classified them independently, and extracted the theme from them. When they had different opinions, they reached a consensus through group discussion. According to the principle of data saturation, 11 patients,aged from 36 to 77, were interviewed. General information is shown in Table 1.
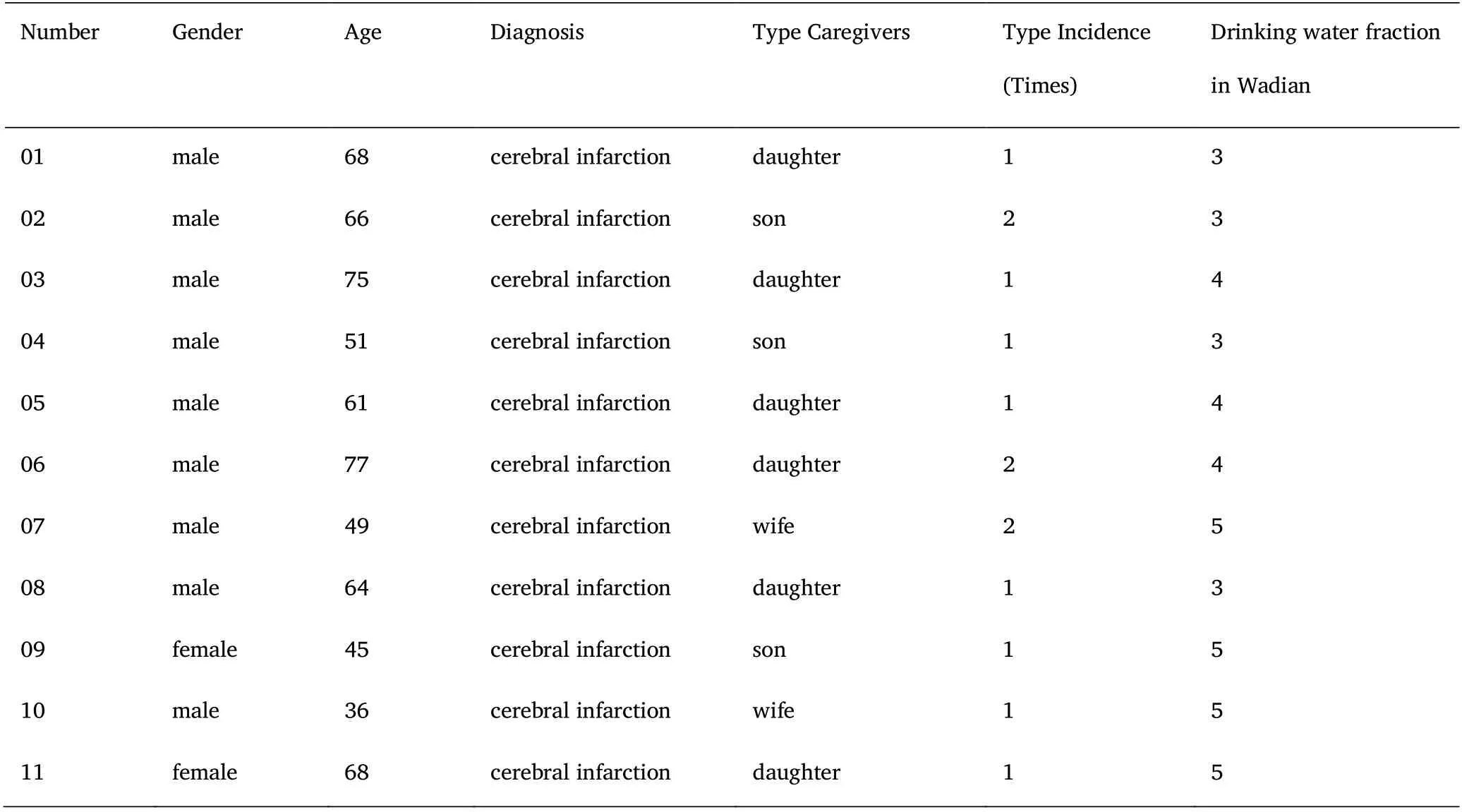
Table 1 general information of subjects (n = 11)
Results
Topic 1: patient factors Patients' cognition of disease
Most of the respondents said that they are in good physical condition and feel that they don't need to go down the gastric tube. Interviewee 06: "I think I should have no problem eating, just eat slowly."Interviewee 03: "I can eat slowly and pay more attention to myself. I don't think I need to go down the gastric tube." Interviewee 02 said,"Choking is not a problem, just pay attention to it."
Patients' subjective pain perception and fear
Most of the respondents were afraid of the inferior gastric tube.Interviewee 05: "I've seen other people put down their stomach tubes.It's terrible to think about it." Interviewee 08: "I didn't know the meaning of gastric tube before. After the nurse told me the general process of gastric tube, I said that I would not do anything. I felt that I was suffering too much." Interviewee 02: "I agreed before, but after the nurse came to me with a gastric tube, I had to go back. I was so scared."
Theme 2: family factors Cognition of patients' caregivers on diseases
Most of the interviewees said that their families didn't think it was necessary to have a gastric tube. Interviewee 11: "I discussed with my family that I didn't want to have a gastric tube, and my family also said that I could eat slowly and I didn't need to have a gastric tube."Interviewee 04: "Compared with my disease, my family feels that choking is a small problem. We should pay more attention to it."
Economic conditions
Some respondents said that they did not want to increase the additional financial burden of the family. Interviewee 09: "The conditions at home are not very good. Anyway, if you can eat some,you won't have to go down the gastric tube and save some treatment costs."
Theme 3: medical factors Trust in medical staff
The degree of trust in medical staff will affect patients' treatment decision to a certain extent. Interviewee 10: "I'm not familiar with that nurse. I'm afraid she's not good at it and it hurts to insert it for me."Interviewee 07: "The nurses who came to explain to me introduced the necessity of gastric tube placement, but I think they are trying to increase additional income."
Medical education mode
The way medical staff explain the disease affects the treatment decision of patients. Interviewee 01: "The nurse who is responsible for receiving me told me that I need to have a gastric tube, but what she said is too professional for me to understand."
Discussion
The disease cognition of patients and caregivers is an important factor affecting patients' gastric tube placement
In this study, patients' and caregivers' cognition of the disease has a serious impact on the treatment decision of gastric tube placement in stroke patients, which is consistent with the research results of Fu Yanhui [5], whose research shows that patients' cognition of the disease has a direct impact on their willingness to participate in the selection of treatment options. As an important source of disease information, medical staff play an important role in improving the disease awareness of patients and their family caregivers [6].Therefore, medical staff should talk about the importance and significance of gastric tube placement from different angles, so as to enhance the disease awareness of patients and their family caregivers.
Patients' subjective pain perception and fear are the main factors affecting patients' gastric tube placement
In this study, the subjective pain perception and fear of gastric tube placement were the main reasons for the respondents to refuse the treatment decision. Studies have shown that subjective pain perception is a conscious subjective experience, which can be transformed into an unpleasant emotional experience. Emotion is also a powerful driving force that affects patients' decision‐making process[7, 8]. One of the sources of patients' subjective pain perception and fear is limited cognition of the operation process of gastric tube insertion. In view of this, medical staff should be clear about the psychological experience of patients, and give targeted help, through professional psychological counseling, reduce fear [9, 10]. In addition,we should pay attention to guide the patients to correctly treat the possible discomfort symptoms of gastric tube implantation, so as to avoid the patients' withdrawal psychology due to temporary discomfort [11, 12]. However, it is undeniable that the operation of gastric tube insertion cannot avoid the pain and discomfort caused by it [13]. How to effectively reduce the pain caused by the operation is the top priority for medical staff to think about and solve.
Family economic factor is one of the factors that affect the placement of gastric tube
In this study, the family economic factors of patients are one of the influencing factors of treatment decision‐making. This is similar to the conclusion of Xie mengke's research [14], which indicates that patients will consider family economic conditions when making treatment decisions. The National Cancer Institute of the United States believes that it is necessary to evaluate the treatment decisions of patients from the economic aspect, especially the patients with poor family economic status, and the treatment cost and treatment benefit are its more concerned contents [15]. In view of this, when patients consider the economic cost of gastric tube placement, medical staff should discuss the necessity of gastric tube placement for patients'health and the importance of ensuring their life safety, so as to make them understand the benefit and value of the operation for patients'overall disease treatment.
The degree of trust in doctors and nurses and the way of propaganda and education of doctors and nurses are the main factors affecting patients' gastric tube placement
The results of this study show that patients' trust in medical staff will affect the treatment decision of gastric tube placement. Therefore, we should select the medical staff who are familiar, trusted, familiar and highly respected by patients as the recommender of gastric tube implantation treatment, so as to enhance patients' sense of trust in medical staff, so as to improve patients' enthusiasm to participate in treatment decision‐making and reduce decision‐making conflict [16,17]. In addition, peer education is an important way for patients to obtain knowledge [18]. Therefore, we should make full use of the demonstration and reference role of successful extubation patients in patients, and improve patients' treatment information and treatment belief. In addition, some patients in this study pointed out that the professional explanation of medical staff will increase the uncertainty of their understanding of gastric tube placement information.Therefore, medical staff should adapt to the patient's educational and cultural background and help patients correctly understand the positive significance of gastric tube placement through appropriate ways [19].
Summary
The reasons for patients with dysphagia after stroke to refuse gastric tube placement can be divided into three themes: patient factors(patient's cognition of disease, patient's subjective pain perception and fear), family factors (patient's caregiver's cognition of disease and economic conditions), and medical factors (trust in medical staff and medical education methods), The incidence rate of stroke is on the rise, and the factors that affect the gastric tube placement in patients with stroke can help the medical staff take targeted measures to improve the participation and compliance of the patients in the treatment of gastric tube placement and maximize the therapeutic benefits of the disease.
 Nursing Communications2022年13期
Nursing Communications2022年13期
- Nursing Communications的其它文章
- Delphi and Analytic hierarchy process for the construction of a risk assessment index system for post-stroke shoulder-hand syndrome
- A review of obstacles and facilitating factors of implementing Clinical Ladder Programs in nursing
- Spiritual health, empathy ability and their relationships with spiritual care perceptions among nursing students in China:A cross-sectional correlational study
- The influence of professional identity and ageism on turnover intention in nursing homes: a cross-sectional study from suzhou, China
- The relationship of family separation and nutrition status among under-five children: a cross-sectional study in Panti Public Health Center, Jember Regency of East Java, Indonesia
- Nursing cooperation related to thoracoscopic surgery in children