
Risk of Developing Non-Alcoholic Fatty Liver Disease Over Time in a Cohort of the Elderly in Qingdao,China*
2023-09-16 09:18:46LIULiSHAOYuHanFENGEnQiangSHAOZhuGangandXINGDongMing
LIU Li ,SHAO Yu Han ,FENG En Qiang ,SHAO Zhu Gang ,and XING Dong Ming
Nonalcoholic fatty liver disease (NAFLD) is characterized by fat accumulation in the liver in the absence of alcohol consumption and comprises a variety of conditions such as simple steatosis,nonalcoholic steatohepatitis,fibrosis,and cirrhosis[1].More than one-quarter of the world’s population experience NAFLD[2]. The prevalence of NAFLD in China increased from 23.8% in 2001 to 32.9% in 2018,indicating that hepatitis B virus is the primary cause of chronic liver disease[3].However,NAFLD is considered one of the most important etiologies of chronic liver diseases.The current annual medical and social costs of NAFLD are estimated to be $103 billion in the United States and €35 billion in the European countries. Therefore,it is critical to explore the etiology of NAFLD to prevent its morbidity.
Age,smoking status,physical activity,obesity,hypertension,diabetes,dyslipidemia,and high alanine aminotransferase (ALT) levels are reportedly associated with NAFLD[4-7]. However,these conclusions remain controversial[8-10].Moreover,no study has investigated the longitudinal relationship between changes in risk factors and the progression of NAFLD in the older adults in China.Therefore,our study aims to clarify the impact of certain factors on the development of NAFLD over time,based on a large Chinese elderly cohort study conducted in Qingdao,China.
Based on the National Basic Public Health Service(BPHS) project,two health examinations for residents aged ≥ 65 years were conducted in 2018 and 2021 in five community centers in Qingdao,Shandong Province,China.All Chinese citizens can use the BPHS project’s services in community health centers.The BPHS includes 12 service categories,one of which is the health management of the elderly,which in 2018 and 2021 included: (1) a standard questionnaire including questions about age,sex,marital status,smoking status,alcohol consumption,education,and dietary habits;(2) measurement of height,weight,and blood pressure;and (3) detection of the levels of fasting plasma glucose (FPG),ALT,total cholesterol (TC),triglycerides (TG),high-density lipoprotein cholesterol (HDL),and performing ultrasonography of the liver.ALT and TG levels were determined using enzymatic techniques,and HDL was measured using a direct method.FPG levels were determined using the glucose oxidase method. A written informed consent was obtained from all participants.This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the Qingdao Municipal Center for Disease Control and Prevention.
A total of 57,808 individuals aged ≥ 65 years participated in the health examination in 2018,and 47,862 individuals underwent a health check-up in 2021. Of the 47,862 participants,those with incomplete information on height,weight,and ultrasonography of the liver (n=6,282),as well as those with ALT levels higher than three times of the upper limit (n=236) were excluded.An additional 3,101 participants were excluded because of high alcohol consumption (>140 g/week for men and>70 g/week for women),the presence of hepatitis B surface antigen,a history of schistosomiasis,viral hepatitis,hepatic cirrhosis,liver carcinoma,and autoimmune liver disease. Finally,the data from 38,243 individuals were included in this study.
A balanced diet was defined as consuming adequate types of food with an appropriate ratio of vegetable-to-meat intake.Overweight was defined as body mass index (BMI) ≥ 24.0 kg/m2,and obesity was defined as BMI ≥ 28.0 kg/m2.Hypertension was defined as systolic blood pressure of ≥ 140 mmHg and (or) diastolic blood pressure of ≥ 90 mmHg.Moreover,dyslipidemia was defined as presence of at least one of the following: TC levels of ≥ 5.72 mmol/L,TG levels of ≥ 1.70 mmol/L,HDL levels of<0.91 mmol/L,or lipoprotein cholesterol (LDL) levels of >3.64 mmol/L.Diabetes was defined as an FPG level of ≥ 7.0 mmol/L or a history of previously diagnosed diabetes.
NAFLD was diagnosed using established ultrasound criteria for fatty liver (at least two of the following abnormal findings: increased echogenicity of the liver relative to that of the kidney and spleen,obliteration of the vascular architecture of the liver,and deep attenuation of the ultrasonic signal),safe alcohol consumption (Asian standards: <140 g/week for males and <70 g/week for females),and the absence of HbsAg and anti-HCV.Abnormal ALT levels were defined as levels of >40 IU/L according to the conventional value.
Statistical analyses were performed using SPSS(version 17.0; SPSS,Chicago,IL),and statistical significance was set at a two-sidedP-value of <0.05.Data are presented as mean ± standard deviation for continuous variables and asn(%) for categorical variables. The normality of the variables was examined using the Kolmogorov-Smirnov test.Group differences were compared using the Student’sttest for continuous variables since data were normally distributed.For categorical variables,we used theχ2test to compare differences.Moreover,multivariate logistic regression models were used to calculate the unadjusted and adjusted odds ratios(ORs) and 95% confidence intervals (CIs) for crosssectional associations. Longitudinal analyses were conducted on 19,919 participants without NAFLD in 2018,and multinomial logistic regression models were used to examine the association between changes in possible risk factors and NAFLD over time.Supplementary Table S1 (available in www.besjournal.com) displayed different groups defined by variable status over time.
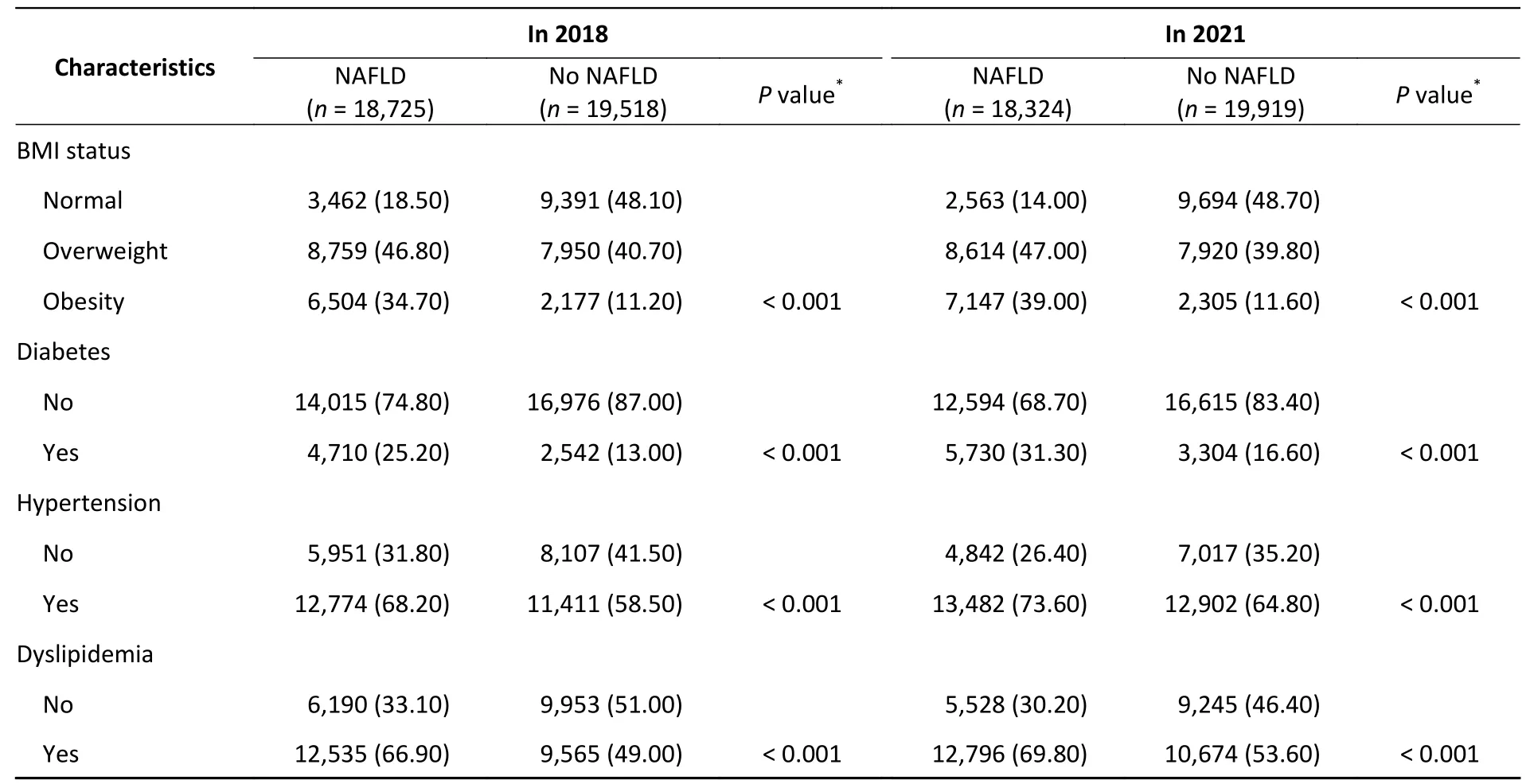
Of the 38,243 individuals aged ≥ 65 years,the prevalence of NAFLD in 2018 and 2021 was 48.96% and 47.91%,respectively (Table 1).The mean values of BMI,TC,TG,LDL,and ALT and the prevalence of hypertension,diabetes,and dyslipidaemia were notably high,while the HDL levels were lower in the participants with NAFLD than that of the participants without NAFLD (P<0.001).
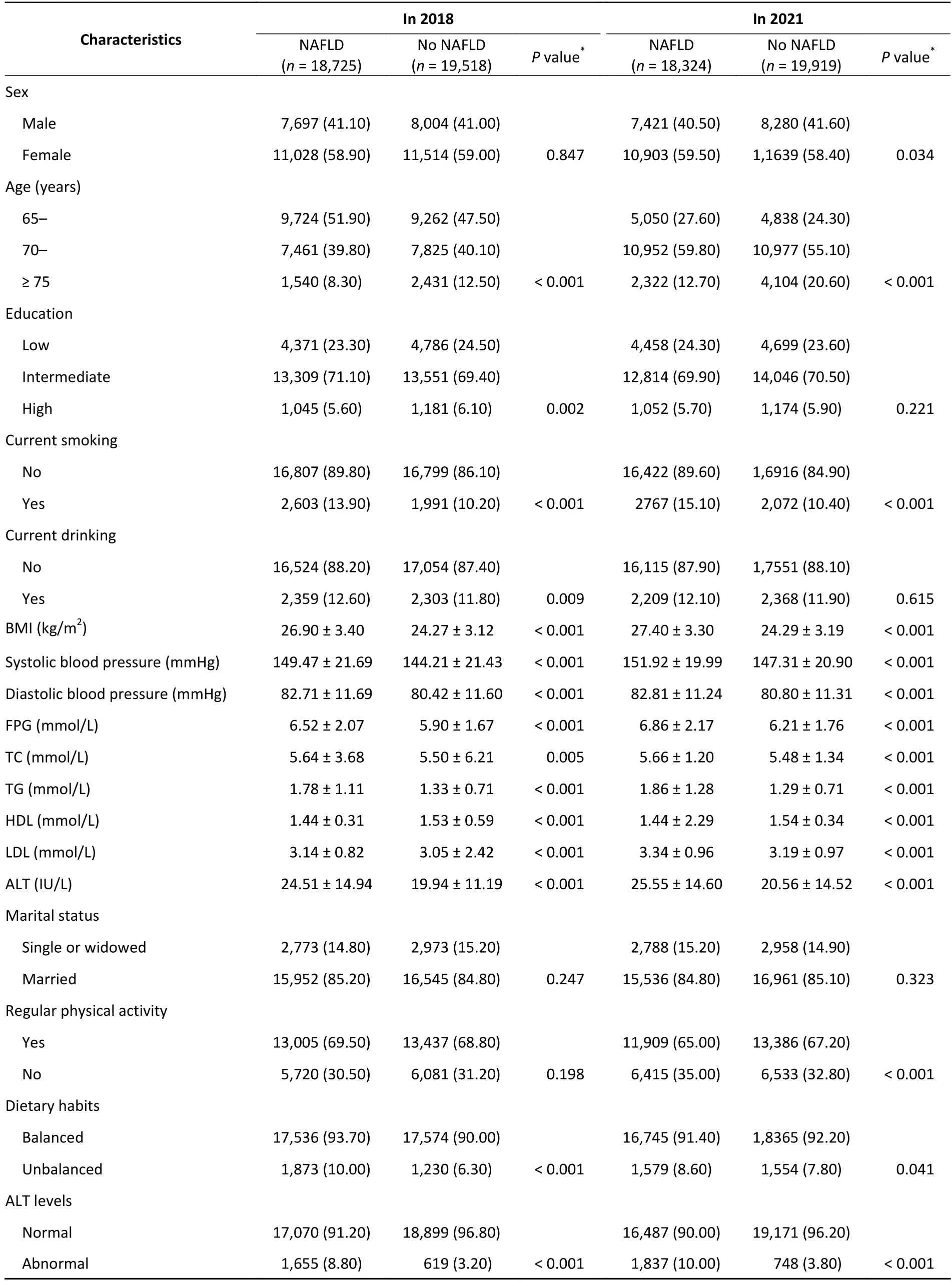
Table 1. Demographic characteristics of the individuals in 2018 and 2021 (in our study)
Continued
In the cross-sectional analysis,current drinking(OR: 1.19,95%CI: 1.11-1.29) and non-balanced dietary habits (OR: 1.63,95%CI: 1.50-1.77)increased the risk of NAFLD,and older age (P<0.001) was negatively associated with NAFLD in the adjusted model in 2018.Compared with those with normal weight,individuals with obesity had a 6.98 fold higher odds (95%CI: 6.54-7.44) and a 10.34 fold higher odds (95%CI: 9.68-11.05) of developing NAFLD in 2018 and 2021,respectively. After adjusting for confounders,abnormal ALT levels,obesity,hypertension,diabetes,and dyslipidemia were all risk factors (P<0.001 for all comparisons)for NAFLD (Table 2).

Table 2. A cross-sectional analysis of relative risk factors for NAFLD in 2018 and 2021
As shown in Table 3,among the elderly without NAFLD in 2018,19.90% had developed NAFLD in 3 years (Table 3).In the longitudinal analyses,current drinking [relative risk reduction (RRR): 1.20,95%CI:1.05-1.38] and unbalanced dietary habits (RRR: 1.45,95%CI: 1.28-1.64) were positively correlated with developing NAFLD,while regular physical activity(RRR: 0.73,95%CI: 0.66-0.81) was negatively associated with NAFLD after adjusting for the confounders. Individuals who remained with overweight or obesity were at an increased risk of developing NAFLD,as the category with the greatest risk for NAFLD was weight gain,which resulted in a change in the BMI status (RRR: 7.99,P<0.001).Remained hypertension (RRR: 1.70,P< 0.001),remained diabetes (RRR: 3.87,P<0.001),remained dyslipidemia (RRR: 1.14,P< 0.05),developed hypertension (RRR: 1.90,95%CI: 1.70-2.12),developed diabetes (RRR: 4.14,95%CI: 3.78-4.54),and developed dyslipidemia (RRR: 1.46,95%CI:1.30-1.63) could increase the incidence of NAFLD,while no longer having hypertension or dyslipidemia could minimize the risks of developing NAFLD.No significant association between ALT levels change and NAFLD was detected,as compared to those with normal ALT levels from 2018 to 2021 (P>0.05).
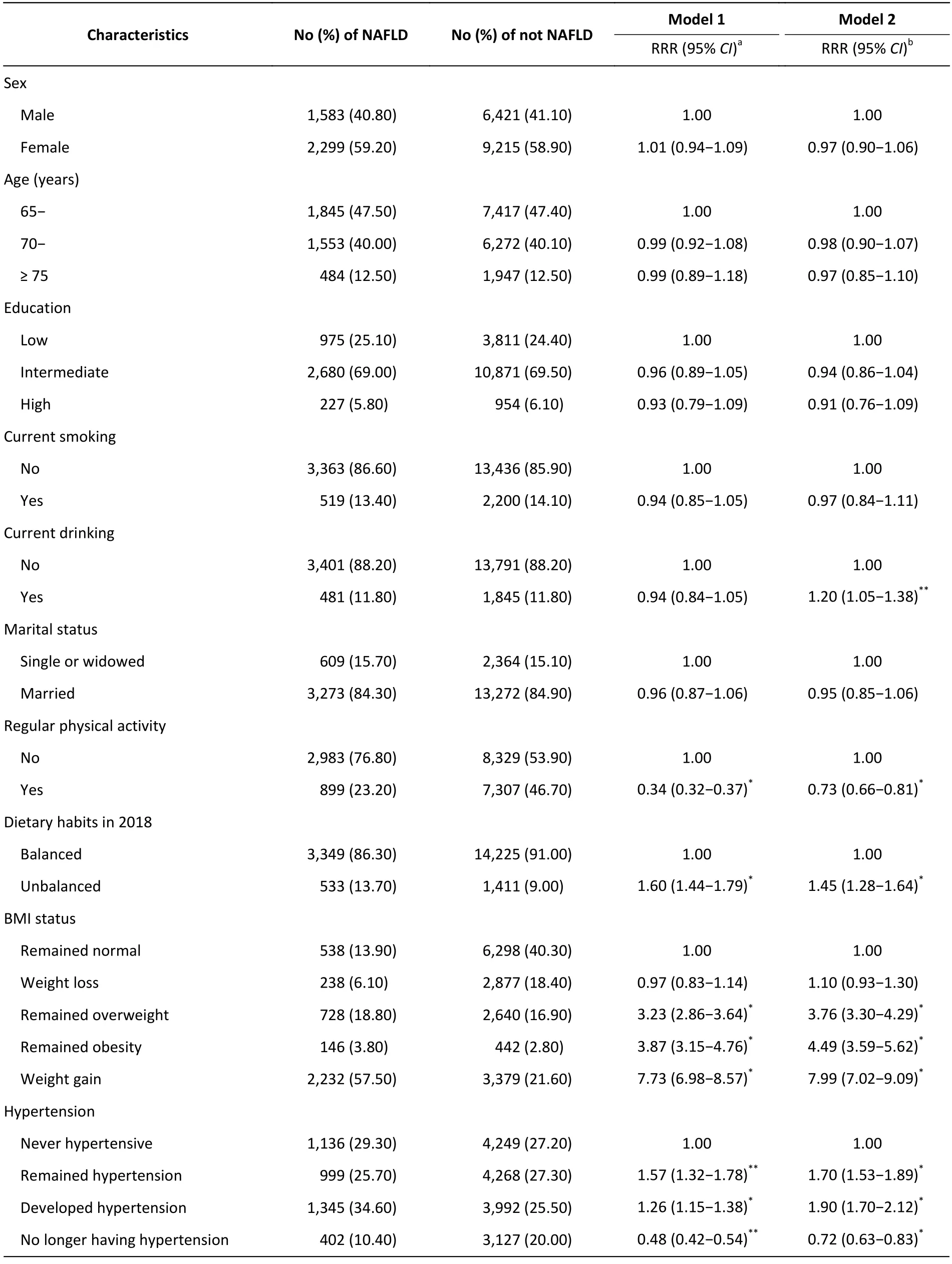
Table 3. Change in risk factors from 2018 to 2021 and the risk of developing NAFLD among participants without NAFLD in 2018 (n=19,518)
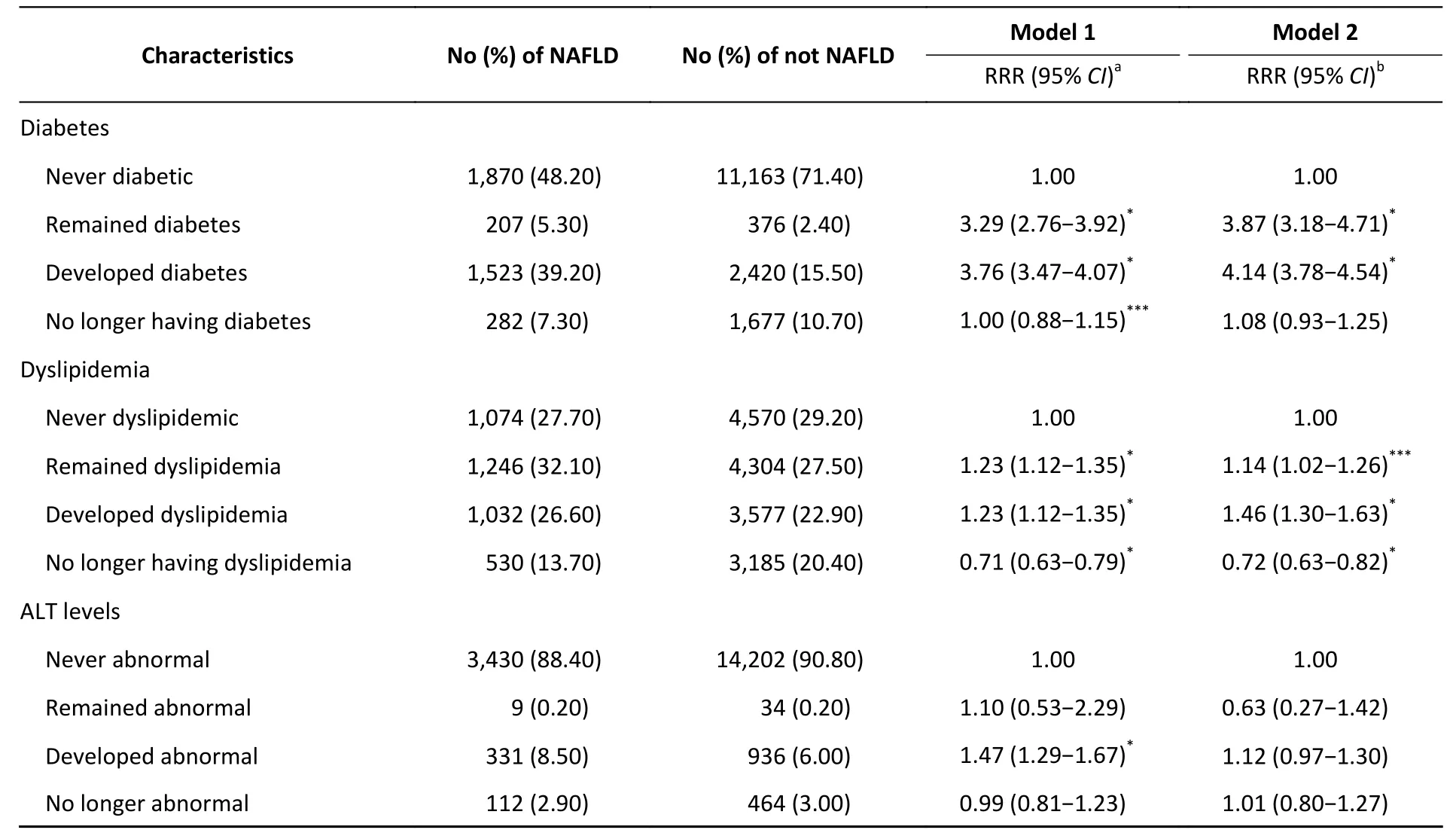
Continued
To the best of our knowledge,this is the first study to evaluate how over-time changes in the status of hypertension,diabetes,dyslipidemia,and ALT levels affect the incidence of NAFLD in the older adults in China. Moreover,the current study revealed that regular physical activity reduced the risk of NAFLD,whereas drinking and unbalanced dietary habits increased the risk.
Obesity was identified as the most important risk factor for NAFLD,as its prevalence increased in proportion to obesity.Overweight and weight gain could predict the development of NAFLD[5,6].Consistent with these studies,our findings revealed that overweight and obesity were associated with NAFLD. Further comparisons revealed that compared with those who maintained a normal weight,participants with long-term overweight and obesity had a 3.76 and 4.49 increased risk of developing NAFLD,respectively. Moreover,our study suggested that the category with the greatest risk for NAFLD was weight gain,which resulted in changes in the BMI status (RRR: 7.99,P<0.001).
Our study showed that diabetes was significantly associated with an increased risk of NAFLD,which was consistent with the findings of the American study[4].Furthermore,patients who remained with diabetes or developed it during the study period had a higher risk of NAFLD than those who did not.However,an Indian cohort study did not reveal a significant association between diabetes and NAFLD[9].The discrepancy between our study and the Indian study might be related to the sample size.Individuals in the Indian study were from a clinical cohort,thus,the conclusion might not apply to the general population.
Many studies reported that higher TG levels (OR:5.03,P<0.001) and lower HDL levels (OR: 3.99,P<0.001) are risk factors for NAFLD[7].Our study not only revealed that dyslipidemia was associated with NAFLD,but also suggested that the presence of dyslipidemia was a more important risk factor.Consistent with other studies’ findings,our results supported a positive association between hypertension and incident NAFLD[7].Moreover,no longer having hypertension or dyslipidemia was a protective factor for the development of NAFLD,indicating that NAFLD could be reversed when patients with hypertension or hyperlipidemia control their blood pressure and lipids to the normal levels.
ALT levels are positively associated with NAFLD and to some extent,can be used as a diagnostic marker for NAFLD.However,25% of patients with NAFLD showed normal ALT levels clinically;however,the elevation of ALT levels is a non-invasive indicator of NAFLD[8,10].A positive association between ALT levels and NAFLD was observed in the cross-sectional analysis of our study;however,this relationship was not detected in the longitudinal analysis.Therefore,further studies are required to verify the impact of ALT levels on NAFLD.
Our study had several strengths,as it is the first study to examine how changes in the status of hypertension,diabetes,dyslipidaemia,and ALT levels over time impact incident NAFLD in the elderly in China. Moreover,the sample size was large enough,increasing the statistical power to detect the association between relative factors and NAFLD.However,this study had some limitations.First,the participants were not from a population-based sample and might not be representative of the entire population. Second,residual confounders might have been ignored in the analysis,although some confounders were controlled in the current study.Third,the diagnostic criteria for NAFLD were based on ultrasonography,which might not be sensitive to mild NAFLD and could not clarify its severity.However,ultrasonography,as a non-invasive method,has been widely used in population-based studies because of its high diagnostic value in detecting NAFLD.
In conclusion,our study revealed that alcohol drinking,unbalanced dietary habits,long-term overweight or obesity,over-time weight gain that results in a BMI category,and the presence of diabetes,hypertension,or dyslipidemia,can increase the risk of developing NAFLD,while regular physical activity and no longer having dyslipidemia or hypertension are protective factors against incident NAFLD. Therefore,the elderly individuals should control their weight,blood pressure,and blood glucose and lipid levels to normal levels to prevent the development of NAFLD.
AcknowledgmentsWe thank the Qingdao Municipal Health Bureau and the Qingdao Municipal Center for Disease Control and Prevention,Qingdao,China,for their contributions to the field survey.
Conflict of InterestNo potential conflicts of interest.
#Correspondence should be addressed to XING Dong Ming,E-mail: xdm_tsinghua@163.com Tel: 86-15726227711.
Biographical note of the first author: LIU Li,female,born in 1986,PhD,majoring in community health and chronic non-communicable disease.
 Biomedical and Environmental Sciences2023年8期
Biomedical and Environmental Sciences2023年8期
- Biomedical and Environmental Sciences的其它文章
- The China Cardiovascular Health Index 2023 was Grandly Released
- Method for Vitamin D Deficiency Screening
- Method for Folate Deficiency Screening
- A Campylobacteriosis Outbreak Caused by One Asymptomatic Food Handler Carrier*
- Exploring Gender Differences in Adolescent Dissociative Symptoms via A Structural Equation Model*
- A Risk Assessment Model for Pancreatic Cancer Based on Cuproptosis-related Genes and Clinical Characteristics