
A young male with abdominal distention and fever after cardiopulmonary resuscitation treatment
2022-09-01 05:20:20GuofengChenKaiboChenJianChen
Guo-feng Chen,Kai-bo Chen,Jian Chen
Department of Gastrointestinal Surgery,the Second Affiliated Hospital of Zhejiang University School of Medicine,Hangzhou 310009,China
Abdominal distention after cardiopulmonary resuscitation (CPR) is a common phenomenon that presents in the emergency department.It is caused by a long period of bag-valve mask ventilation or esophageal intubation.However,a rare but life-threating diagnosis should be considered when distention progresses rapidly.Here,we reported a patient who developed a fever and abdominal pain that couldn’t be relieved by gastric decompression.
CASE
A healthy 33-year-old male had fatigue that lasted for one month,cough and dizziness,and he suddenly developed cardiac arrest and was sent to the emergency department.His body mass index (BMI) was 26.4 kg/m.He had no history of peptic ulcer,mental,infectious or hereditary disease.He never smoked and occasionally had social alcohol drinking.He was diagnosed with acute myocarditis and saved by CPR and defibrillation.A feeding tube was inserted into the duodenum to provide enteral nutrients.However,he developed abdominal distension with a fever of 39.2 ℃ after one week of observation in the intensive care unit (ICU).
On examination,the patient had significant left upper quadrant tenderness and rebound tenderness on palpation.The laboratory examinations showed obvious elevations in the white blood cell count,C-reactive protein,and D-dimer,which were 18.7×10/L,250.0 mg/L,and 13,990 μg/L,respectively.Then,acute abdominal computed tomography(CT) with intravenous contrast was performed,and a small amount of extragastric free air was found (Figure 1).Therefore,the initial diagnosis was gastric perforation of an unknown cause with acute peritonitis.
Since the disease was severe and complicated,a multidisciplinary team discussion was held.Upon rigorous observation of the CT images,the radiologist recognized that there was ischemia within the celiac trunk and the superior mesenteric artery (SMA) (Figures 2 A and B),which was the main cause of the perforation.In addition,emergency exploratory laparotomy was suggested for perforation repair.A perforation in the fundus of the stomach was identified during the operation.Meanwhile,ischemia and necrosis were revealed in the entire stomach,liver,and most segments of the small intestine and colon (Figure 2C),and no arterial pulse was palpable in the hepatic or splenic artery.
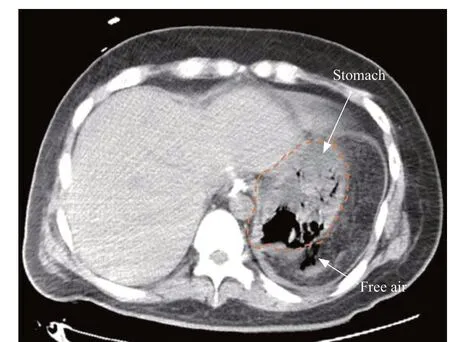
Figure 1. An abdominal computed tomography scan indicated extragastric free air (shown in axial view).
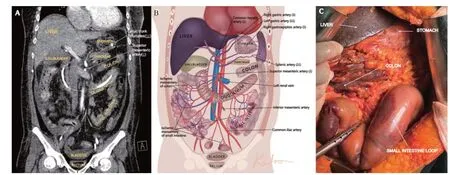
Figure 2. Images of a computed tomography (CT) scan and intraoperative photograph.A: the contrast CT scan showed that there was no enhancement of the splenic artery and insufficient enhancement of the left gastric artery,the common hepatic artery and the superior mesenteric artery (shown in coronal view);B: the illustrative picture simulated different degrees of ischemia (↓: decreased blood flow;↓↓: significantly decreased blood flow);C: in traoperative photograph demonstrated ischemia and necrosis of the entire perforated stomach,liver,and most segments of the small intestine and colon.
His family refused any additional intervention after a detailed intraoperative conversation,and unfortunately,the patient soon died of multiple organ dysfunction syndrome (MODS).
DISCUSSION
Gastric perforation or rupture with pneumoperitoneum was mostly related to massive gastric distension,esophageal intubation,a history of peptic ulcer or other underlying causes and was rarely reported after CPR.Gastric perforation after CPR,if not recognized,is associated with a very high mortality risk.For cases without underlying vascular factors,surgical exploration with primary closure or gastrostomy is indicated for patients with signs of peritonitis,and conservative therapy should be cautiously applied for non-peritonitis patients.
Normally,the stomach is supplied by a rich system of arteries derived from the celiac trunk;thus,it is extremely rare to see entire gastric ischemia.Babu was the first to describe the term “ischemic gastritis”,which referred to acute or chronic mesenteric ischemia with a component of celiac territory ischemia syndrome (CTIS).A previous study documented that perforation of the gastric fundus and splenic infarction could occur after acute occlusion of the celiac trunk or its branches or as a result of ischemia of the celiac artery due to aortic dissection.Another retrospective study concluded that patients with ischemic gastritis would have vomiting,epigastric pain,bleeding or even gastric perforation.This patient developed severe abdominal distention and pain,whereas he had no vomiting or gastrointestinal bleeding.Revascularization of the celiac trunk and SMA via bypass surgery and percutaneous transluminal angioplasty are two alternative treatments for patients with ischemic gastritis.We excluded the possibility of esophageal intubation or improper ventilation as the cause of gastric perforation,and no trauma was seen in the stomach.Although the mechanism of how thromboembolism was formed in the celiac trunk and SMA was unknown,gastric perforation due to CTIS was the most likely explanation based on the CT findings and the intraoperative manifestation of multiorgan ischemia.Emergency physicians should keep this rare complication of CPR in mind.Furthermore,consultations with vascular doctors are necessary to determine the best possible vascular interventions for such cases of ischemia.
CONCLUSIONS
We reported a case of gastric perforation due to CTIS after successful CPR treatment.Clinicians should be aware of this rare complication of CPR when abdominal distention persists with severe pain and fever because an emergency laparotomy and a vascular intervention are needed.
ACKNOWLEDGMENTS
The authors would like to sincerely thank Cong-cong Yu and Jia-ning Chen for their support.
This work was supported by the Basic Public Welfare Research Project of Zhejiang Province (LGF21H030005);the Zhejiang Provincial Key Project of Research and Development Fund (2019C03043).
Ethical approval for this study was obtained from the Medical Ethics Committees of the Second Affiliated Hospital of Zhejiang University School of Medicine (approval number 2022-0075).
The author(s) declare no potential conflicts of interest.
GFC and KBC contributed equally to this study.GFC,KBC,and JC wrote the manuscript,drew the figures,gained ethical approval and revised the manuscript.All the authors have read and approved the final version of the manuscript.
 World Journal of Emergency Medicine2022年5期
World Journal of Emergency Medicine2022年5期
- World Journal of Emergency Medicine的其它文章
- Death related to ethyl chloride inhalation abuse: a case report
- A young man presenting with persistent hypoglycaemia and reduced level of consciousness: case study with review of literature
- Sepsis caused by Eggerthelle lenta: a case report
- Use of veno-arterial extracorporeal membrane oxygenation in the first successful combined lung-liver transplantation patient in China
- Systemic lupus erythematosus in a male teenager manifested with cardiogenic shock and extremities infarction
- Association between cardiovascular implantable electronic devices and tricuspid regurgitation: a casecontrol study