
Anti-SSA/SSB-negative primary Sj?gren’s syndrome presenting with hypokalemia: A case report
2022-03-02 06:46:28HaiyanTuShulingYueLijunMou
Hai-yan Tu, Shu-ling Yue, Li-jun Mou
1 Department of Nephrology, the Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou 310009,China
2 Guangzhou KingMed Center for Clinical Laboratory Co. Ltd., Guangzhou 510320, China
Dear editor,
Here we report a rare case of a patient presented with repeated hypokalemia and metabolic acidosis secondary to primary Sj?gren’s syndrome (pSS). Though no significantly raised titers of anti-SSA/SSB antibodies was detected in our case, minor salivary gland biopsy,kidney biopsy and positive Schirmer’s test confirmed the diagnosis of pSS.
CASE
A 57-year-old female initially presented with fatigue and weakness seven years ago. She was diagnosed with hypokalemia and was receiving therapy with potassium replacement. She had chronic hypokalemia leading to multiple visits to our emergency department for muscle weakness. These episodes were treated with potassium supplementation, with only transient improvement. She did not present the symptoms of xerophthalmia (dry eyes)or xerostomia (dry mouth) for the past years. Recently,the patient developed nocturia and progressive renal impairment (serum creatinine was 125 μmol/L). Then she was admitted to the nephrology department. Distal renal tubular damage was suggested by compensated metabolic acidosis. Her vital signs were unremarkable and no abnormal finding was identified on physical examination. Initial lab investigations revealed sodium 136 mmol/L, potassium 2.9 mmol/L, chloride 116 mmol/L, and bicarbonate 14.1 mmol/L (normal anion gap acidosis). A spot urine sample showed a pH of 7.0 and a positive anion gap (urinary sodium 5.1 mmol/L, potassium 34 mmol/L,and chloride < 5 mmol/L). On arterial blood gas analysis,the pH was 7.2 (7.35-7.45) and a normal anion gap.Trans-tubular potassium gradient (TTKG) was 10. The 24-hour urine calcium was 3.9 mmol/d (normal for her dietary intake). All of these findings were compatible with the diagnosis of distal renal tubular acidosis(RTA). Her autoantibody profile showed negative antimitochondrial, anti-smooth muscle, antineutrophil cytoplasmic antibodies (ANCA), rheumatoid factor(RF), cryoglobulin, gamma globulin and anti-doublestranded DNA antibodies. Anti-nuclear antibody, anti-SSA, and anti-SSB were also negative. Serum IgG was 4.77 g/L (7-16 g/L), serum IgA was 3.07 g/L (0.7-4.0 g/L),serum IgM was 0.6 g/L (0.4-2.3 g/L), serum IgG4 was 1.1 g/L (0.03-2.01 g/L), and serum light chain kappa/lambda ratio was 1.7 (1.35-2.65). Human immunodeficiency virus(HIV), hepatitis B (HBV), and anti-hepatitis C (anti-HCV)were negative. The high resolution computed tomography(HRCT) scan did not show pulmonary infiltrates or swollen lymph nodes. There was no history of eyes or mouth dryness. We did perform a Schirmer’s test and salivary gland biopsy. A positive Schirmer’s test occurred when 2 mm of the strip was wet after 5 min in both eyes.A salivary gland biopsy demonstrated multiple foci of lymphocyte and plasma cell infiltrate with ducts revealed intraepithelial lymphocyte infiltrate (Figure 1). Urinalysis showed 1+ albumin without associated hematuria and 24-hour urinary protein was 200 mg. Her serum albumin was 39 g/L and serum creatinine was 125 μmol/L. Renal ultrasound revealed normal-sized kidneys with preserved cortical thickness and corticomedullary distinction.As a progressive increase in her serum creatinine, she denied any recent illnesses. She underwent a kidney biopsy. Kidney biopsy showed multifocal lymphocytic and plasma cell infiltration in the renal interstitial tissues(Figure 2). Light microscopy showed tubular epithelial vacuolation and granular degeneration, protein tubular pattern, multifocal atrophy, multifocal lymphocytic and plasma cell infiltration of the renal interstitium with fibrosis, thickening of the arterial wall, and luminal stenosis. Direct immunofluorescent examination revealed no significant glomerular immune deposits. Transmission electron microscopy revealed no evidence of glomerular or extraglomerular electron-dense deposits. She was started on oral prednisolone at a dose of 15 mg daily to control the pSS and tapered over three months while the potassium replacement continued (potassium citrate was initiated at a dose of 30 mEq twice daily). She was discharged with the same dose of prednisolone. She was advised for regular follow-up in the nephrology clinic and responded well to the treatment symptomatically.Lab tests showed serum creatinine was 110 μmol/L, potassium 4.2 mmol/L, and negative proteinuria three months after discharge. The dose of prednisolone was tapered off to a minimum of 5 mg daily while the potassium replacement continued. However, she was lost to follow-up later.
DISCUSSION
Hypokalemia can cause life-threatening arrhythmia. The causes of hypokalemia can be occult and challenging to diagnose. It is caused by several underlying etiologies, namely, genetic, endocrine,gastrointestinal, and renal.Our patient had repeated episodes of hypokalemia and metabolic acidosis in the past, which responded symptomatically to potassium supplementation alone. The patient did not present the symptoms of dry eyes or dry mouth at the onset of the disease. She was also negative for anti-SSA/SSB antibody. Thus, she was labeled as a case of hypokalemic paralysis, but a detailed workup for the etiopathogenesis of her problem was missed. Distal RTA is the common pathway for potassium loss in a variety of diseases including connective tissue diseases such as Sj?gren’s syndrome (SS). The patient developed nocturia and progressive renal impairment (serum creatinine 125 μmol/L) with ocular and oral dryness, which prompted us to evaluate the possibility of SS as the root cause of her recurrent clinical problems. SS is an autoimmune disease characterized by lymphocytic infiltration of the exocrine glands, mainly the lacrimal and salivary glands, resulting in impaired secretory function. Renal involvement is seen in 5% of patients with SS, the most common of which is interstitial nephritis followed by distal RTA.
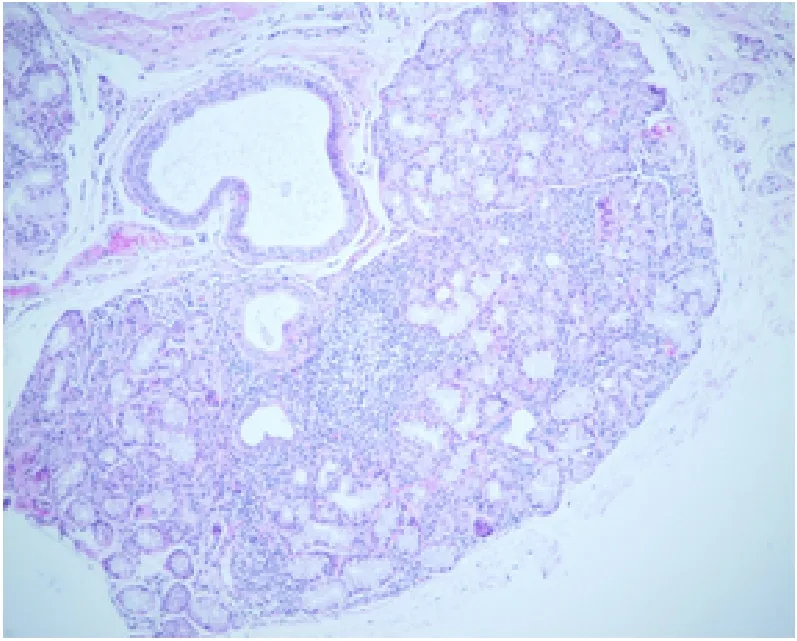
Figure 1. Multiple foci of periductal and intra epithelial mononuclear cell and lymphoplasma cell infiltrate are seen forming lymphoepithelial islands (lymphoid follicle).
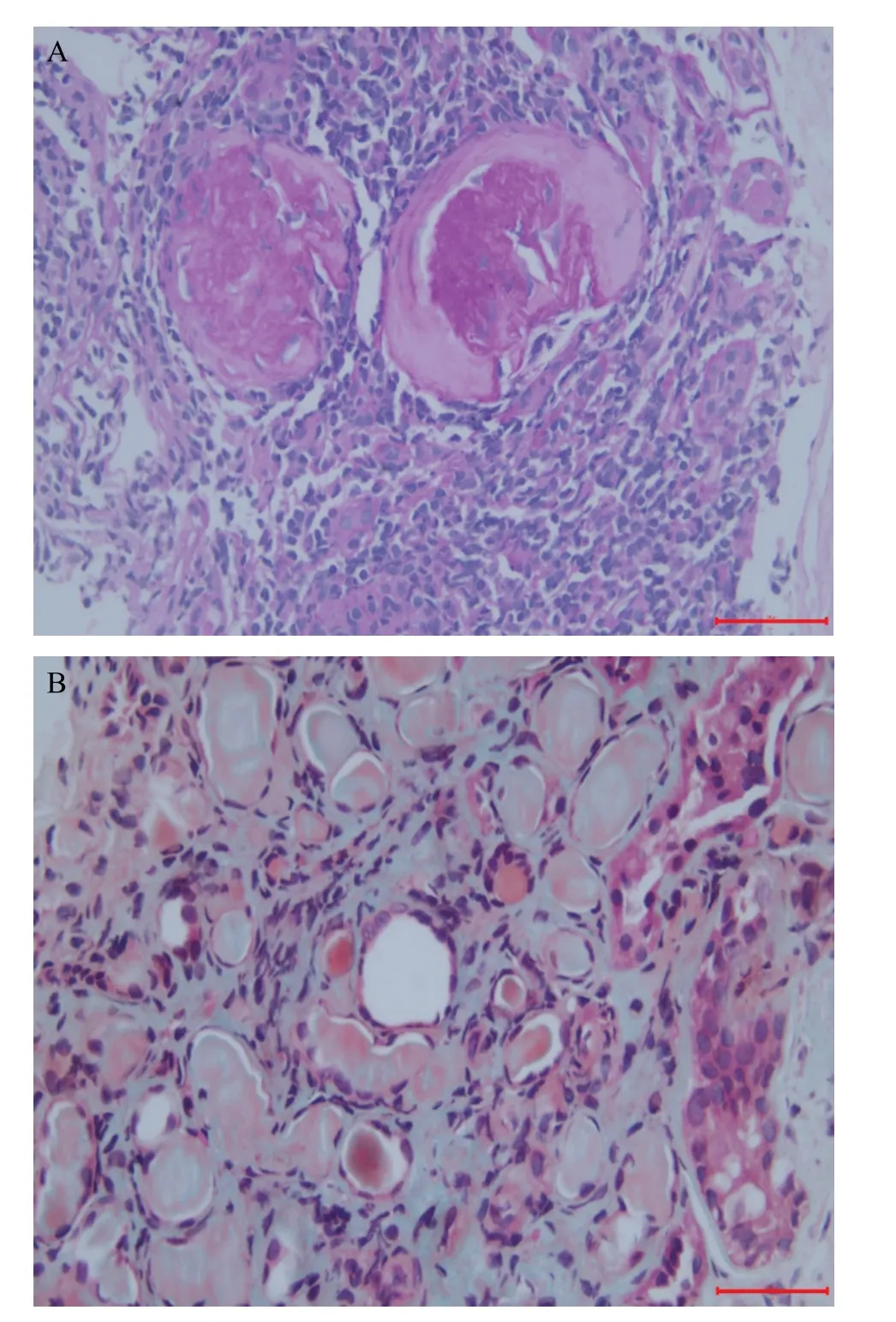
Figure 2. Histological findings secondary to Sj?gren’s syndrome (SS)are typically described as multifocal lymphocytic and plasma cell infiltration in the renal interstitial tissues. A: chronic tubulointerstitial nephritis nephritis (TIN) with glomerulus fibrosis and glomerular capillaries sclerotic; B: acute and chronic TIN with proteinaceous casts and atrophic tubules (magnifications ×200, hematoxylin and eosin stain).
A diagnosis of pSS is often considered based on the classic symptoms of mouth and eyes dryness,fatigue, and pain.The presence of anti-SSA/SSB antibodies strongly supports the diagnosis and should be assessed in all suspected cases of pSS. According to the most recently published 2016 American College of Rheumatology (ACR) / European League Against Rheumatism (EULAR) classification criteria for pSS,we should classify suspected patients as pSS upon at least one positivity for either anti- SSA/SSB antibody or minor salivary gland biopsy (MSGB).Anti-SSA/SSB antibody is presented in 60%-70% of pSS patients.The positivity for anti-SSA/SSB antibody is associated with early disease onset, more severe exocrine glandular dysfunction and extra glandular manifestations, persistent B cell activation and a higher risk of lymphoproliferative disease.On the other hand, we can consider a patient with pSS without anti-SSA/SSB positivity if the patient shows positive findings in histopathology fulfilling the 2016 ACR classification criteria. However, MSGB cannot be easily performed in primary care settings due to its inconvenience and possible complications.
Management of pSS is symptomatic. In the acute setting, when the patient presents with hypokalemia,the priority will be to reverse the severe hypokalemia with intravenous potassium supplementation, followed by correcting the underlying acidosis. Long-term use of potassium supplementation might be required for the majority of the patients. Although no immunomodulatory drug has proved to be efficacious in pSS, a combination of corticosteroids and other immunosuppressive drugs has been reported to slow the progression of renal damage in SS.
CONCLUSIONS
In conclusion, we present a case of pSS though this patient was negative for anti-SSA/SSB antibody.Although SS might have a varying clinical presentation,the presentation of a person with renal symptoms in the form of hypokalemia as the first symptom might create confusion to reach the diagnosis. This case emphasizes the need to consider a wide set of differential diagnoses, including SS, in cases of repeated episodes of unexplained hypokalemia and RTA. Biopsy of minor salivary glands is typically recommended for establishing a diagnosis of pSS in the absence of anti-SSA/SSB antibodies. Diagnosis at an early stage and timely treatment may allow for better control and prevent the progression of the disease.
This work was supported by a research grant from the Medical Science and Technology Projects of Zhejiang Province,China (2018KY421).
The patient was given his informed consent and all procedures performed followed the ethical standards of our hospital.
The authors report no conflicts of interest.
All authors contributed substantially to the writing and revision of this manuscript and approved of its contents.
 World Journal of Emergency Medicine2022年2期
World Journal of Emergency Medicine2022年2期
- World Journal of Emergency Medicine的其它文章
- Comment on “Comparison of different versions of the quick sequential organ failure assessment for predicting in-hospital mortality of sepsis patients”
- An incident of chloroform poisoning on a university campus
- Systemic embolism with left atrial thrombus occurring four years after left atrial appendage closure in a patient with atrial fibrillation
- Born with a luxated globe: An ocular emergency
- Euglycemia despite a sodium glucose co-transporter 2 inhibitor overdose
- Bedside diagnosis of hemoperitoneum by characteristics of fluid visualized on focused assessment with sonography in trauma exam in a patient in non-traumatic shock