
Spousal communication,fertility preference and other factors affecting contraceptive use among married couples in Ekiti State,Nigeria
2022-03-31 08:14:28AustineIdowuIbikunlePaulOladapoAjayiOluwafunmilayoOluwadamilolaIbikunleDemiladeOlusolaIbirongbeAyodeleKamalAlabiKabirAdekunleDurowade
Austine Idowu Ibikunle,Paul Oladapo Ajayi,Oluwafunmilayo Oluwadamilola Ibikunle,Demilade Olusola Ibirongbe,Ayodele Kamal Alabi,5,Kabir Adekunle Durowade,5
1Department of Community Medicine,Federal Teaching Hospital (FETHI),Ido-Ekiti,Nigeria
2Department of Community Medicine,Ekiti State University,Ado Ekiti,Ekiti State,Nigeria
3Department of Public Health,Ekiti State Ministry of Health,Ekiti State,Nigeria
4Department of Community Medicine,University of Medical Sciences (UNIMED),Ondo,Nigeria
5Department of Community Medicine,Afe Babalola University Ado-Ekiti,Ekiti State,Nigeria
ABSTRACT
Objective:To assess and compare the relationship between spousal communication,fertility preference,and other factors with contraceptive use among married couples in Ekiti State,Nigeria.
Methods:This cross-sectional study was carried out in Ado-Ekiti Local Government Area of Ekiti State,Nigeria between the 12th of August 2017 and the 15th of February 2018. A pre-tested,semi-structured interviewer-administered questionnaire was used to collect data from 976 respondents by a multi-stage sampling technique. Data were analyzed (univariate,bivariate,and binary logistic regression analysis) using SPSS version 24.0. Factors that showed statistical significance (P<0.05) were included in a binary logistic regression to determine significant predictors of contraceptive use.
Results:The proportion of respondents currently using contraceptives was 56.9%. The education status of the respondents revealed that those with primary education were more likely to use contraceptives than those without formal education [adjusted odds ratio (aOR) 8.4,95% confidence interval (CI) 1.97-36.2,P<0.001].Respondents with fair spousal communication were more likely to use contraceptive than those with poor communication (aOR 4.9,95% CI 2.80-8.71,P<0.001). In addition,fertility preference of 4 or less children was found to be significantly associated with contraceptive use (aOR 3.0,95% CI 1.67-5.50,P<0.001)compared to a preference of more than 4 children. Finally,the urban respondents were more likely to use contraceptives than those in the rural setting (aOR 1.7,95% CI 1.16-2.41,P=0.047).
Conclusions:Educational status,residential site,spousal communication,and fertility preference significantly influence the level of contraceptive use among married couples. Couples should endeavor to discuss more on issues bordering on their fertility preference and contraceptive issue. Government should formulate policies to improve the rural uptake of contraceptives using identified target interventions.
KEYWORDS:Spousal communication; Contraceptive use;Fertility preference; Factors; Modern contraceptive; Married couples; Ekiti State; Nigeria
Significance
Contraceptive use has been widely accepted globally,especially in the developed countries. However,in developing countries like Nigeria,the use is still low despite improved awareness. The study shows that educational status,spousal communication,residence site,and fertility preference constitute major factors affecting contraceptive use among married couples. Hence,target intervention among married couples using these dentified factors will improve contraceptive usage.
1. Introduction
The importance of spousal communication among married couples cannot be overlooked,as it has been seen to impact family contraceptive use and family stability[1,2]. Ability to regulate fertility among couples requires adequate communication,deliberate actions,and behaviours,including the agreement on the desired number of children. Since marital fertility involves the participation of the wife and husband who may differ in their reproductive goals (in terms of number and sex composition of children,the timing of having the children),successful planning and decision-making about family size and use of contraceptives require effective communication of both marital partners[3,4].
Most contraceptive methods are developed for women,and family planning services are primarily provided to individual women,too,not to couples. Family planning programs for several decades have virtually ignored men[5]. However,it is obvious that husbands play a crucial role in fertility decision-making throughout the world. A Nigerian study on male reproductive intentions found that interspousal communication,as reported by more than 3 000 couples,was significantly associated with having a smaller family size[6].
A high level of awareness about contraception but a very low level of use has been established in some studies in Nigeria[7-9]. Although the unmet need for modern contraceptives was still very high,particularly in sub-Saharan Africa,South Asia,and western Asia[10-12],in Nigeria,the 2013 Nigeria Demographic and Health Survey(NDHS) still found that only 15% of married women of reproductive age use contraceptives[10]. This is lower than the current Sub-Saharan Africa average of 17%. Further analysis of the total contraceptive prevalence rate indicates wide state variations,ranging from 0.6% in Kano to 48.3% in Lagos state and zonal variations ranging from 3.2% in the North East to 38.0% in the South West. According to the 2013 NDHS,Nigerian women have about one child more than the number they want. This implies that the total fertility rate of 5.5 children per woman is 15% higher than it will be if all unwanted births were avoided[10].
Promotion of contraceptive practices has also intensified,yet with 14.1% contraceptive prevalence in Nigeria,it shows low usage of contraceptives (compared to set a target of 60%) among the women[11],which might not be unconnected to couples’ inability to achieve their fertility preference through the barrier of poor or lack of sound communication on the need and choice of contraceptive uptake,necessitating enquiring into factors that could explain the trend among the dwellers of Ado Ekiti Local Government Areas(LGA) where such study has not been carried out before.
This study aims to assess spousal communication,fertility preference,and other factors affecting contraceptive practice among married couples in Ado LGA,Nigeria.
2. Subjects and methods
2.1. Study design and setting
This was a community-based,cross-sectional analytic study of married couples in Ado-Ekiti Local Government Area (LGA) of Ekiti State,Nigeria. This study was conducted between the 12th of August 2017 and the 15th of February 2018. The study was carried out in Ado LGA,which is one of the sixteen LGAs of Ekiti State,South-Western Nigeria. It is the most populous Local Government in Ekiti state with 13 wards,and a population of 308 621 based on the 2006 national census,and an annual growth rate of 3.2% (with a 2016 projected population of 423 215). About 22% of the total population in the LGA[10],which amounted to 93 108,was the population of women of reproductive age in the LGA from which the participants in this study were drawn.
The study population consisted of married females within the reproductive age group (15-49 years) and their spouses,who had been living together for the least six months preceding the time of the study,while couples without a child were excluded.
2.2. Sample size
The minimum sample size for this study was determined by using the formula for comparison of two proportions[13].

Where n is the minimum sample size,U is standard normal deviate corresponding to the power of 80% = 0.84,V is standard normal deviate corresponding to the confidence level of 95% for two-tailed test = 1.96.
Using (P1) the prevalence of contraceptive use among married couples from a previous study in an urban community in Sokoto State[14]and assuming a 10% difference for a comparable rural population,on the basis that contraceptive prevalence rate in a rural community will be lower compared to the urban community (P2),and compensating for 10% non-response[15],a minimum sample size of 244 was derived,which implied that a total of 488 respondents(spouses) in each of urban and rural areas of Ado LGA were recruited for the study,making a total of 976 respondents.
A multi-stage sampling technique was used to select the respondents from the 13 wards in Ado LGA. In stage 1,two wards were selected through a simple random sampling technique by balloting. In stage 2,five settlements were selected from the two wards by simple random sampling technique by balloting method.The list of all the households in each selected settlement was generated to produce a sampling frame in stage 3,while a systematic random sampling method was used to determine households involved in the study.
2.3. Data collection and measurement
A pre-tested,semi-structured interviewer-administered questionnaire adapted from the 2012 National HIV/AIDS and Reproductive Health Survey (NARHS PLUS)[11]and NDHS 2013[10],Nigeria,was used to collect data from the respondents.This was pre-tested in a settlement in Oye LGA,which is about 60 kilometers from Ado-Ekiti,with the reliability of the instrument guaranteed by a test-retest method. The questionnaire contained section A-D:having socio-demographic information of the respondent; contraceptive use among married couples; spousal communication,and fertility preference; factors associated with contraceptive use,respectively.
2.4. Statistical analysis
The data were collected,cleaned,and entered manually,and analyzed (univariate,bivariate,and binary logistic regression analysis) using IBM SPSS version 24.0. Results were presented in mean±standard deviation (mean±SD),number,and percentage.Chi square test was carried out to assess the association between the independent and dependent variables in the bivariate analysis.Factors that showed statistical significance (P<0.05) in bivariate analysis were included into a binary logistic regression to determine the significant predictors of contraceptive use using an adjusted odds ratio (aOR) at 95% confidence interval (CI).
2.5. Ethical consideration
The study was approved by the Ethical Review Committee of the Federal Teaching Hospital,Ido-Ekiti (protocol number:ERC/2017/07/04/64),and written informed consent was obtained from the respondents after the study was explained to the participants. Confidentiality of the respondent’s data was guaranteed during and after the study.
3. Results
3.1. Socio-demographic characteristics of respondents
As shown in Table 1,out of the 976 expected respondents,we had 956 respondents giving a 2% non-response rate. More of the respondents fell between 25-34 years age group,401 (42.0%). The mean age of the respondents was (35.2±6.1) years. The majority of the respondent had their first marriage with the 20-29 years age group,576 (60.2%). The respondents were predominantly Yorubas [652 (68.2%)]and mostly Christians [643 (67.2%)].Most of the respondents had tertiary education,467 (48.9%).
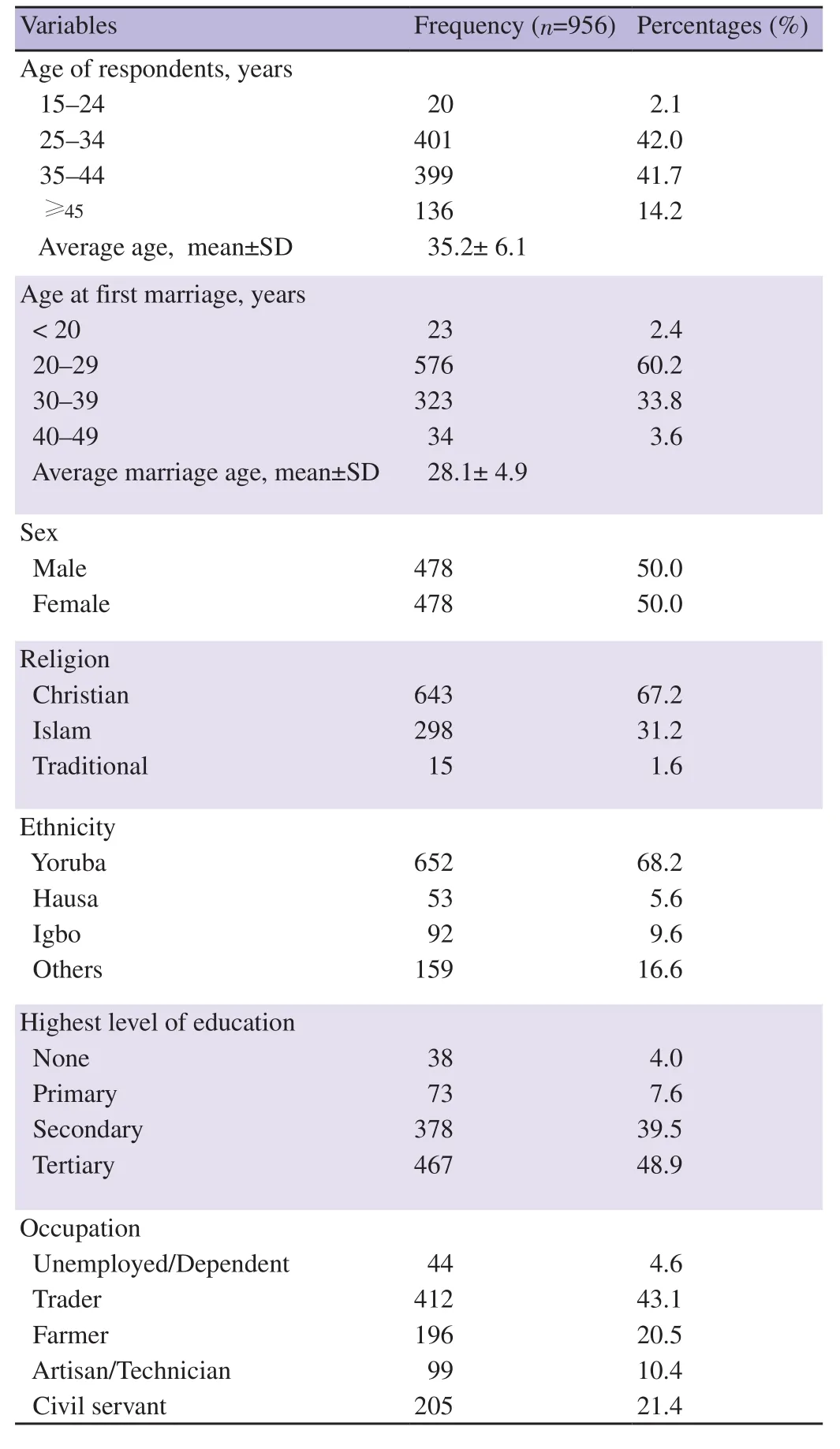
Table 1. Socio-demographic characteristics of respondents.
3.2. Contraceptive use among respondent couples
Most of the respondents had ever used contraceptives,768 (80.3%).Contraceptive pills were the main type of contraception being used in the communities,537 (69.9%). More than half of the respondents currently use contraceptives,544 (56.9%). Among the couples in the communities,many of the respondents said they suggested the use of contraceptives,281 (51.6%) (Table 2).
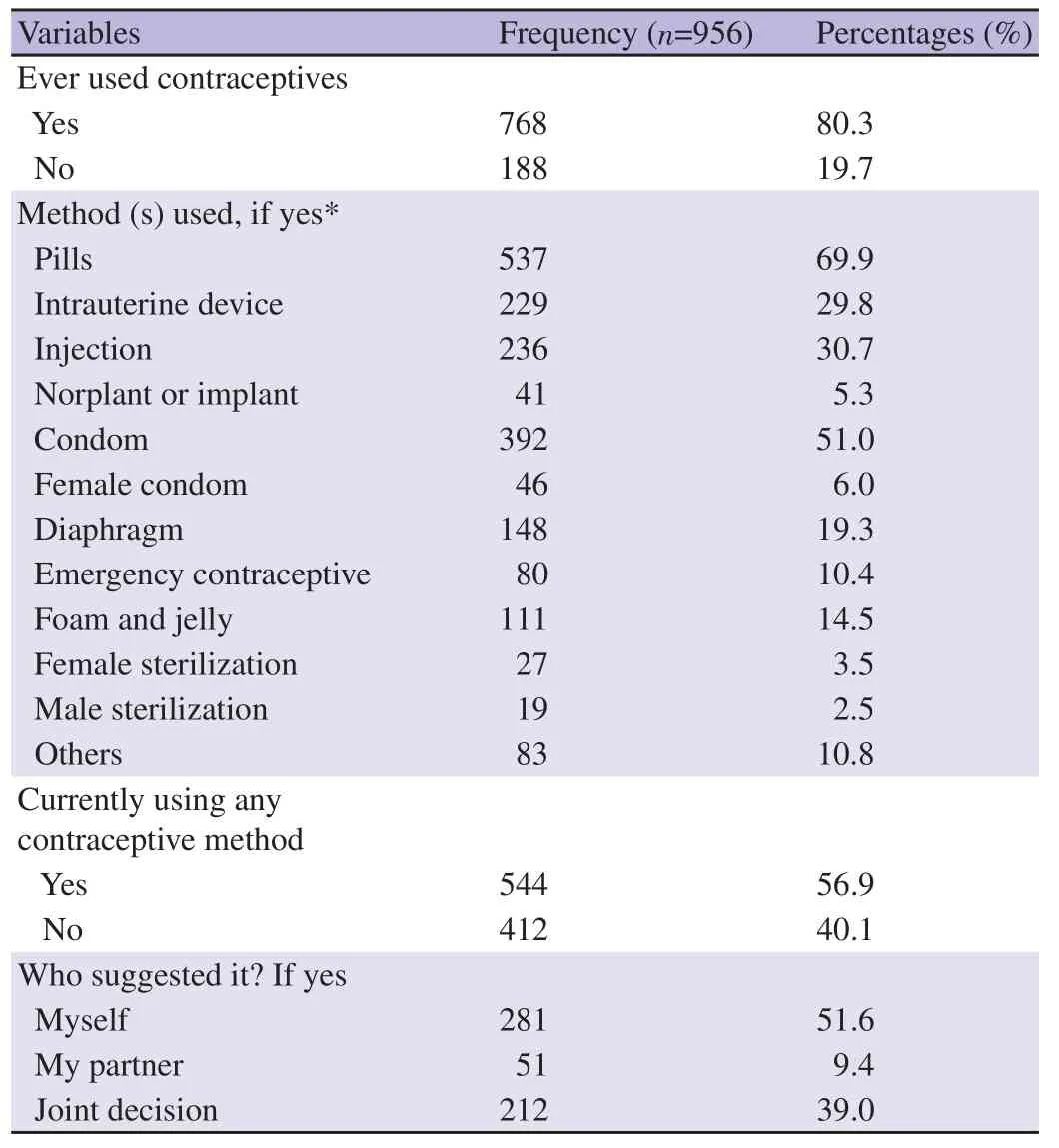
Table 2. Contraceptive use among respondent couples.
3.3. Relationship between socio-demographic characteristics and contraceptive use among respondents in this study
In Table 3,there were significant differences between contraceptive user and nonuser groups in religion (P<0.001),ethnicity (P<0.001),the level of education (P<0.001),residency site (P<0.044),and occupation (P<0.001).
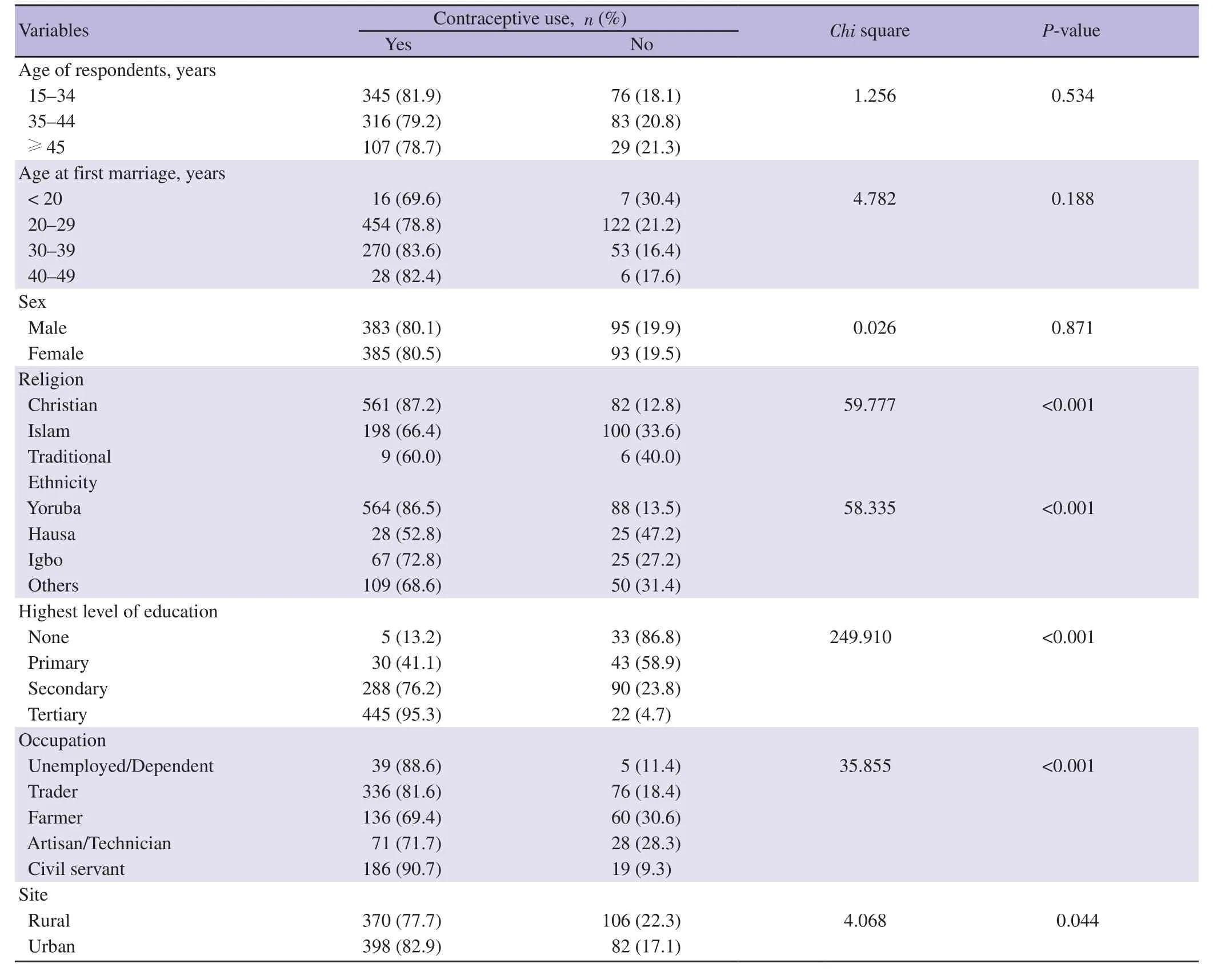
Table 3. Relationship between socio-demographic characteristics and contraceptive use among respondents.
3.4. Relationships between spousal communication,fertility preference,and contraceptive use among respondents in this study
Table 4 reveals there were significant differences between contraceptive users and non-users in their level of spousal communication and fertility preference. The majority (446,97.4%) of the respondents in this study who had good spousal communication were contraceptive users,while the majority (238,87.8%) of those with fair communication were contraceptive users.Equally,the majority (143,63.0%) of those with poor spousal communication were non-users.
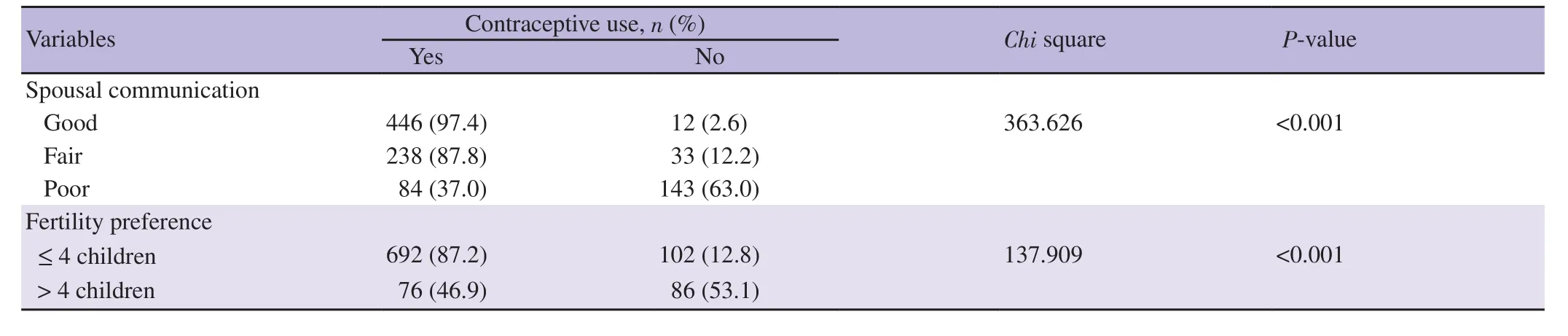
Table 4. Relationships between spousal communication,fertility preference,and contraceptive use among respondents.
Similarly,the majority (692,87.2%) of the respondents who desired ≤ 4 children were found to be contraceptive users,while the majority (86,53.1%) of those who desired > 4 children were non-users.
3.5. A binary logistic regression for the predictors of contraceptive use among respondents in this study
In Table 5,among the respondents in this study,the binary logistic regression revealed that the level of education,spousal communication,residency site and fertility preference were significant predictors of contraceptive use among the respondents.Those with primary education were more likely to use contraceptives than those without formal education (aOR 8.4,95% CI 1.97-36.2,P<0.001). Those with fair spousal communication were more likely to use contraceptives than those with poor spousal communication(aOR 4.9,95% CI 2.80-8.71,P<0.001). On fertility preference,those who desired ≤ 4 children were more likely to use contraceptives than those who desired > 4 children (aOR 3.0,95% CI 1.67-5.50,P<0.001). The urban respondents were more likely to use contraceptives more than those in the rural setting (aOR 1.70,95%CI 1.16-2.41,P=0.047).
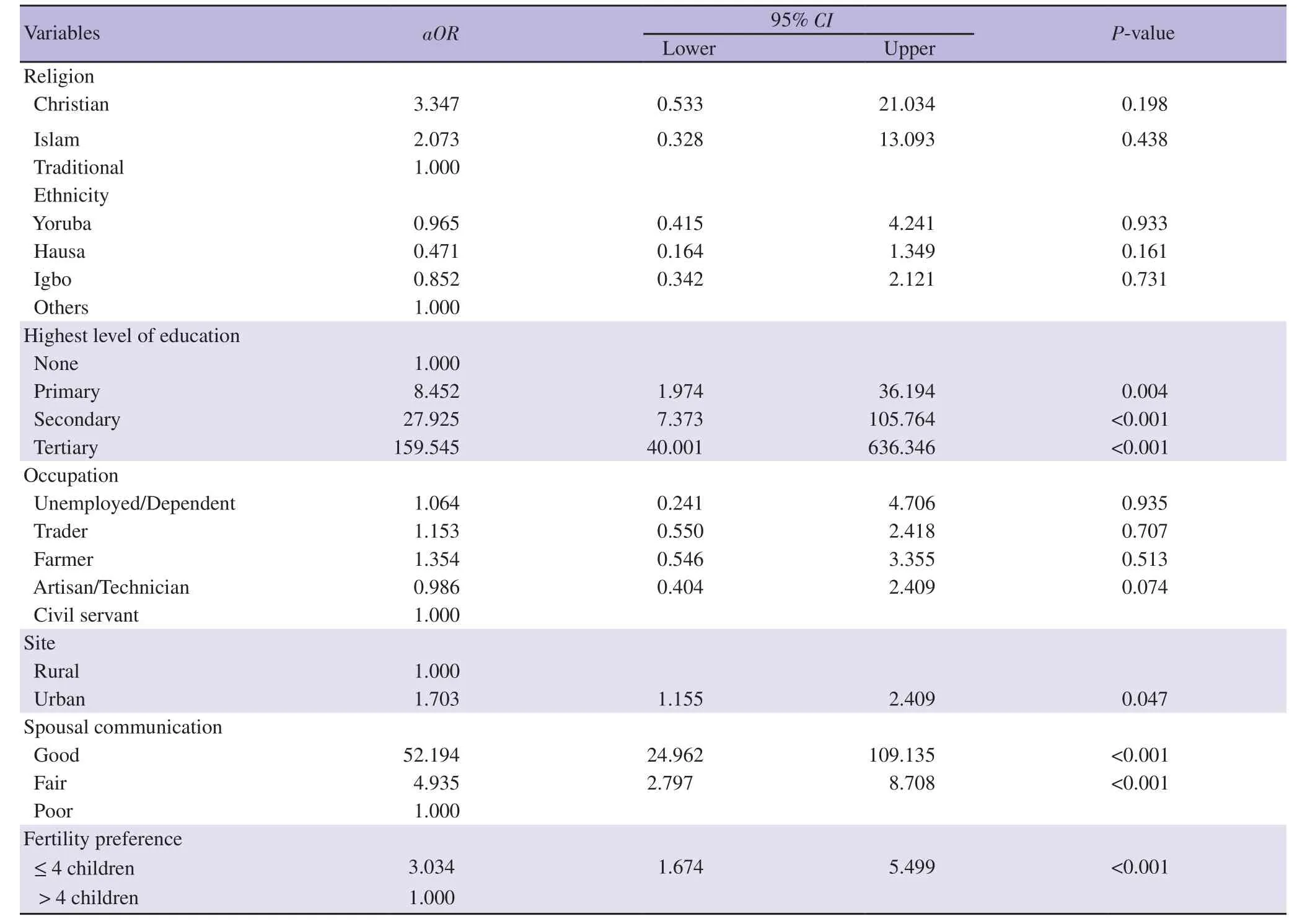
Table 5. A binary logistic regression for the predictors of contraceptive use among respondents.
4. Discussion
This study examines how spousal communication,fertility preference,and other factors affect contraceptive use among married couples in Ekiti State,Nigeria. Respondents’ educational status,residential site of the respondents,spousal communication,and fertility preference were the statistically significant explanatory variables while respondent’s age,gender,age at the first marriage,religion,ethnicity,and occupation had no significant effect on contraceptive use.
In this study,the prevalence rate for the current contraceptive user was 56.9%,with contraceptive pills being the commonest contraceptive method used; the result of this study was quite higher than the (NDHS 2018) national contraceptive rate (17%)[16]. This may have resulted from a high level of education of the respondents and ease of using an oral contraceptive. A study reported that the modern contraceptive prevalence rate was 81.3% in Dhulikhel Municipality,Nepal in which Depo-Provera was the most used(54.5%) contraceptive method[17]. The literacy rate was high,and the sample size was smaller; this may have accounted for the high prevalence.
The educational status of the respondents had a significant effect on contraceptive use (aOR 8.4,95% CI 1.97-36.2,P<0.001). Those with primary education were more likely to use contraceptives than those without formal education. This is similar to Alo,Solanke,and Nyarko’s studies revealed that a higher education status increases the likelihood of contraceptive use[18-20]; education exposes individuals to information and is expected to enlighten the mind and free one of misconceptions and biases towards contraceptives usage.
The level of spousal communication affects contraceptive use among the respondents. Those with fair spousal communication were more likely to use contraceptives (aOR 4.9,95% CI 2.80-8.71,P<0.001). Similarly,spousal communication was found to increase the use of contraceptives in two studies,in Ethiopia and Bangladesh,respectively[21,22]. Also,a study in Nepal revealed 91.6% of women were found to be involved in decision making and had good inter-spousal communication (93.3%) which increase contraceptive use[17]. Communication helps the couple to sort out their differences and harmonize on their fertility preferences,thus improving their usage of contraceptives. The majority of the couples discussed together with the number of children and the preferred sex that they desired to have. And this might have influenced them to have also adequately discussed the need to use contraceptives with their spouses. The high level of spousal communication in this study is expected to influence contraceptive use in the communities.Our finding is similar to that of a study conducted in Ogbomoso and Iseyin on husband-wife communication and couple’s fertility desires among the Yoruba of Nigeria,which showed that 66% of the couples reported joint spousal communication on family planning and 59% on fertility[23].
In this current study,concerning fertility preferences,a significantly higher proportion of the respondents do not want more than 4 children; those who desire less than 4 children were more likely to use contraceptives than those who desire more than 4 children (aOR 3.0,95% CI 1.67-5.50,P<0.001). Fertility preference was found to increase the use of contraceptives in two studies in Ethiopia and Bangladesh,respectively[21,22]. Sex preference may be another reason for fertility preference; the majority preferred to have a boy as their next child. This high level of desire or demand for a male child might not be unconnected to the peculiarity of our environment and cultural values,which rate male children above female ones. As a result,there is the likelihood that couples may not use contraceptives but continue child-bearing until a male child is born[24].
For the respondents who do not communicate with their spouses oncontraception,lack of interest was the main reason for talking about contraceptives. Interventions can be planned towards increasing interest and awareness among such individuals.
The majority of the couples agree together on the number of children. This is similar to a study in which 87% of couples reported similar fertility preferences[8]. Agreement on when to have another child was low and spousal agreement on when to stop having children was lower. This implies that though spouses communicate and agree more on the number of children they want to have,there is less agreement on when to have or stop having them. This could have a negative effect on the current use of contraceptives.Finally,more respondents residing in the urban areas used more contraceptives than their rural counterparts (aOR 1.70,95% CI 1.16-2.41,P=0.047),which is similar to a study by Milkowski et al in the United State[25].
There are some limitations in the study. Reluctance to divulge information concerning couples’ reproductive life was observed,but assurances of confidentiality of data,and keeping identity anonymous reduced this limitation.
In conclusion,spousal communication and joint decisionmaking among married couples in the communities significantly influence the level of contraceptive use,as seen in the majority of the respondents who had good or fair spousal communications.Fertility preference in terms of the number of children desired by the respondents also has a significant effect on contraceptive use,especially those respondents who do not want more than four children tends to use contraceptives more. Other factors that influence contraceptive use include educational status and urban residency. It is therefore recommended that couples should endeavor to discuss more on issues bordering on their fertility preference and contraceptive issue. Lastly,the government should ensure all their citizens (especially in the rural areas) are educated to improve the adoption of healthy behaviours including contraceptive use. Also,the government should formulate policies to improve the uptake of contraceptives using the identified factors.
Conflict of interest statement
The authors declare that they have no competing interests.
Authors' contributions
Austine Idowu Ibikunle,Paul Oladapo Ajayi,Oluwafunmilayo Oluwadamilola Ibikunle,Demilade Olusola Ibirongbe,Ayodele Kamal Alabi,Kabir Adekunle Durowade conceived and designed the study,including study selection,data analysis,and results interpretation. All authors prepared and reviewed the manuscript;read and approved the manuscript.
 Asian Pacific Journal of Reproduction2022年2期
Asian Pacific Journal of Reproduction2022年2期
- Asian Pacific Journal of Reproduction的其它文章
- INRA82 extender enhances semen quality in ram under cooled and cryopreserved stages
- Protective effect of Scrophularia striata combined with trehalose and cysteine added to diluents on cryopreservd goat epididymal sperm
- Profiling of seminal antioxidant indices and sperm quality in Plasmodium bergheiinduced malarial mice treated with Phyllanthus amarus
- An ethnopharmacological survey of medicinal plants used in the traditional treatment of human infertility in eastern Algeria
- Determinants of emergency contraceptive pill use in Bangladesh:An analysis of national survey data
- A scoping review of SARS-CoV-2 and male infertility:Concerns and future prospects