
Augmentation of literature review of COVlD-19 radiology
2022-09-30 02:59:28SulemanAdamMerchantPrakashNadkarniMohdJavedSaifullahShaikh
World Journal of Radiology 2022年9期
TO THE EDlTOR
We compliment Pal
[1] for their excellent review. It is a comprehensive review indeed. An excellent effort with great details, including in depth pathophysiology, detailed illustrations,
Their coverage of imaging modalities is quite extensive too and includes a detailed look into the role of ultrasound in coronavirus disease 2019 (COVID-19), including point-of-care ultrasound, an invaluable addition. For the benefit of your readers, we wish to augment their excellent work and submit the following suggestions for the benefit of your readers.
lNCLUSlON OF ADDlTlONAL RADlOLOGlC FEATURES
We are involved in an ongoing multicentric international study on COVID-19 chest imaging and developing artificial intelligence (AI) algorithms for diagnosis, risk stratification, monitoring, prognostication,
Our 2020 publication has described additional important and distinctive COVID-19 chestimaging features[2]. These include the following, seen on both plain chest radiographs and computed tomography (CT).
The words of Proverbs 11 came to mind: “A good man [person] is guided…and directed by honesty…Be sure you know a person well before you vouch9 for his [or her] credit
Classic signs of pulmonary infarcts
Triangular/wedge shaped opacities with their bases towards the periphery of the lung/lobe/lobule. This sign has sensitivity and specificity of 22% and 82%, respectively[3,4].
Oligemia, a rarefied area due to blood vessel collapse, distal to the site of occlusion by a pulmonary embolus. This sign has sensitivity and specificity of 14% and 92%, respectively[3,5].
I was willing to give him that pleasure, but I was afraid that he wouldn t be able to find the way here by himself, so I made myself ready to go with him
Fuhrman
[61] developed a cascaded transfer learning approach to extract quantitative features from thoracic CT sections using a fine-tuned VGG19 network where a CT-scan-level representation of thoracic characteristics and a support vector machine was trained to distinguish between patients who required steroid administration and those who did not. They demonstrated significant differences between patients who received steroids and those who did not and concluded that their ‘cascade deep learning method’ has great potential in clinical decision-making and for monitoring patient treatment.
SlGNS ASSOClATED WlTH COVlD-19 PNEUMONlA
Subpleural sparing
Reported in 23% of COVID-19 cases in an Iranian study[10], subpleural sparing is commonly associated with nonspecific interstitial pneumonia and is described with lung contusions, pulmonary alveolar proteinosis, severe acute respiratory syndrome (SARS) and
infection[11]. The specificity of this finding depends on the prior probability of COVID-19 based on molecular detection
polymerase chain reaction (PCR).
Then he opened a little window in the roof and let down the chain from which the kettle usually hung, and tried to hook the bed covering and to draw it up
Reversed halo sign
The reversed halo sign is a focal ring-shaped area of ground-glass opacity within a peripheral rim of consolidation, suggesting an organizing/healing pneumonia[12]. It offers prognostic potential in COVID-19[13,14]. Data on sensitivity/specificity are not currently available. Utilizing classic signs of infarcts and pneumonia will increase diagnostic accuracy, and also help raise awareness about chest radiographs’ utility, even in the current era, especially in cost-constrained locales lacking sophisticated infrastructure. It will also help develop more accurate AI algorithms for diagnosis/prognosis of COVID-19. Co-occurrences of these signs are uncommon across COVID-19 patients: When seen in tandem, however, they may constitute a highly specific diagnostic signature. This speculation, of course, needs validation by larger studies.
ADDlTlONAL ANNOTATlON TO lMAGES
The paper’s images[1] show the following (currently unannotated) features: Subpleural sparing, figures 4B just under arrow marked as ground glass opacities, 7C and 7F; Hampton’s humps, figures 2E, 2F, 4B (marked as consolidation), 4C and 7A (larger, but fewer, in the right lung than left lung); Westermark sign, figure 2F; and pericardial air, figure 2C.
AMPLlFlED DlSCUSSlON OF CARDlOVASCULAR EFFECTS FROM COVlD-19
Distribution of cardiovascular angiotensin-converting enzyme 2 receptors and pathophysiology impact
While correctly noting the ability of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of COVID-19, to invade cells by binding with high affinity to angiotensin-converting enzyme 2 and transmembrane protease serine 2 receptors, the authors have not discussed the cardiovascular system, where COVID-19’s impact has been reviewed widely[6,15-17]. The angiotensinconverting enzyme 2 receptor is also expressed in the cardiovascular system in the endothelium of coronary arteries, cardiomyocytes, cardiac fibroblasts, epicardial adipocytes, vascular endothelial and smooth muscle cells[18-20].
A recent report implicates the booster dose of the COVID-19 vaccine for acute myocarditis too[29]. In infants and children with COVID-19 reports of CAAs, including giant CAAs are gathering momentum[23-26], and cardiac MRI/CT can be an invaluable in diagnosing these too. This is particularly important as these aneurysms (and their catastrophic consequences) are potentially regressible with ‘steroid therapy’. In addition these aneurysms would need to be monitored and managed, including for their potential to develop thrombosis[24]. Management includes cardiac support, immunomodulatory agents and anticoagulation[26]. Richardson
[24] stated that in infants rapidly progressing CAAs are noted post COVID-19 infection. They also stated that as opposed to published reports these may be seen even in the absence of hemodynamic instability, ventricular dysfunction, myocardial ischemia or myopericarditis. In view of the risk of progression of cardiac signs and symptoms, Sperotto
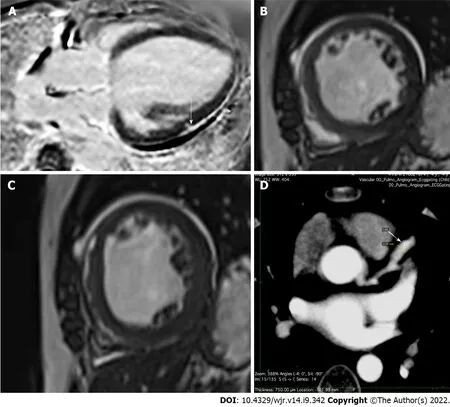
[26] recommended long-term follow-up of these patients. Coronary arteries should therefore be thoroughly assessed in patients presenting with multisystem inflammatory syndrome in children symptoms[25]. For its non-ionizing radiation nature MRI would be the first choice in children. However, CT on account of its speed (and current low radiation protocols) can be utilized effectively too (Figure 1D).
Lukose
[37] stated that the currently popular method of collecting samples using the nasopharyngeal swab and subsequent detection of RNA using real-time PCR has false-positive results and a longer diagnostic time frame. Various optical techniques such as optical sensing, spectroscopy and imaging show great promise in virus detection, and the progress in the field of optical techniques for virus detection unambiguously show great promise in the development of rapid photonics-based devices for COVID-19 detection. They also provided a comprehensive review of the various photonics technologies employed for virus detection, especially the SARS-CoV family, such as near-infrared spectroscopy, fourier transform infrared spectroscopy, raman spectroscopy, fluorescence-based techniques, super-resolution microscopy and surface plasmon resonance-based detection.
ROLE OF CARDlAC AND THORAClC MAGNETlC RESONANCE lMAGlNG
While the authors correctly note that cardiac magnetic resonance imaging (MRI) may be useful in the future to detect complications in patients with abnormal echocardiography, this is a current need too. Up to 60% of hospitalized COVID-19 patients have been reported to have evidence of myocardial injury[21] (Figure 1A). Among post-discharge patients, approximately 10% complain of palpitations, with half of these having ongoing chest pain 6 mo after discharge[15]. Dilated cardiomyopathy is a known complication of COVID-19 cardiac injury[27] (Figures 1B and C). In post-COVID-vaccination patients, distinct self-limited myocarditis and pericarditis have appeared. While myocarditis developed rapidly in younger patients, mostly after the second vaccination, pericarditis affected older patients later, after either the first or second dose[28].
Binding of SARS-CoV-2 to the endothelium predisposes to microthrombosis
endothelial inflammation, complement activation, thrombin generation, platelet and leukocyte recruitment and initiation of innate and adaptive immune responses with complications such as deep vein thrombosis, pulmonary embolism, cortical venous thrombosis, stroke, cardiac inflammation and injury, arrhythmias, blood clots[18] and acute/chronic myocardial injury[21]. An assay of the fibrin degradation product D-dimer (a thrombosis marker) on admission for prognostication of in-hospital mortality is now mandated in most clinical protocols to differentiate mild from severe COVID-19[7,22], especially when coupled with thrombocytopenia[8]. In infants and children reports of coronary artery aneurysms (CAA), including giant CAAs are gathering momentum as a part of multisystem inflammatory syndrome in post COVID-19 children[23-26].
In their Radiology 2021 editorial, Lima
[30] stated that prolonged symptoms due to “l(fā)ong-haul” COVID-19 portend the potential for chronic cardiac sequelae, whose duration and severity remain unknown. They introduced the work of Kravchenko
[31], which demonstrated the value of cardiac MRI in identifying inflammation, adverse patterns of hypertrophy, fibrosis and myocardial injury due to myocarditis, pericarditis, cardiomyopathy and healing.
An enlarged right pulmonary artery, suggesting embolism of segmental/subsegmental pulmonary arteries when seen together with Westermark sign. Sensitivity is reported to be “l(fā)ow” and specificity unknown. These findings are likely due to the microvascular thrombosis propensity in COVID-19[6-8], as discussed below, leading to a relatively increased incidence of pulmonary thromboembolism in COVID-19 pneumonia patients[9].
Lauren Hodge: If you were going to a restaurant and wanted a healthier option, which would you choose, grilled or fried chicken? Now most people would answer grilled, and it's true that grilled chicken does contain less fat and fewer calories. However, grilled chicken poses a hidden danger. The hidden danger is heterocyclic amines -- specifically phenomethylimidazopyridine, or PhIP -- (laughter) which is the immunogenic or carcinogenic compound.
Although thoracic CT is widely used for imaging of COVID-19 infection, thoracic MRI can also be used as an alternative diagnostic tool because of its advantages[32]. This is particularly important in patients requiring avoidance of exposure to ionizing radiation,
in children and during pregnancy where pulmonary MRI may be preferred over pulmonary CT[33]. Pulmonary abnormalities caused by COVID-19 pneumonia can be detected on True FISP MRI sequences and correspond to the patterns known from CT. Spiro
[34] made a useful suggestion for the current pandemic: Following MRI of the abdomen or heart, there should be careful evaluation of the visualized parts of the lungs for COVID-19 findings. This would enable the identification and isolation of undetected cases of COVID-19.
Necker
[35] reported a cinematic rendering of SARS-CoV-2 pneumonia. Cinematic rendering is a digital three-dimensional visualization technique that converts grayscale slices from CT or MRI into colored three-dimensional volumes
transfer functions illuminating the reconstruction with physical light simulation. They have stated that this type of rendering produces a natural, photorealistic image that is intuitively understandable and can be well applied for clinical purposes. Cinematic rendering of CT images is a new way to show the three dimensionality of the various densities contained in volumetric CT/MRI data. We agree with them and feel that such cinematic rendering can make complicated volume rendered CT/MRI images easy to understand for other clinicians, administrators, policy makers as well as patients alike.
Realizing that he had let away someone so important in his life, he decided to call her immediately. His whole mind was flooded with fear. He was afraid that she might have found someone new or no longer had the same feelings anymore... For once, he felt the fear of losing someone.
ROLE OF 18-FLUORODEOXYGLUCOSE POSlTRON EMlSSlON TOMOGRAPHY
The authors’ suggestion of using fluorodeoxyglucose-positron emission tomography (PET) in the future for prognosis and monitoring is wonderful. We wish to add that the “rim sign”, a slight and continuous fluorodeoxyglucose uptake at the border of a peripheral lung consolidation[36], is easily recognizable on fluorodeoxyglucose PET/CT (though data on sensitivity/specificity are not available). When present, it strongly suggests pulmonary infarction and is observable even without suggestive finding of pulmonary infarction. The reverse halo sign would also be seen. Though highly sensitive, use of PET/CT for primary detection of COVID-19 is constrained by poor specificity as well as considerations of cost, radiation burden and prolonged exposure times for imaging staff. However, in patients who may require nuclear medicine studies for other clinical indications, PET imaging may yield the earliest detection of nascent infection in otherwise asymptomatic individuals. This may be extremely vital for immunocompromised patients, including those with coexistent malignancies, where the early diagnosis of infection and subsequent initiation of care needed will contribute vitally to improving outcomes and reducing morbidity and mortality[33].
Role of optical thermal imaging and other remote patient monitoring devices
They hadhastened to bring forth1 flowers before they got green leaves, and inthe yard all the ducklings walked up and down, and the cat too: itbasked in the sun and licked the sunshine from its own paws
Gomez-Gonzalez
[38] reported a proof of concept of optical imaging spectroscopy for rapid, primary screening of SARS-CoV-2. A study by Shah
[39] found that home pulse oximetry monitoring identified the need for hospitalization in initially non-severe COVID-19 patients when a cutoff SpO
of 92% was used and that home SpO
monitoring also reduced unnecessary emergency department revisits. McKay
[40] stated that due to its portability, affordability and potential to serve as a screening tool for a conventionally lab-based invasive test, the mobile phone capillaroscope could serve as an important point-of-care tool and that the simplicity and portability of their technique may enable the development of an effective non-invasive tool for white blood cell screening in point-of-care and global health settings. This would be extremely useful in the COVID-19 pandemic scenario as white blood cell monitoring forms an essential part of COVID-19 management and follow-up[41,42].
Infrared thermography has been considered a gold standard method for screening febrile individuals during pandemics since the SARS outbreak in 2003. Khaksari
[43] showed that in addition to an elevated body temperature a patient with COVID-19 will exhibit changes in other parameters such as oxygenation of tissues and cardiovascular and respiratory system functions. They also promulgated a compelling need to develop a new technique that would have the ability to screen all these signals and utilize the same for early detection of viral infections. In their opinion, keeping the advent of wireless technologies in mind, the development of such sensors that have point-of-care home-accessible capabilities will go a long way in better managing the increasing numbers of patients with COVID-19 who are opting for home quarantine and that this will eventually reduce the burden on the healthcare system.
The COVID-19 pandemic is changing the landscape of healthcare delivery worldwide. There is a discernible shift toward remote patient monitoring. It is pertinent to note that a large number of remote patient monitoring platforms are already utilizing optical technologies[44]. This area of research has great potential for growth, and the biomedical optics community has great prospects in the development, testing and commodification of new wearable remote patient monitoring technologies to add to the available healthcare armamentarium and contribute to the rapidly changing healthcare and research environment, not just for the COVID-19 era but far beyond[44].
Various other ingenious methods/modalities have been used for early detection/screening for COVID-19. These include smartwatches[45], smart phones and other intelligent edge devices. Mishra
[45] developed a method utilizing data from smartwatches to detect the onset of COVID-19 infection in real-time that detected 67% of infection cases at or before symptom onset. They stated that their study provided a roadmap to a rapid and universal diagnostic method for the large-scale detection of respiratory viral infections in advance of symptoms, highlighting a useful approach for managing epidemics using digital tracking and health monitoring. Seshadri
[46] stated that when used in conjunction with predictive platforms, wearable device users could receive alerts when changes in their metrics match those related to COVID-19 and that such anonymous data localized to regions such as neighborhoods or zip codes could provide public health officials and researchers a valuable tool to track and mitigate the spread of the virus. Their manuscript describes clinically relevant physiological metrics that can be measured from commercial devices today and highlights their role in tracking the health, stability, and recovery of COVID-19 + individuals and front-line workers.
Cho
[60] performed quantitative CT analysis on chest CT images using supervised machine learning to measure regional ground glass opacities and inspiratory and expiratory image matching to measure regional air trapping in survivors of COVID-19. They summarized that quantitative analysis of expiratory chest CT images demonstrated that small airway disease with the presence of air trapping is a long-lasting sequelae of SARS-CoV-2 infection.
AI in COVID-19 imaging. Telemedicine has advanced by leaps and bounds. AI algorithms enable faster diagnosis (including remote diagnosis), with a fair degree of accuracy[48]. While the application of AI to medical imaging of cancers and other diseases is being developed over the past decades, the recent COVID-19 pandemic hastened the: (1) Need; (2) Development; (3) Training; and (4) Testing of AI algorithms, within a relatively shorter time-span of less than 2 years[49]. This was extremely beneficial for radiologists and other physicians involved in performing rapid diagnosis, keeping in mind this was a time when there was immense overloading of the healthcare system[50]. The benefits including for management were obvious. However limitations such as: (1) Limited datasets; (2) Inaccurate execution of training and testing procedures; and (3) Use of incorrect performance criteria needed to be dealt with. The above limitations can be overcome by the utilization of federated learning[48,51,52].
The technique of federated learning was originally pioneered by Google[53] as an application of their well-known MapReduce algorithm[54] and allows for iteratively training a machine learning model across geographically separated hardware, including mobile devices. The machine learning algorithm is distributed, while data remains local. It can be employed for both statistical and deep learning. Despite its drawbacks, specifically wide-area network bandwidth limits computation speed, federated learning appears to be a great way forward, especially for multicenter collaborations, getting around the ‘tricky’ data privacy issue and enabling algorithms/outcomes with much more accuracy than otherwise possible[51].
If AI is to make an even greater impact, Merchant
[48] suggested getting down to the basics and incorporating time tested key medical ‘teaching’ and/or key ‘clinical’ parameters, including prognostic indicators, for more effective AI algorithms and their better clinical utility. They also stated that “Artificial Intelligence needs real Intelligence to guide it!”. Combining the wisdom gained over the years with the immense versatility of AI algorithms will maximize the accuracy and utility of AI applications in medical diagnosis and treatment modalities. We have gained wisdom regarding COVID-19 imaging over the past few years and should utilize the same for creation of better algorithms for screening/detection/prognostication and management.
El Naqa
[55], as part of a Medical Imaging Data and Resource Center initiative, noted that the pandemic has led to the coupling of interdisciplinary experts that include: (1) Clinicians; (2) Medical physicists; (3) Imaging scientists; (4) Computer scientists; and (5) Informatics experts, all of whom are working towards solving the challenges of the COVID-19 pandemic, specifically AI methods applied to medical imaging. They stated that the lessons learned during the transitioning to AI in the medical imaging of COVID-19 can inform and enhance future AI applications, making the entire transition more than every discipline combined to respond to emergencies like the COVID-19 pandemic. AI has been used in multiple imaging fields for COVID-19 imaging.
The model by Manokaran
[56] could achieve an accuracy of 94.00% in detecting COVID-19 and an overall accuracy of 92.19%, which was based on DenseNet-201. The model can achieve an area under receiver operating characteristic curve of 0.99 for COVID-19, 0.97 for normal and 0.97 for pneumonia. Their automated diagnostic model yielded an accuracy of 94.00% in the initial screening of COVID-19 patients and an overall accuracy of 92.19% using chest X-ray images.
Kusakunniran
[57] proposed a solution to automatically classify COVID-19 cases in chest X-ray images using the ResNet-101 architecture, which was adopted as the main network with over 44 million parameters. A heatmap was constructed under the region of interest of the lung segment to visualize and emphasize signals of COVID-19. Their method achieved a sensitivity, specificity and accuracy of 97%, 98% and 98%, respectively. Rao
[58] stated that separable SVRNet and separable SVDNet models greatly reduced the number of parameters while improving the accuracy and increasing the operating speed.
Yi
[50] utilized a large CT database (1112 patients) provided by the China Consortium of Chest CT Image Investigation and investigated multiple solutions in detecting COVID-19 and distinguishing it from other common pneumonia and normal controls. They compared the performance of different models for complete and segmented CT slices, in particular studying the effects of CT-superimposition depths into volumes, on the performance of their models and showed that an optimal model could identify COVID-19 slices with 99.76% accuracy (99.96% recall, 99.35% precision and 99.65% F1-score).
Chaddad
[59] investigated the potential of deep transfer learning to predict COVID-19 infection using chest CT and X-ray images. They opined that combining chest CT and X-ray images with DarkNet architecture achieved the highest accuracy of 99.09% and area under receiver operating characteristic curve of 99.89% in classifying COVID-19 from non-COVID-19 and that their results confirmed the ability of deep convolutional neural networks with transfer learning to predict COVID-19 in both chest CT and X-ray images. They concluded that this approach could help radiologists improve the accuracy of their diagnosis and improve overall efficiency of COVID-19 management.
Schuller
[47] in their paper tilted ‘COVID-19 and Computer Audition: An Overview on What Speech & Sound Analysis Could Contribute in the SARS-CoV-2 Corona Crisis’ provided an overview on the potential for computer audition,
the usage of speech and sound analysis by AI, to help in the COVID-19 pandemic scenario and concluded that computer audition appears ready for implementation of (pre-)diagnosis and monitoring tools and more generally provides rich and significant, yet so far untapped, potential in the fight against COVID-19 spread.
It is time to revisit these time-tested radiological signs for pulmonary infarcts[2]. Utilizing classic signs of infarcts and pneumonia will increase diagnostic accuracy and help raise awareness about the utility of chest radiographs, even in the current era; especially in cost-constrained locales lacking sophisticated infrastructure. It will also help develop more accurate AI algorithms for diagnosis/prognosis of COVID-19. Co-occurrences of these signs are uncommon across COVID-19 patients: When seen in tandem, however, they may constitute a highly specific diagnostic signature. This speculation, of course, needs validation by larger studies.
THE FUTURE
Quantum computers and quantum microscopes, new quantum repeaters enabling a scalable super secure quantum internet (distance will no longer be a hindrance, not just internet of things but ‘intelligent edge’ devices commonplace[62]) will give a quantum boost to COVID-19 and other health care algorithms/strategies, including in other related fields, improving healthcare in ways beyond the realm of dreams[51]. Cloud computing could be complemented by edge computing, taking advantage of the burgeoning intelligent edge devices (smartphones are commonplace in the remotest of locations). Besides latency, edge computing is preferred over cloud computing in remote locations, where there is limited or no connectivity to a centralized location (a requirement of cloud computing), which requires local storage, similar to a mini data center at their location[63]. Medical imaging including COVID-19/other pandemic imaging and AI will never be the same again, in the era of quantum computing and quantum AI imaging and health care will reach stratospheric levels and beyond[47].
Was Cocoa aware of just what he was doing? I’ll never really know. What I do know is that I’m glad I made a promise to spend my golden years with this wonderful chocolate brown poodle -- for Cocoa not only shares his life with me, he has made sure that I will be around to share my life with him!
Correction of “pulmonary destruction”. The author’s state: “The migration of fluid into the alveolar sacs is governed by the imbalance in Starling forces. The diffuse alveolar damage caused by the viral particles results in an increased capillary wall permeability (high
value), thereby increasing the force at which fluid migrates from the capillaries to the alveolar space.” emphasis added. Surely the authors mean “rate” instead of “force”. Permeability is the inverse of resistance. By analogy with Ohm’s Law for electricity (current = voltage/resistance) or its equivalent for blood pressure (cardiac output = blood pressure/peripheral resistance), capillary outflow will increase under fixed/constant pressure if permeability increases.
The old woman, who guessed his thoughts, laughed kindly7 and said, I ll tell you what you must do, for I ve taken a fancy to you, and I m sure you won t forget me when you ve made your fortune
We hope that this augmentation of the excellent review by Pal
[1] will enhance your readers’ ability to evaluate COVID-19 patients on imaging. COVID-19 is here to stay. Each effort at adding to the information available in the literature will go a long way in improving patient care overall.
FOOTNOTES
All authors contributed equally.
All the authors report no relevant conflicts of interest for this article.
You know that, not content with endowing Celandine, Princess of the Summer Islands, with everything she could desire to make her charming, I actually took the trouble to bring her up myself; and now what does she do but come to me with more coaxings and caresses13 than usual to beg a favour
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
India
Oh! you wicked child, 39 cried the Witch. What is this I hear? I thought I had hidden you safely from the whole world,40 and in spite of it you have managed to deceive me. 41
One day, when he was in the wood gathering4 sticks and crying bitterly, a little old woman came up to him and asked him what was the matter; and he told her all his troubles
Suleman Adam Merchant 0000-0001-6513-450X; Prakash Nadkarni 0000-0002-9628-4700; Mohd Javed Saifullah Shaikh 0000-0002-5615-4813.
Wang JJ
The girl watched Gaston on the plate, and she actually didn t like him. He was all ugh, as he had been in the first place. He didn t have a home anymore and he was wandering around on the white plate and he was silly and wrong and ridiculous and useless and all sorts of other things. She cried a little, but only inside, because long ago she had decided17 she didn t like crying because if you ever started to cry it seemed as if there was so much to cry about you almost couldn t stop, and she didn t like that at all. The open halves of the peach seed were wrong, too. They were ugly or something. They weren t clean.
Filipodia
Wang JJ
1 Pal A, Ali A, Young TR, Oostenbrink J, Prabhakar A, Deacon N, Arnold A, Eltayeb A, Yap C, Young DM, Tang A,Lakshmanan S, Lim YY, Pokarowski M, Kakodkar P. Comprehensive literature review on the radiographic findings,imaging modalities, and the role of radiology in the COVID-19 pandemic.
2021; 13: 258-282 [PMID:34630913 DOI: 10.4329/wjr.v13.i9.258]
2 Merchant SA, Ansari SMS, Merchant N. Additional Chest Imaging Signs That Have the Potential of Being COVID-19 Imaging Markers.
2020; 215: W57-W58 [PMID: 32762540 DOI: 10.2214/AJR.20.24170]
3 Worsley DF, Alavi A, Aronchick JM, Chen JT, Greenspan RH, Ravin CE. Chest radiographic findings in patients with acute pulmonary embolism: observations from the PIOPED Study.
1993; 189: 133-136 [PMID: 8372182 DOI:10.1148/radiology.189.1.8372182]
4 Han D, Lee KS, Franquet T, Müller NL, Kim TS, Kim H, Kwon OJ, Byun HS. Thrombotic and nonthrombotic pulmonary arterial embolism: spectrum of imaging findings.
2003; 23: 1521-1539 [PMID: 14615562 DOI:10.1148/rg.1103035043]
5 Stein PD, Beemath A, Matta F, Weg JG, Yusen RD, Hales CA, Hull RD, Leeper KV Jr, Sostman HD, Tapson VF, Buckley JD, Gottschalk A, Goodman LR, Wakefied TW, Woodard PK. Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II.
2007; 120: 871-879 [PMID: 17904458 DOI: 10.1016/j.amjmed.2007.03.024]
6 Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review.
2020; 5: 831-840 [PMID: 32219363 DOI: 10.1001/jamacardio.2020.1286]
7 Zhang L, Yan X, Fan Q, Liu H, Liu X, Liu Z, Zhang Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19.
2020; 18: 1324-1329 [PMID: 32306492 DOI: 10.1111/jth.14859]
8 McFadyen JD, Stevens H, Peter K. The Emerging Threat of (Micro)Thrombosis in COVID-19 and Its Therapeutic Implications.
2020; 127: 571-587 [PMID: 32586214 DOI: 10.1161/CIRCRESAHA.120.317447]
9 Léonard-Lorant I, Delabranche X, Séverac F, Helms J, Pauzet C, Collange O, Schneider F, Labani A, Bilbault P, Molière S, Leyendecker P, Roy C, Ohana M. Acute Pulmonary Embolism in Patients with COVID-19 at CT Angiography and Relationship to d-Dimer Levels.
2020; 296: E189-E191 [PMID: 32324102 DOI: 10.1148/radiol.2020201561]
10 Tabatabaei SMH, Talari H, Moghaddas F, Rajebi H. CT Features and Short-term Prognosis of COVID-19 Pneumonia: A Single-Center Study from Kashan, Iran.
2020; 2: e200130 [PMID: 33778569 DOI:10.1148/ryct.2020200130]
11 Chong WH, Saha BK, Austin A, Chopra A. The Significance of Subpleural Sparing in CT Chest: A State-of-the-Art Review.
2021; 361: 427-435 [PMID: 33487401 DOI: 10.1016/j.amjms.2021.01.008]
12 Maturu VN, Agarwal R. Reversed halo sign: a systematic review.
2014; 59: 1440-1449 [PMID: 24782557 DOI: 10.4187/respcare.03020]
13 Sales AR, Casagrande EM, Hochhegger B, Zanetti G, Marchiori E. The Reversed Halo Sign and COVID-19: Possible Histopathological Mechanisms Related to the Appearance of This Imaging Finding.
2021; 57: 73-75[PMID: 34629671 DOI: 10.1016/j.arbres.2020.06.029]
14 Marchiori E, Nobre LF, Hochhegger B, Zanetti G. CT characteristics of COVID-19: reversed halo sign or target sign?
2021; 27: 306-307 [PMID: 33290240 DOI: 10.5152/dir.2020.20734]
15 Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, Kang L, Guo L, Liu M, Zhou X, Luo J, Huang Z, Tu S, Zhao Y, Chen L,Xu D, Li Y, Li C, Peng L, Xie W, Cui D, Shang L, Fan G, Xu J, Wang G, Zhong J, Wang C, Wang J, Zhang D, Cao B. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study.
2021; 397: 220-232 [PMID:33428867 DOI: 10.1016/S0140-6736(20)32656-8]
16 Hamming I, Timens W, Bulthuis ML, Lely AT, Navis G, van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis.
2004; 203: 631-637 [PMID:15141377 DOI: 10.1002/path.1570]
17 Zheng YY, Ma YT, Zhang JY, Xie X. COVID-19 and the cardiovascular system.
2020; 17: 259-260[PMID: 32139904 DOI: 10.1038/s41569-020-0360-5]
18 Salamanna F, Maglio M, Landini MP, Fini M. Body Localization of ACE-2: On the Trail of the Keyhole of SARS-CoV-2.
2020; 7: 594495 [PMID: 33344479 DOI: 10.3389/fmed.2020.594495]
19 Gheblawi M, Wang K, Viveiros A, Nguyen Q, Zhong JC, Turner AJ, Raizada MK, Grant MB, Oudit GY. Response by Gheblawi
to Letter Regarding Article, "Angiotensin-Converting Enzyme 2: SARS-CoV-2 Receptor and Regulator of the Renin-Angiotensin System: Celebrating the 20th Anniversary of the Discovery of ACE2".
2020; 127: e46-e47[PMID: 32614719 DOI: 10.1161/CIRCRESAHA.120.317332]
20 Patel VB, Zhong JC, Grant MB, Oudit GY. Role of the ACE2/Angiotensin 1-7 Axis of the Renin-Angiotensin System in Heart Failure.
2016; 118: 1313-1326 [PMID: 27081112 DOI: 10.1161/CIRCRESAHA.116.307708]
21 Giustino G, Croft LB, Stefanini GG, Bragato R, Silbiger JJ, Vicenzi M, Danilov T, Kukar N, Shaban N, Kini A, Camaj A,Bienstock SW, Rashed ER, Rahman K, Oates CP, Buckley S, Elbaum LS, Arkonac D, Fiter R, Singh R, Li E, Razuk V,Robinson SE, Miller M, Bier B, Donghi V, Pisaniello M, Mantovani R, Pinto G, Rota I, Baggio S, Chiarito M, Fazzari F,Cusmano I, Curzi M, Ro R, Malick W, Kamran M, Kohli-Seth R, Bassily-Marcus AM, Neibart E, Serrao G, Perk G,Mancini D, Reddy VY, Pinney SP, Dangas G, Blasi F, Sharma SK, Mehran R, Condorelli G, Stone GW, Fuster V, Lerakis S, Goldman ME. Characterization of Myocardial Injury in Patients With COVID-19.
2020; 76: 2043-2055 [PMID: 33121710 DOI: 10.1016/j.jacc.2020.08.069]
22 Velavan TP, Meyer CG. Mild versus severe COVID-19: Laboratory markers.
2020; 95: 304-307 [PMID:32344011 DOI: 10.1016/j.ijid.2020.04.061]
23 Navaeifar MR, Shahbaznejad L, Sadeghi Lotfabadi A, Rezai MS. COVID-19-Associated Multisystem Inflammatory Syndrome Complicated with Giant Coronary Artery Aneurysm.
2021; 2021: 8836403 [PMID: 33505752 DOI: 10.1155/2021/8836403]
24 Richardson KL, Jain A, Evans J, Uzun O. Giant coronary artery aneurysm as a feature of coronavirus-related inflammatory syndrome.
2021; 14 [PMID: 34210694 DOI: 10.1136/bcr-2020-238740]
25 Pick JM, Wang S, Wagner-Lees S, Badran S, Szmuszkovicz JR, Wong P, Votava-Smith J. Abstract 17092: Coronary Artery Aneurysms Are More Common in Post-COVID-19 Multisystem Inflammatory Syndrome in Children (MIS-C) Than Pre-Pandemic Kawasaki Disease.
2020; 142: A17092 [DOI: 10.1161/circ.142.suppl_3.17092]
26 Sperotto F, Friedman KG, Son MBF, VanderPluym CJ, Newburger JW, Dionne A. Cardiac manifestations in SARS-CoV-2-associated multisystem inflammatory syndrome in children: a comprehensive review and proposed clinical approach.
2021; 180: 307-322 [PMID: 32803422 DOI: 10.1007/s00431-020-03766-6]
27 Omidi F, Hajikhani B, Kazemi SN, Tajbakhsh A, Riazi S, Mirsaeidi M, Ansari A, Ghanbari Boroujeni M, Khalili F,Hadadi S, Nasiri MJ. COVID-19 and Cardiomyopathy: A Systematic Review.
2021; 8: 695206[PMID: 34222385 DOI: 10.3389/fcvm.2021.695206]
28 Diaz GA, Parsons GT, Gering SK, Meier AR, Hutchinson IV, Robicsek A. Myocarditis and Pericarditis After Vaccination for COVID-19.
2021; 326: 1210-1212 [PMID: 34347001 DOI: 10.1001/jama.2021.13443]
29 Sanchez Tijmes F, Zamorano A, Thavendiranathan P, Hanneman K. Imaging of Myocarditis Following mRNA COVID-19 Booster Vaccination.
2022; 4: e220019 [PMID: 35506135 DOI: 10.1148/ryct.220019]
30 Lima JAC, Bluemke DA. Myocardial Scar in COVID-19: Innocent Marker versus Harbinger of Clinical Disease.
2021; 301: E434-E435 [PMID: 34374597 DOI: 10.1148/radiol.2021211710]
31 Kravchenko D, Isaak A, Zimmer S, Mesropyan N, Reinert M, Faron A, Pieper CC, Heine A, Velten M, Nattermann J,Kuetting D, Duerr GD, Attenberger UI, Luetkens JA. Cardiac MRI in Patients with Prolonged Cardiorespiratory Symptoms after Mild to Moderate COVID-19.
2021; 301: E419-E425 [PMID: 34374593 DOI: 10.1148/radiol.2021211162]
32 Ates OF, Taydas O, Dheir H. Thorax Magnetic Resonance Imaging Findings in Patients with Coronavirus Disease(COVID-19).
2020; 27: 1373-1378 [PMID: 32830031 DOI: 10.1016/j.acra.2020.08.009]
33 Fields BKK, Demirjian NL, Dadgar H, Gholamrezanezhad A. Imaging of COVID-19: CT, MRI, and PET.
2021; 51: 312-320 [PMID: 33288215 DOI: 10.1053/j.semnuclmed.2020.11.003]
34 Spiro JE, Curta A, Mansournia S, Marschner CA, Maurus S, Weckbach LT, Hedderich DM, Dinkel J. Appearance of COVID-19 pneumonia on 1.5 T TrueFISP MRI.
2021; 54: 211-218 [PMID: 34393286 DOI:10.1590/0100-3984.2021.0028]
35 Necker FN, Scholz M. Chest CT Cinematic Rendering of SARS-CoV-2 Pneumonia.
2022; 303: 501 [PMID:34935512 DOI: 10.1148/radiol.212902]
36 Soussan M, Rust E, Pop G, Morère JF, Brillet PY, Eder V. The rim sign: FDG-PET/CT pattern of pulmonary infarction.
2012; 3: 629-633 [PMID: 22903456 DOI: 10.1007/s13244-012-0189-5]
37 Lukose J, Chidangil S, George SD. Optical technologies for the detection of viruses like COVID-19: Progress and prospects.
2021; 178: 113004 [PMID: 33497877 DOI: 10.1016/j.bios.2021.113004]
38 Gomez-Gonzalez E, Barriga-Rivera A, Fernandez-Mu?oz B, Navas-Garcia JM, Fernandez-Lizaranzu I, Munoz-Gonzalez FJ, Parrilla-Giraldez R, Requena-Lancharro D, Gil-Gamboa P, Rosell-Valle C, Gomez-Gonzalez C, Mayorga-Buiza MJ,Martin-Lopez M, Mu?oz O, Gomez-Martin JC, Relimpio-Lopez MI, Aceituno-Castro J, Perales-Esteve MA, Puppo-Moreno A, Garcia-Cozar FJ, Olvera-Collantes L, Gomez-Diaz R, de Los Santos-Trigo S, Huguet-Carrasco M, Rey M,Gomez E, Sanchez-Pernaute R, Padillo-Ruiz J, Marquez-Rivas J. Optical imaging spectroscopy for rapid, primary screening of SARS-CoV-2: a proof of concept.
2022; 12: 2356 [PMID: 35181702 DOI:10.1038/s41598-022-06393-3]
39 Shah S, Majmudar K, Stein A, Gupta N, Suppes S, Karamanis M, Capannari J, Sethi S, Patte C. Novel Use of Home Pulse Oximetry Monitoring in COVID-19 Patients Discharged From the Emergency Department Identifies Need for Hospitalization.
2020; 27: 681-692 [PMID: 32779828 DOI: 10.1111/acem.14053]
40 McKay GN, Mohan N, Butterworth I, Bourquard A, Sánchez-Ferro á, Castro-González C, Durr NJ. Visualization of blood cell contrast in nailfold capillaries with high-speed reverse lens mobile phone microscopy.
2020; 11:2268-2276 [PMID: 32341882 DOI: 10.1364/BOE.382376]
41 Pirsalehi A, Salari S, Baghestani A, Sanadgol G, Shirini D, Baerz MM, Abdi S, Akbari ME, Bashash D. Differential alteration trend of white blood cells (WBCs) and monocytes count in severe and non-severe COVID-19 patients within a 7-day follow-up.
2021; 13: 8-16 [PMID: 33889357 DOI: 10.18502/ijm.v13i1.5486]
42 Leulseged TW, Hassen IS, Ayele BT, Tsegay YG, Abebe DS, Edo MG, Maru EH, Zewde WC, Naylor LK, Semane DF,Dresse MT, Tezera BB. Laboratory biomarkers of COVID-19 disease severity and outcome: Findings from a developing country.
2021; 16: e0246087 [PMID: 33720944 DOI: 10.1371/journal.pone.0246087]
43 Khaksari K, Nguyen T, Hill B, Quang T, Perreault J, Gorti V, Malpani R, Blick E, González Cano T, Shadgan B,Gandjbakhche AH. Review of the efficacy of infrared thermography for screening infectious diseases with applications to COVID-19.
2021; 8: 010901 [PMID: 33786335 DOI: 10.1117/1.JMI.8.S1.010901]
44 Roblyer D. Perspective on the increasing role of optical wearables and remote patient monitoring in the COVID-19 era and beyond.
2020; 25 [PMID: 33089674 DOI: 10.1117/1.JBO.25.10.102703]
45 Mishra T, Wang M, Metwally AA, Bogu GK, Brooks AW, Bahmani A, Alavi A, Celli A, Higgs E, Dagan-Rosenfeld O,Fay B, Kirkpatrick S, Kellogg R, Gibson M, Wang T, Rolnik B, Ganz AB, Li X, Snyder MP. Early Detection Of COVID-19 Using A Smartwatch. 2020 Preprint. Available from: medRxiv: 2020.07.06.20147512 [DOI:10.1101/2020.07.06.20147512]
46 Seshadri DR, Davies EV, Harlow ER, Hsu JJ, Knighton SC, Walker TA, Voos JE, Drummond CK. Wearable Sensors for COVID-19: A Call to Action to Harness Our Digital Infrastructure for Remote Patient Monitoring and Virtual Assessments.
2020; 2: 8 [PMID: 34713021 DOI: 10.3389/fdgth.2020.00008]
47 Schuller BW, Schuller DM, Qian K, Liu J, Zheng H, Li X. COVID-19 and Computer Audition: An Overview on What Speech & Sound Analysis Could Contribute in the SARS-CoV-2 Corona Crisis.
2021; 3: 564906[PMID: 34713079 DOI: 10.3389/fdgth.2021.564906]
48 Merchant SA, Shaikh MJS, Nadkarni P. Tuberculosis conundrum - current and future scenarios: A proposed comprehensive approach combining laboratory, imaging, and computing advances.
2022; 14: 114-136[DOI: 10.4329/wjr.v14.i6.114]
49 Giger M. Medical imaging of COVID-19.
2021; 8: 010101 [PMID: 34754885 DOI:10.1117/1.JMI.8.S1.010101]
50 Li Y, Pei X, Guo Y. 3D CNN classification model for accurate diagnosis of coronavirus disease 2019 using computed tomography images.
2021; 8: 017502 [PMID: 34322573 DOI: 10.1117/1.JMI.8.S1.017502]
51 Nadkarni P, Merchant SA. Enhancing medical-imaging artificial intelligence through holistic use of time-tested key imaging and clinical parameters: Future insights.
2022; 3: 55-69 [DOI: 10.35711/aimi.v3.i3.55]
52 Rieke N, Hancox J, Li W, Milletarì F, Roth HR, Albarqouni S, Bakas S, Galtier MN, Landman BA, Maier-Hein K,Ourselin S, Sheller M, Summers RM, Trask A, Xu D, Baust M, Cardoso MJ. The future of digital health with federated learning.
2020; 3: 119 [PMID: 33015372 DOI: 10.1038/s41746-020-00323-1]
53 McMahan B, Ramage D. Federated Learning: Collaborative Machine Learning without Centralized Training Data.Google AI Blog. 6 Apr 2017. [cited 14 November 2021]. Available from: https://starrymind.tistory.com/180
54 Dean J, Ghemawat S. MapReduce: Simplified Data Processing on Large Clusters.
2008; 51: 107-113 [DOI:10.1145/1327452.1327492]
55 El Naqa I, Li H, Fuhrman J, Hu Q, Gorre N, Chen W, Giger ML. Lessons learned in transitioning to AI in the medical imaging of COVID-19.
2021; 8: 010902-010902 [PMID: 34646912 DOI:10.1117/1.JMI.8.S1.010902]
56 Manokaran J, Zabihollahy F, Hamilton-Wright A, Ukwatta E. Detection of COVID-19 from chest x-ray images using transfer learning.
2021; 8: 017503 [PMID: 34435075 DOI: 10.1117/1.JMI.8.S1.017503]
57 Kusakunniran W, Karnjanapreechakorn S, Siriapisith T, Borwarnginn P, Sutassananon K, Tongdee T, Saiviroonporn P.COVID-19 detection and heatmap generation in chest x-ray images.
2021; 8: 014001 [PMID:33457446 DOI: 10.1117/1.JMI.8.S1.014001]
58 Rao K, Xie K, Hu Z, Guo X, Wen C, He J. COVID-19 detection method based on SVRNet and SVDNet in lung x-rays.
2021; 8: 017504 [PMID: 34471647 DOI: 10.1117/1.JMI.8.S1.017504]
59 Chaddad A, Hassan L, Desrosiers C. Deep CNN models for predicting COVID-19 in CT and x-ray images.
2021; 8: 014502 [PMID: 33912622 DOI: 10.1117/1.JMI.8.S1.014502]
60 Cho JL, Villacreses R, Nagpal P, Guo J, Pezzulo AA, Thurman AL, Hamzeh NY, Blount RJ, Fortis S, Hoffman EA,Zabner J, Comellas AP. Quantitative Chest CT Assessment of Small Airways Disease in Post-Acute SARS-CoV-2 Infection.
2022; 304: 185-192 [PMID: 35289657 DOI: 10.1148/radiol.212170]
61 Fuhrman JD, Chen J, Dong Z, Lure FYM, Luo Z, Giger ML. Cascaded deep transfer learning on thoracic CT in COVID-19 patients treated with steroids.
2021; 8: 014501 [PMID: 33415179 DOI:10.1117/1.JMI.8.S1.014501]
62 TechCrunch BS. The future is not the Internet of Things… it is the Connected Intelligent Edge. Dec 21, 2021. [cited 22 December 2021]. Available from: https://www.nastel.com/the-future-is-not-the-internet-of-things-it-is-the-connectedintelligent-edge/
63 Arora S. Edge Computing Vs. Cloud Computing: What are the Differences. Jun 30, 2022. [cited 8 March 2022].Available from: https://www.simplilearn.com/edge-computing-vs-cloud-computing-article
 World Journal of Radiology2022年9期
World Journal of Radiology2022年9期
- World Journal of Radiology的其它文章
- Contrast-enhanced multidetector computed tomography features and histogram analysis can differentiate ameloblastomas from central giant cell granulomas
- Reliability of ultrasound ovarian-adnexal reporting and data system amongst less experienced readers before and after training