
Prone-positioned upside-done arch exercise, a kind of lumbodorsal muscles training,curbs the progression of lumbar disc bulge
2018-08-27 10:50:06ZengJieGaoJiuYiChenYangLiuGuiyangCollegeofTraditionalChineseMedcineGuiyangChinaFirstHospitalAffiliatedtoGuiyangCollegeofTraditionalChineseMedicineGuiyangChina
TMR Non-Drug Therapy 2018年1期
Zeng-Jie Gao, Jiu-Yi Chen, Yang LiuGuiyang College of Traditional Chinese Medcine, Guiyang, China; First Hospital Affiliated to Guiyang College of Traditional Chinese Medicine, Guiyang, China.
Abstract Objective: To study the effects of prone-positioned upside-done arch exercise, a kind of lumbodorsal muscles training originated from Yoga, on curbing the progression of lumbar disc bulge. Methods: A total of 120 out-patients, diagnosed with lumbar disc bulge by CT and/or MRI, were randomly divided into the observation group and the control group, with 60 patients in each group. Patients in the observation group received the prone-positioned upside-done arch exercise combined with traction and acupuncture for two months and followed with a two-year treatment with prone-positioned upside-done arch exercise while the patients in the control group only received traction and acupuncture for two months.After two years, patients in both groups were investigated for the visual analogue score, MR image and straight leg raise tests. Results: Compared to the control group, prone-positioned upside-done arch exercise combined with traction and acupuncture showed significant decrease in patients’ visual analogue score, bulge size and the positive ratio of straight leg raise test (P = 0.001, P = 0.001 and P = 0.02 respectively), suggesting the inhibitory effect on the progression of lumber disc bulge. Conclusion: Prone-positioned upside-done arch has the potentials to protect patients with lumbar disc bulge from nerve root compression syndrome.
Key words: Prone-positioned upside-done arch, Yoga, Lumbar disc bulge, Exercise
Background
Lumbar disc bulge and disc protrusion were usually diagnosed by CT and/or MR. However, lumbar disc bulge with low back pain does not mean lumbar disc protrusion,which is a condition related to nerve root compression syndrome normally that needs surgical intervention if more than three months’ conservative treatment shows no effect. As one of the most common types of musculoskeletal pain in the world, lumbar disc bulge combined with discogenic chronic back pain could result in not only muscle weakness and muscle imbalance of the lumbar region, but also reduction of re-positioning ability,leading to spine unstability due to the decreased proprioceptive sense [1-4].
According to current evidence-based clinical guidelines, various exercise programs, one of the nonoperational treatments of lumbar disc bulge, should be implemented in individuals with chronic low back pain[5]. The function of lumbodorsal muscles training centering the spine has been proved to be effective in alleviating pain and improving function, which has drawn the attention of physicians to utilize all sorts of exercise regime to train the muscles around the spine [1-4].Prone-positioned upside-done arch exercise is known as Locust Pose in Yoga originated in ancient India, which has been widely accepted by clinicians and patients.Different scholars have shown that different exercise regimes, including prone-positioned upside-done arch exercise, mostly showed positive effects on relieving pain caused by lumbar disc bulge. However, its effect combined with traditional Chinese treatment on curbing the progression of lumbar disc bulge into disc protrusion with nerve root compression has not been thoroughly studied.
In this study, a clinical controlled trial was designed to determine the positive effect of prone-positioned upside-done arch exercise on curbing lumbar disc bulge into lumbar disc protrusion with nerve root compression syndrome.
Materials and methods
Patients
120 out-patients, aged 16 to 45 years, with the complaint of chronic low back pain were selected as cases from June 2014 to June 2015. Inclusion criteria: (1) Lumbar disc bulge were found with CT and/or MR. (2) Straight leg raising tests and Bragard sign were negative. (3) All patients were suffering from chronic low back pain more than 3 months but denied the discomfort of calves and toes such as numbness and soreness, indicating the absence of nerve root compression. (4) No intermittent claudication was claimed. Exclusion criteria: (1)Lumbar gluteal myofascitis. (2) Piriformis syndrome. (3)The third lumbar vertebra processes transversus syndrome. (4) Ischiogluteal bursitis. (5) Inflammation of superior clunial nerves. (6) Disabledpatients suffering from various kinds of serious diseases. (7) Patients who were going through physical exercises programs in the past three months. All patients signed written consent on this research. This research was approved by the ethics committee of The First Hospital Affiliated to Guiyang College of Traditional Chinese Medicine (No.KY2014-017).
120 patients (83 male and 37 female) were randomly divided into two groups: the observation group and the control group, with 60 patients in each group. The patients in the observation group prescribed the therapy of traction, acupuncture and prone-positioned upside-done arch exercise while those in the control group only prescribed the therapy of traction and acupuncture. Two months later, patients in the observation group will continue to receive a two-year treatment of prone-positioned upside-done arch exercise.After two years, patients in both groups were investigated for visual analogue score (VAS), MR image and straight leg raise (SLR) tests.
Method of pelvic traction, acupuncture and prone-positioned upside-done arch exercise
Pelvic traction. All patients were tracked in a supine position with the thoracic cages and pelvis fixed with traction belt. The initial tractive force for each patient was calculated by the following formula. Initial tractive force= 15% × body weight + 40kg. When the initial tractive force cannot be endured by the patient, the force would be decreased to the level that the patient can endure. The maximum tractive force should be not exceeding the body weight of the patient undergoing the traction. One traction cycle lasted 30 minutes. This program lasted 5 times per week.
Acupuncture. All patients were needled in a prone position after the skins were sterilized. The points of Jiaji(EX-B2), Dachangshu (BI25), Shenshu (BL23) and Weizhong (BL40) were needled. All patients were performed this manipulation 30 minutes each time, 5 days per week.
Prone-positioned upside-done arch exercise. Patients in the observation group went through the prone-positioned upside-done arch exercise as required and trained by a physical therapist. The patient is in a prone position with head up, upper limbs poster superiorly stretched, and lower limbs bent anterior superiorly. The whole body bent like a flying swallow or an inverted arch (Figure 1).Patients performed this procedure 5 minutes each time,two times a day.

Figure 1 Prone-positioned upside-done arch exercise
Outcome measures:

Figure 2 Visual Analogue Score
VAS is a psychometric response scale which can be used in questionnaires, which is a measurement instrument for subjective characteristics or attitudes that cannot be directly measured (Figure 2). When responding to a VAS item, respondent specify a mark along a ruler with scales from 0 to 10, indicating his/her level of pain. The score is determined by measuring the distance (mm) on the back of ruler (total length 100 millimeter) between the “no pain” anchor and the patient’s mark, providing a range of scores from 0 - 10. The following cut points on the pain VAS have been recommended: no pain (0 - 4 mm, 0 - 0.4 score), mild pain (5 - 44 mm, 0.5 - 4.4 score), moderate pain (45 - 74 mm, 4.5 - 7.4 score), and severe pain (75 -100 mm, 7.5 - 10 score).
Protrusion size were measured via MR according to what Thelander once introduced and this is widely accepted in clinical practice [6] (Figure 3). The sagittal diameter of the protruding intervertebral disc was the maximum anterior and posterior diameter at the point of the protrusion (AB). The transverse diameter is the vertical diameter of the middle point of the sagittal diameter (CD).The sagittal diameter of the spinal canal was the maximum anterior and posterior diameter of the tissues and their sensitivity to mechanical stress or compression. The sagittal diameter of the spinal canal was the maximum anterior and posterior diameter of the spinal canal at the same level (EF), and the transverse diameter of the spinal canal was also obtained (GH).Sagittal and horizontal indices = (AB × CD) / (EF ×GH), sagittal indices = AB / EF.
SLR is a passive test. Each leg is tested individually and the normal leg being tested first. When performing the SLR test, the patient is positioned in supine without a pillow under his/her head, the hip medially rotated and adducted, and the knee extended. The clinician lifts the patient’s leg by the posterior ankle while keeping the knee in a fully extended position. The clinician continues to lift the patient's leg by flexing at the hip until the patient complains of pain or tightness in the back or back of the leg. In normal situation, the elevation degrees can reach 80-90 degrees. When the elevation degrees is less than 70° and the patient presents radiative pain in the back of the lower limb, SLR result is thought to be positive.
Statistical analysis
The data were analyzed by SPSS 22.0 software,measurement data were showed by mean ± standard deviation (ˉx ± s). Self-controlled data were in accordance with normal distribution using paired t test,otherwise using rank sum test. Multiple groups’ means were compared with single factor analysis of variance,and the comparison between groups was performed with least significance difference method or Dunnett method.Qualitative variables were compared by using Chi-square test.
Results
During the process, 16 participants in the observation group dropped out after two months due to personal willingness and other reasons. However, at the end of the research, we still recalled all of them to participate in our physical examination and MR scan under their consent because all of them denied any other alternative treatments during the 2 years’ time. As even a short-term lumber muscles’ training might have positive results, the efficacy of the study is controllable. 5 patients in the control group dropped out at the end of the first 2-month treatment and sought other treatments. Then we further recruited another 5 candidates for supplement.
The short-term and long-term therapeutic effects were compared as follows: the comparison of the two groups’basic information and short term therapeutic effects showed no statistical significance (P > 0.05) (Table 1and 2), while the 2-year therapeutic effects showed statistical significance. Two years later, the VAS, bulge size and the positive ratio of SLP test in observation group were less than those of control group (P = 0.001, P = 0.001 and P =0.02 respectively) (Table 2-4, Figure 4), indicating that majority patients in observation group didn’t manifest the syndrome of nerve root compression and the comprehensive therapy containing prone-positioned upside-done arch exercise has obvious effect on curbing the progression of lumber disc bulge.
Discussion
In the past, many scholars studied the effect of prone-positioned upside-done arch exercise on curing chronic low back pain [1-4, 10, 13]. However, the connection between prone-positioned upside-done arch exercise and lumbar disc bulge as well as lumbar disc herniation with nerve root compression syndrome has not been fully studied. Our study found that prone-positioned upside-done arch exercise effectively alleviated pain and curbed the degenerative process of the lumbar disc bulge into disc herniation.
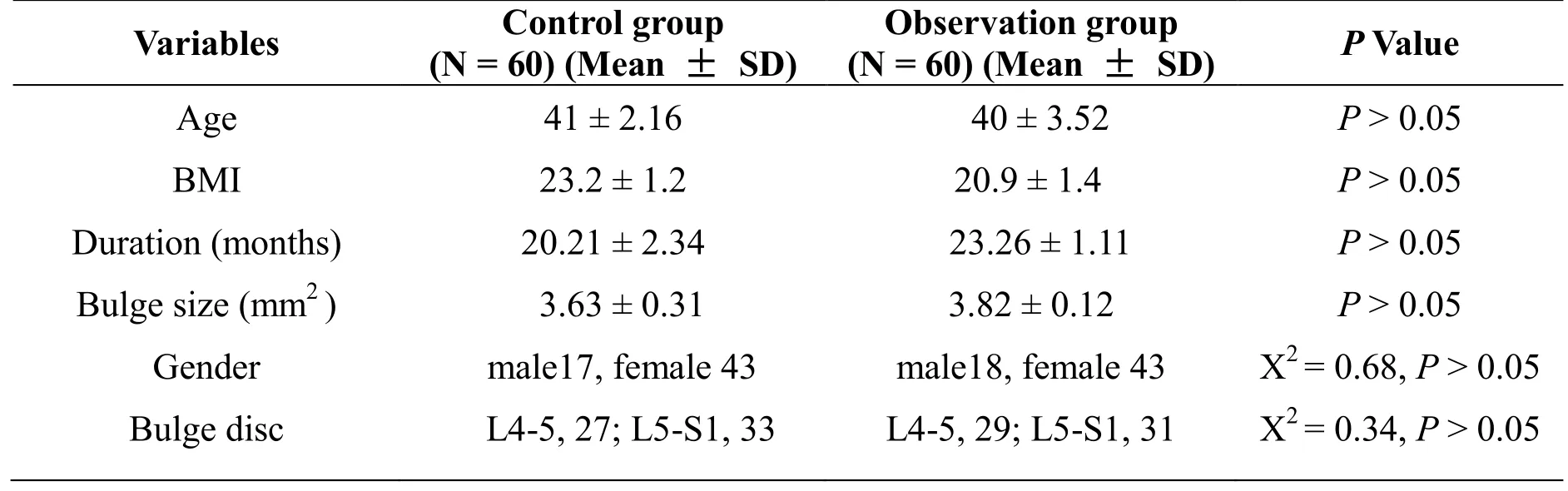
Table1 Comparision of basic information
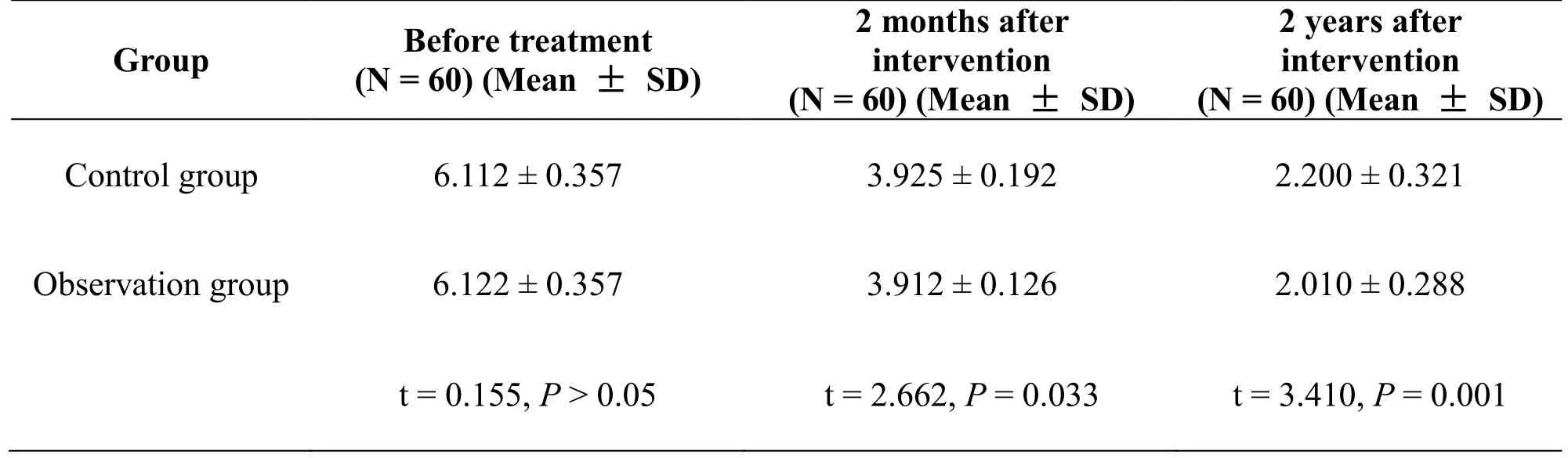
Table 2 Comparison of Visual Analogue Score
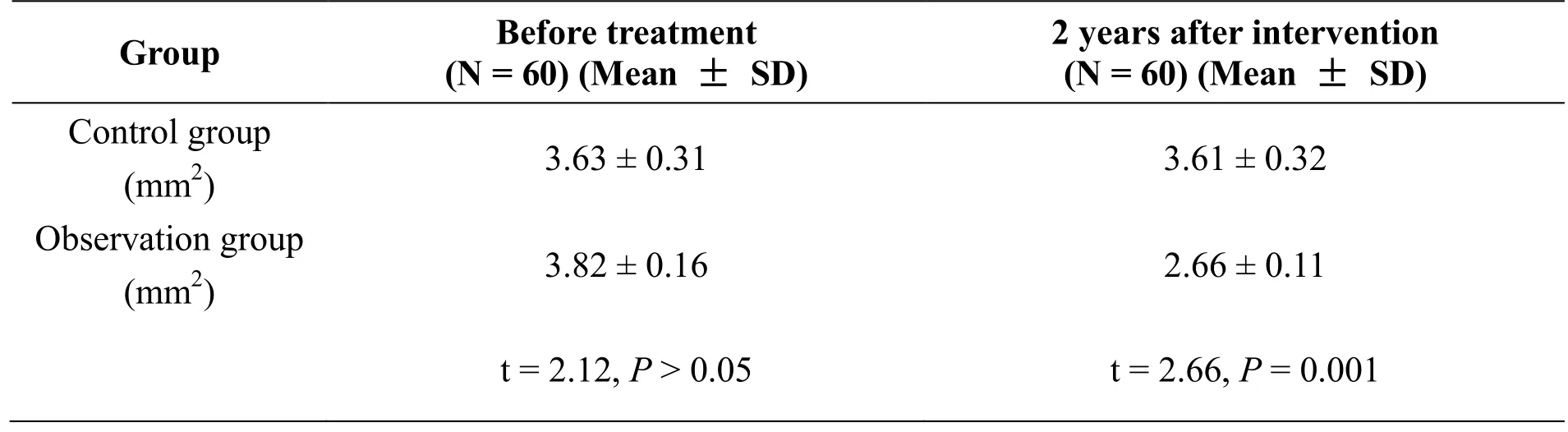
Table 3 Comparision of Bulge size

Table 4 Positive ratio of straight leg rising test

Figure 4 A. MR photograph showed a bulge in L4 B. MR image showed improvement after two years intervention
In many studies and clinical practice, disc bulge or protrusion rather than nerve root compression was misused as the gold standard for surgical operation.However, disc bulge has been found to be asymptomatic in many subjects [7-9]. There were also some patients with chronic or discogenic low back pain who experience some extent of bulge or protrusion on L3-S1 but showed no syndrome of nerve root compression.
The mechanism of discogenic low back pain and malfunction of lumbar muscles have been studied by many scholars. O’Sullivan PB and Park SY found that chronic back pains aggravated the instability of the lumbar spine as well as caused degenerative changes,atrophy of muscle strength, and reduce flexibility and joint range of motion [10, 11]. There was also emerging evidence that lumbar herniated nucleus pulposus occurred not due to lumbar pain or disability, but often due to deterioration of the related muscles around affected area[12].
Now, various types of composite exercises and core exercises in addition to exercises for muscular strength and stability are currently being utilized for the treatment of chronic low back pain [12, 13]. Lumbar and trunk muscle extension exercise therapies, including prone-positioned upside-done arch exercise, were found to be helpful to stabilize the lumbar spine through adjusting lumbar and trunk dynamically, and increasing muscle strength [12]. Weinstein JN and Jensen MCs’studies showed that exercise rehabilitation approaches for strength and stability, including prone-positioned upside-done arch exercise played a key role in postoperative intervention due to restricted activities of post-operative patients [14, 15]. Prone-positioned upside-done arch exercise has been recommended for the purpose of preventing recurrence of pain and improving the function lumbar spine [16-20].
According previous literature, lumbar muscles training mainly works in the following ways: (1) Strengthen the muscles around the spine and improve endogenous stability. (2) Improve blood circulation of and accelerate inflammation elimination. (3) Relax tissue adhesion and improve internal milieu. However, physicians lumbodorsal muscle’s training usually neglected the necessary medical education regarding lumbodorsal muscle’s training, which result in many patients to suffer from lumbar disc bulge and have the possibility to progress into lumbar disc herniation. It is accompanied with nerve root syndrome that needs surgical intervention and much economic cost. In this study, VAS, bulge size and the SLR test manifestation were improved after treatment, indicating the comprehensive therapy consisting of prone-positioned upside-done arch exercise has the potentials to curb the progression of lumber disc bulge into lumbar disc herniation with the syndrome of nerve root compression.
There are some shortcomings in our research. Firstly,the detailed changes of the muscles’ power and width around the spine were not detected. Secondly, patients’implementation of this physical operation cannot be fully monitored because the programs need to be done by themselves after they have understood how to perform the exercises. During the process, potential interference might be hidden and ignored by patients who probably sought for other alternatives. Thirdly, the follow-up more than 2 years is required to conform the protective effect of prone-positioned upside-done arch exercise.

- TMR Non-Drug Therapy的其它文章
- Acupuncture therapy in a patient with radial nerve injury
- Comparative study for cardiovascular risk factors of rheumatoid arthritis and osteoarthritis
- The beneficial effects of non-drug therapy on osteoarticular disease
- The clinical progress and potential mechanism of massage therapy on knee osteoarthritis
- TMR Non-Drug Therapy: the modernization of non-drug therapy