
Arteriosclerosis Obliterans Presenting as Multiple Leg Ulcers: A Case Report
2019-10-16 11:05:14LeiShaoRuiHuaFangJiangWuQunLiLiJieChenJianQinWang
國際皮膚性病學(xué)雜志 2019年3期
Lei Shao, Rui-Hua Fang, Jiang Wu, Qun Li, Li-Jie Chen, Jian-Qin Wang,?
1Institute of Dermatology, Guangzhou Medical University, Guangzhou, Guangdong 510095, China, 2Department of Dermatology,Guangzhou Institute of Dermatology, Guangzhou, Guangdong 510095, China, 3Department of Dermatology, Guangzhou First People’s Hospital, Guangzhou Medical University, Guangzhou, Guangdong 510180, China.
Introduction
Arteriosclerosis obliterans (ASO) is characterized by the ischemic symptoms of lower extremity, which are due to the stenosis and/or occlusion of artery based on the pathology of atherosclerotic change,mainly involving the large-and medium-sized arteries.Pain and ulcers of the leg are the main causes of patient seeking medical aid;however, a presentation of multiple ulcers is rare. Herein we report a case of ASO presenting as multiple leg ulcers.
Case report
A72-year-oldmanwithnonpainfulskinulcersontheleftleg for 1 year presented at Guangzhou First People’s Hospital in Oct 2017. The patient had first noticed the ulcers 1 year earlier, and most of the ulcers had healed on their own within a few weeks.However,new ulcers with intermittent claudication subsequently developed and had not healed for the past 2 months. The patient reported chest pain with a squeezing sensation or discomfort for almost 1 month.Except for a smoking history of 30 packs a month, his medical history was otherwise unremarkable.
Physical examination revealed multiple dry ulcers with 1-2cm diameter on the left leg with a low skin temperature(Fig. 1A and 1B), and the pulse of the left dorsalis pedis artery was weak. No enlarged surface lymph nodes were palpable. Color Doppler ultrasound, computed tomography(CT)angiography(Fig.2A and 2B),and arteriography(Fig.3A and 3B)indicated that the left external iliac artery was obstructed and that the right common iliac-external iliac artery had multiple mixed plaques with a cavity that had narrowed by 60%-70%.Based on the patient’s clinical manifestations and imaging findings,the diagnosis of ASO was confirmed.

Figure 1. Skin lesions at different stages. (A and B) Clinical manifestation at the first visit was characterized by multiple 1- to 2-cm dry ulcers on the left leg.(C and D)The leg ulcers healed after 10 days of interventional therapy.
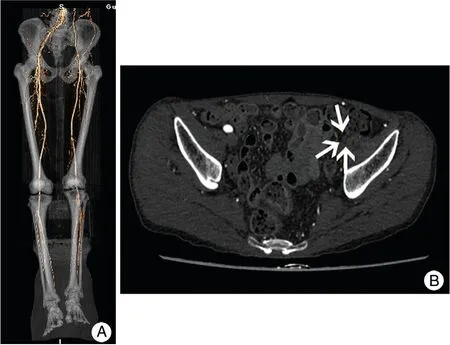
Figure 2. Computed tomography angiography of both lower limbs showed that the left external iliac artery was obstructed. (A)Computed tomography angiography showed that the left external iliac artery was obstructed and that the right common iliac-external iliac artery had multiple mixed plaques with a cavity that had narrowed by 60%-70%. (B) White arrows showed that the left external iliac artery was obstructed.
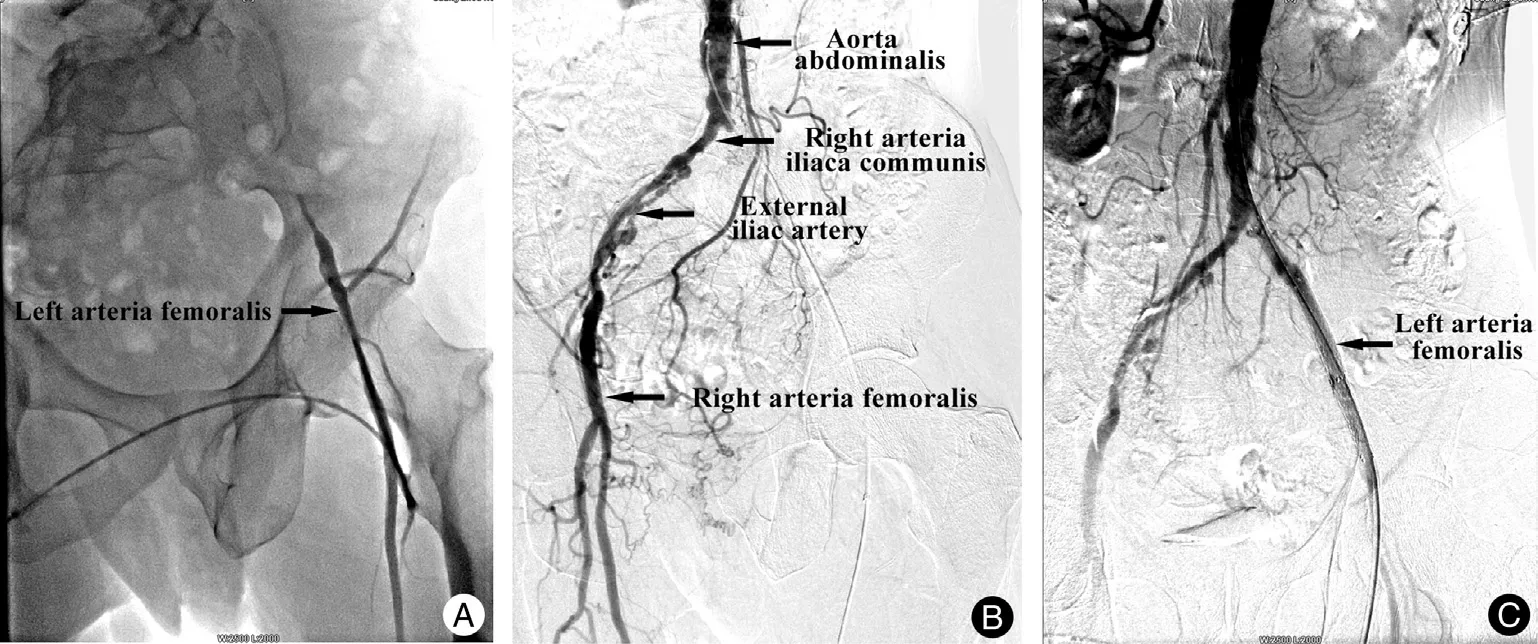
Figure 3. Arteriography before and after treatment.(A and B)The left external iliac artery was completely occluded before treatment.(C)Normal flow of the left external iliac artery returned after interventional therapy.
The patient was treated with interventional therapy;two stents (10mm×8cm and 8mm×8cm) were implanted into the left iliac artery.Angiography showed a significant improvement,with normal blood flow in the region of the left iliac artery stenosis (Fig. 3C). By 10 days postoperatively, the leg ulcers had healed, the leg pain had disappeared, and the skin temperature had returned to normal (Fig. 1C and 1D).
Discussion
ASO is characterized by lower extremity ischemia that causes intermittent claudication,pain while resting,and gangrene.Lower extremity ASO significantly affects 17% of people aged 55-75 years worldwide.1Early diagnosis and treatment are necessary.Risk factors for ASO include older age,male sex,smoking, hypertension, hyperlipidemia,diabetes mellitus,chronic renal failure,and hyperhomocysteinemia.2The clinical symptoms and severity of ASO are related to the location, degree, speed, and range of the vessel blockage,embolization formation,and collateral circulation establishment.Therefore,its clinical manifestations are variable,and this may lead to misdiagnosis or mistreatment.A decreased skin temperature and numbness and intermittent claudication of the affected limbs can occur in the early stage.As the disease progresses,the toes,feet,and lower leg may develop persistent pain at rest, embolization, ulceration, and dry gangrene;however,multiple ulcers are rare.
Early diagnosis can be achieved by color Doppler ultrasound, arteriography, magnetic resonance imaging,and CT angiography.Balloon angioplasty procedures and stent implantations yield immediate positive results and have thus become the main approaches to treat ASO.1However,some studies have revealed that about 30%-50%ofpatientsdeveloppost-angioplastyrestenosiswithin1year after the procedure and that 12%of patients develop severe ischemia and eventually require amputation.3-4The prognosis of ASO is closely related to complications;about 70%-80%of the patients with lower extremity ASO die of cardiovascular disease.5
The clinical manifestations in the present case were multiple leg ulcers and pain at rest; gangrene was absent and therefore can be easily misdiagnosed as vasculitis.The causes of multiple ulcers are still under investigation, and we speculate that good collateral circulation reconstruction of the lower extremities after occlusions of a lower limb artery is an important condition for multiple leg ulcers. ASO is not uncommon in clinical practice, but its pathogenesis and clinical manifestations are complex.Reliance on a dermatologist alone to make the diagnosis is difficult; instead, the joint efforts of clinicians from multiple disciplines, including cardiovascular imaging physicians and radiologists, are necessary for an accurate clinical diagnosis.
Acknowledgements
The authors thank Dr. Shuo-Yi Ma and Dr. Cui-Hua Gao for their help on the imaging images preparation and Dr. Xi-Bao Zhang for his help on manuscript editing.
- 國際皮膚性病學(xué)雜志的其它文章
- Solid-Cystic Hidradenoma
- Interstitial Mycosis Fungoides with Systemic Sclerosis-Like Features: A Case Report
- Nasal Type Extranodal NK/T-Cell Lymphoma Presenting with Unilateral Facial Erythemas,Nodules, and Necrosis
- Lentigines within Nevus Depigmentosus
- Subungual Exostosis Misdiagnosed as Subungual Wart
- Severe Port Wine Stain with Significant Nodules and Alveolar Bone Invasion Leading to Restricted Mouth Opening