
Hypertrophic cardiomyopathy secondary to deficiency in lysosomeassociated membrane protein-2: A case report
2023-12-03 07:52:34YeTongZhaoXiuQunCaoXiaoLinMu
World Journal of Cardiology 2023年11期
Ye-Tong Zhao,Xiu-Qun Cao,Xiao-Lin Mu
Abstract BACKGROUND Danon disease (DD),in which mutations in the X-linked lysosome-associated membrane protein-2 (LAMP-2) gene result in hypertrophic cardiomyopathy,is a rare disease,reported primarily in small samples or cases.However,with the development of cardiac magnetic resonance imaging and genetic technology in recent years,the number of reports has increased.CASE SUMMARY We report a case of DD in an adolescent male patient,confirmed by genetic testing.The patient was admitted to our hospital with complaints of a three-year history of chest tightness and shortness of breath.His preliminary clinical diagnosis is hypertrophic cardiomyopathy.Our report includes the patient’s clinical course from hospital admission to death,step-by-step diagnosis,treatment course,and noninvasive imaging features.We highlight how a noninvasive diagnostic approach,based solely on clinical and imaging “red flags” for DD,can be used to achieve a diagnosis of DD with a high degree of confidence.CONCLUSION DD is a very dangerous cardiomyopathy,and it is necessary to achieve early diagnosis and treatment.
Key Words: Danon disease;Lysosome-associated membrane protein-2 gene;Cardiomyopathy;Hypertrophy;Cardiac magnetic resonance imaging;Myocardial strain;Case report
INTRODUCTION
Danon disease (DD) is a rare,hereditary,X-linked,and dominant lysosomal glycogen storage disease,caused by a deficiency in lysosome-associated membrane protein-2 (LAMP-2)[1].The disease predominantly affects men,who usually exhibit more severe clinical manifestations and present at an earlier age than women.Clinical manifestations of DD include myocardial enlargement,skeletal myopathy,and mental aberrations[2],and the most frequent high-risk form of DD is cardiomyopathy,which can manifest as arrhythmia(s),early onset heart failure,or even sudden cardiac death.Young male patients with DD typically present with left ventricular hypertrophy,which,unfortunately,is frequently mistaken for hypertrophic cardiomyopathy or other secondary conditions related to left ventricular hypertrophy.Characterized by rapid progression and a propensity for high mortality at an early age,DD may be the most lethal cardiomyopathy in young male patients[3].In the present case study,we describe the patient’s clinical course from hospital admission to death,including all diagnostic work-ups,his treatment course,and any notable noninvasive imaging features.Herein,we emphasize the importance of utilizing unique clinical signs and imaging features for the early recognition and diagnosis of DD.
CASE PRESENTATION
Chief complaints
An 18-year-old adolescent male patient was admitted to our hospital with complaints of a three-year history of chest tightness and shortness of breath.
History of present illness
The patient’s symptoms became noticeably worse one week before his admission,with increased chest tightness,an inability to lie supine,and anuria.
History of past illness
The patient was seen at a hospital in Beijing with complaints of chest tightness and was diagnosed with non-obstructive hypertrophic cardiomyopathy,a small pericardial effusion,and chronic bilateral lung inflammation with a few interstitial changes.Additionally,the patient suffered a cerebral infarction during the hospitalization,which improved slightly after treatment.
Personal and family history
The patient denied any family history of genetic disorders or similar conditions.
Physical examination
Upon physical examination,the patient exhibited evidence of hypotension,with a blood pressure of 92/62 mmHg.He exhibited normal development,intelligence,consciousness,and retinal features.Limb muscle strength was graded as level 5 upon the first hospitalization,and muscle tone was normal;however,at the time of the final hospitalization,muscle strength in the right upper limb was grade 4,while muscle strength in the left lower,left upper,and right lower limbs were grade 1.Unfortunately,the hospital staff did not perform electromyography,skeletal muscle magnetic resonance imaging (MRI),or a pathological examination.Atrial/ventricular premature beats and ventricular blocks were visible on resting electrocardiography,although no pre-excitation was observed.
Laboratory examinations
Laboratory testing revealed elevated levels of high-sensitivity cardiac troponin T (0.187 ng/mL) and N-terminal pro-Btype brain natriuretic peptide (NT-proBNP;6,554 pg/mL),while liver function tests revealed elevated levels of creatine kinase (1075 U/L,1545 U/L,and 936 U/L),creatine kinase-MB (63 U/L,61 U/L,and 58 U/L),lactate dehydrogenase(728 U/L),alanine transpeptidase (206 U/L),and aspartate aminotransferase (273 U/L).The patient’s troponin T and myocardial enzyme levels were also elevated,suggesting secondary myocardial damage.
Imaging examinations
Left ventricular centripetal and right ventricular hypertrophy were observed on transthoracic echocardiography(ventricular septal thickness,20-31 mm;lateral wall thickness,26 mm) (Figures 1A-C).Tissue Doppler imaging revealed increased end-diastolic filling pressure,with an E value of 70 cm/s (Figure 1D),a ventricular septum e′ value of 3 cm/s,and a lateral wall e′ value of 4 cm/s (Figures 1E and F).
The patient underwent coronary computed tomography (CT) angiography with maximum intensity projection,excluding acute coronary syndrome,which revealed the patency of the lumen of the coronary trunk and its branches(Figure 1G).To further characterize the cardiac phenotype,a cardiac MRI (CMRI) was performed,which revealed bilateral ventricular hypertrophy,severe trabecularization of the biventricular wall,and minor pericardial effusion.Additionally,myocardial strain analyses of the entire left ventricle (Figure 2A),as well as each segment,were performed.The 16-segment bullseye diagram and longitudinal strain map revealed varying degrees of strain reduction in each segment of the patient’s left ventricle,indicating myocardial injury (Figures 2B and C).The ventricular myocardium exhibited substantial late gadolinium enhancement (LGE) on MRI,sparing the mid-basal septum but involving the apex(Figures 1H and I),which is a unique imaging characteristic of DD[4].
FINAL DIAGNOSIS
After reviewing the patient’s gene sequencing,in conjunction with the aforementioned data,the patient’s final diagnosis was DD.
TREATMENT
The patient experienced ventricular thrombosis,pulmonary thrombosis,pulmonary hypertension,and cerebral infarction in previous hospitalization,which required the administration of the cardiotonic medication digoxin and the anticoagulant warfarin.The patient and his family approved a therapeutic regimen;however,after undergoing treatment with the medications for >1 mo,the patient’s chest tightness worsened,anuria developed,and his lungs started to crackle.Additionally,paroxysmal atrial fibrillation was detected on resting electrocardiography and laboratory results showed an additional elevation in high-sensitivity cardiac troponin T (0.527 ng/mL) and NT-proBNP (84,072.43 pg/mL) concentrations,as well as hyperkalemia (potassium level,6.4 mmol/L).Multislice chest CT revealed serious infection in both lungs.The patient was treated with diuretics,nutritional supplementation for the myocardium,anticoagulants,and antiinfection therapy for one week.However,he did not show any significant improvement.
OUTCOME AND FOLLOW-UP
The patient’s prognosis continued to be poor,and he subsequently exhibited signs of entering a deep coma and died,despite attempts at active resuscitation.
DISCUSSION
DD is a highly penetrant vacuolar myopathy caused by a primary deficiency in LAMP-2[5].This condition usually involves the skeletal muscle and myocardium and can be definitively diagnosed through a biopsy.The characteristic pathological features of DD include intracytoplasmic vacuoles harboring autophagic components and glycogen[1].The classic “trifecta,” which includes cardiac enlargement,skeletal myopathy,and abnormal liver function,is used to definitively diagnose patients with suspected DD[5].Other red flags,such as pre-excitation on resting electrocardiography,are not always present in patients with DD.Although the patient presented herein did not undergo a skeletal muscle biopsy,his decreased muscle strength,in combination with an increase in creatine kinase concentrations,indicated the presence of skeletal muscle damage.
A distinctive LGE pattern and basal septum preservation,seen on CMRI,may help distinguish DD from sarcomeric or other hypertrophic cardiomyopathy phenotypes[4,6] and strengthen a suspected diagnosis of DD.Physicians should confirm cardiac hypertrophy,impaired liver function,and a genuine pattern of progressive gadolinium enhancement on CMRI to diagnose DD.To date,CMRI findings in patients with DD have been described in only a few case reports[4].CMRI provides accurate imaging of morphological structures and tissue characteristics,such as unusual LGE patterns,which may have practical utility in the identification and differential diagnosis of cardiomyopathy in patients with DD.Additionally,adding myocardial fibrosis to the list of indicators of DD may be appropriate.For the first time,we added feature-tracking technology to investigate cases of DD.The analysis of global and segmental longitudinal myocardial strain using CMRI-feature tracking revealed that both were damaged;however,no other unique features were observed.We speculate that the patient presented herein was in the late stage of heart failure,although he had left ventricular noncompaction,which differs from the preservation of normal apical strain patterns described in previous reports.We hope that more patients with DD will undergo feature-tracking analysis in the future,to further characterize the unique features of cardiac strain seen in these patients.
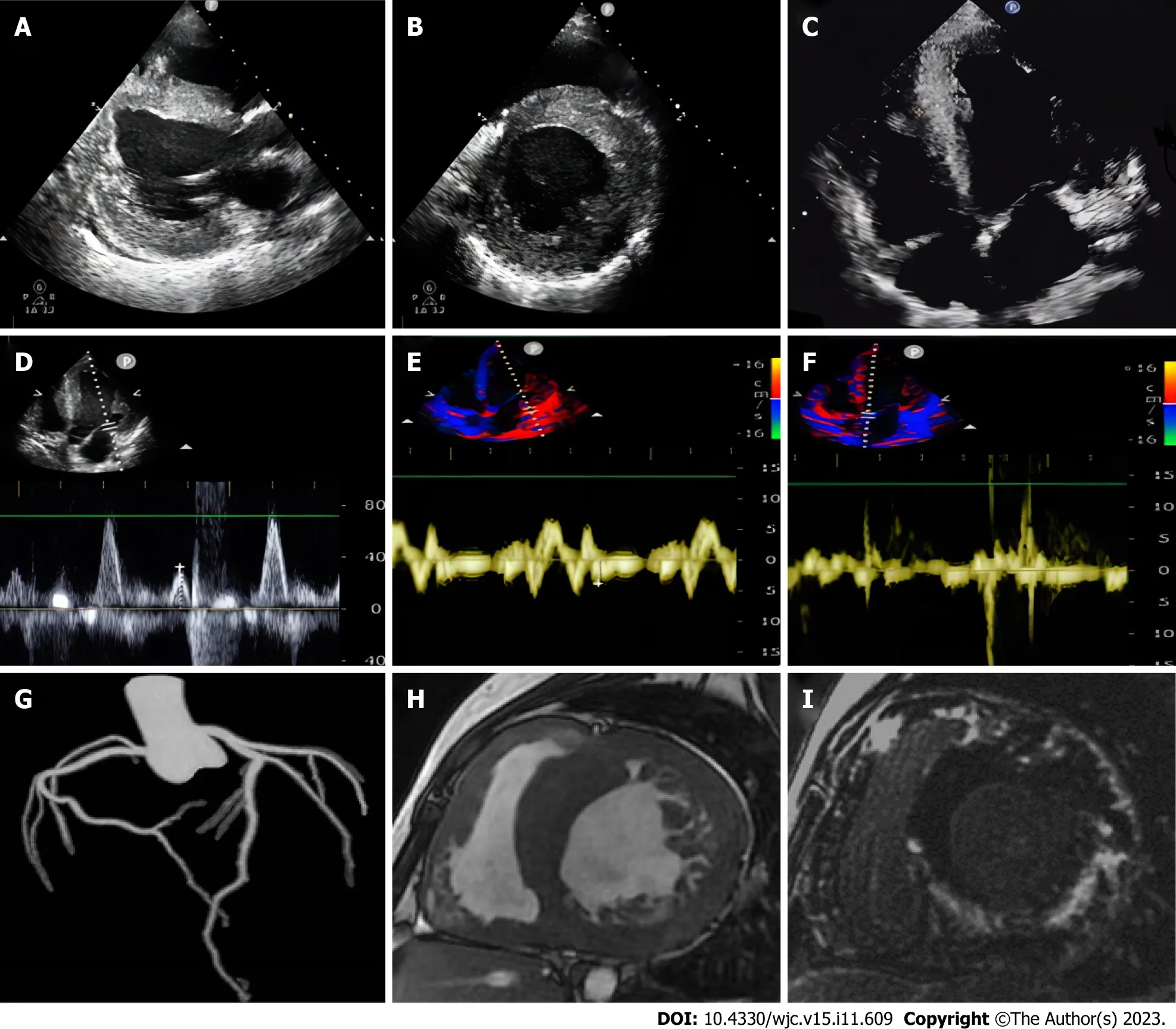
Figure 1 Imaging features of the male patient. A: Transthoracic echocardiography shows left ventricular centripetal hypertrophy in parasternal long axis view;B: Transthoracic echocardiography shows left ventricular centripetal hypertrophy in parasternal short axis view;C: Transthoracic echocardiography shows left ventricular centripetal hypertrophy and right ventricular hypertrophy in long axis view;D: Tissue Doppler imaging shows increased end-diastolic filling pressure in the left ventricle,with an E value of 70 cm/second;E: Tissue Doppler imaging shows increased end-diastolic filling pressure in the left ventricle,with e' (lateral wall) value of 4 cm/second;F: Tissue Doppler imaging shows increased end-diastolic filling pressure in the left ventricle,with e' (ventricular septum) value of 3 cm/second;G:The coronary tree’s maximum intensity projection displays the patency of each branch lumen;H: Cardiac magnetic resonance short-axis cine shows diffuse thickening of the biventricular wall,excessive myocardial trabeculation,and pericardial effusion;I: Late gadolinium enhancement of the short axis demonstrates extensive late gadolinium enhancement of the biventricular wall,sparing only the basal segment septum.
The clinical results of treating DD depend on the severity of cardiomyopathy,which can be difficult to identify,frequently being discovered only in the presence of clinically significant symptoms.In the case presented herein,substantial myocardial injury,cardiac insufficiency,and arrhythmia were the secondary causes of numerous organ disorders that ultimately led to the patient’s death.Physicians should be aware that young males exhibiting myocardial hypertrophic changes,elevated plasma creatine kinase levels,pre-excitation syndrome on electrocardiography,and/or distinctive LGE on CMRI may have DD;therefore,abnormal clinical or laboratory results and CMRI features can be used to diagnose and distinguish DD from other diseases.Furthermore,the aforementioned data allow a diagnosis to be made in a noninvasive manner,providing an alternative to the current gold standard for the diagnosis of DD– genetic testing for LAMP-2 deficiency/mutations.Although there is currently no specific gene therapy for DD,the adenovirus-mediated delivery of a functional LAMP2B transgene has been achieved in a mice model,the efficacy of which is being tested in adolescent male patients with DD.
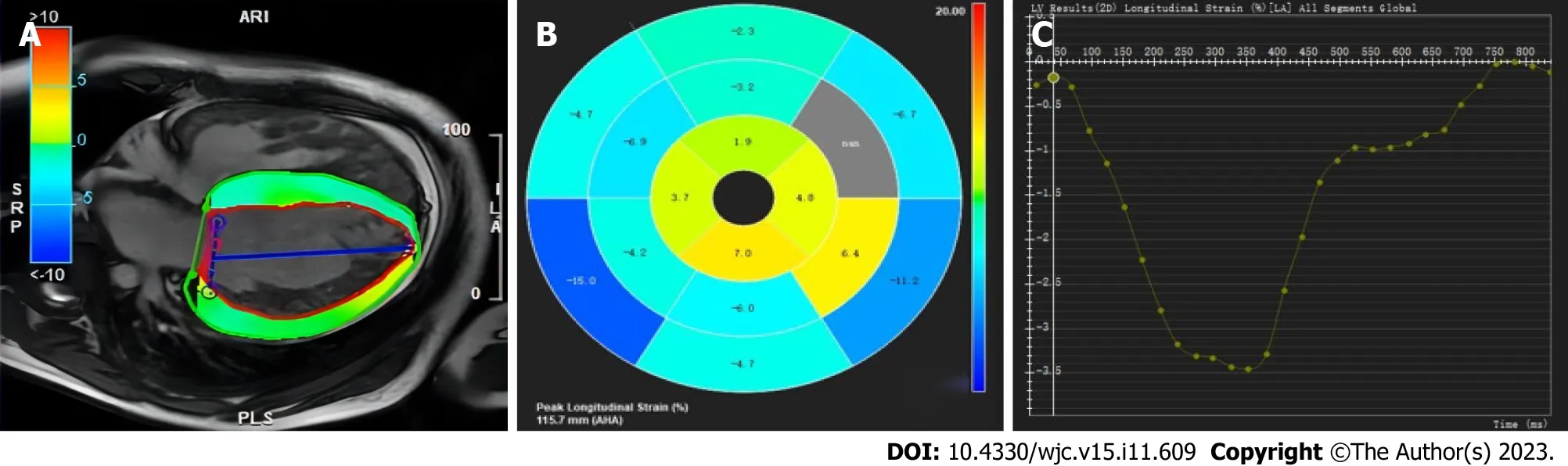
Figure 2 Feature Tracking strain measurements. A: Cardiac magnetic resonance feature tracking with longitudinal strain overlay on a four-chamber cine steady-state free procession image;B: Bull’s-eye diagram of strain in each segment in the left ventricular myocardium of the same patient;C: The map show the longitudinal strain values.The vertical axis shows longitudinal strain (%),and the horizontal axis shows the time in ms.
The Dalian Municipal Central Hospital Affiliated to Dalian Medical University Ethics Committee approved the present case study (No.YN2023-003-04).The patient’s parents consented to the publication of anonymized case details.
CONCLUSION
In summary,the authors would like to emphasize the importance of the early diagnosis of DD,which facilitates advanced treatments,such as targeted gene therapy,cardiac transplantation,or the installation of an implantable cardioverter defibrillator.A deeper understanding of the unique clinical signs and imaging features of DD is needed,particularly with the use of CMRI.Genetic testing should also be performed as early as possible to increase diagnostic accuracy.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the patient and his family for their participation in the present case study.
FOOTNOTES
Author contributions:Cao XQ and Mu XL collected the clinical data;Mu XL and Zhao YT analyzed and interpreted the clinical data;Zhao YT drafted the manuscript;Mu XL guided the completion of this article,supervising and revising the manuscript for intellectual content;All of the authors have read and approved the final manuscript.
Informed consent statement:Written informed consent was obtained from the patient’s parents for the publication of this report and any accompanying images.
Conflict-of-interest statement:All the authors have no conflicts of interest to declare.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Xiao-Lin Mu 0000-0003-3449-9658.
S-Editor:Liu JH
L-Editor:A
P-Editor:Yuan YY
 World Journal of Cardiology2023年11期
World Journal of Cardiology2023年11期
- World Journal of Cardiology的其它文章
- Down syndrome child with multiple heart diseases: A case report
- Clinical impact of portal vein pulsatility on the prognosis of hospitalized patients with acute heart failure
- Novel predictors of permanent pacemaker implantation following transcatheter aortic valve replacement
- Cardiovascular implications of inflammatory bowel disease: An updated review
- Acute myocardial infarction in myeloproliferative neoplasms