
Potential rules of anesthetic gases on glioma
2020-04-16 07:08:12XiaoChenYiGuangMaoZhengQuanYuJiangWuGangChen
Medical Gas Research 2020年1期
Xiao Chen,Yi-Guang Mao,Zheng-Quan Yu,Jiang Wu,Gang Chen
Department of Neurosurgery & Brain and Nerve Research Laboratory,The First Affiliated Hospital of Soochow University,Suzhou,Jiangsu Province,China
Abstract
Glioma is one of the most frequent primary brain tumors.Currently,the most common therapeutic strategy for patients with glioma is surgical resection combined with radiotherapy or/and adjuvant chemotherapy.However,due to the metastatic and invasive nature of glioma cells,the recurrence rate is high,resulting in poor prognosis.In recent years,gas therapy has become an emerging treatment.Studies have shown that the proliferation,metastasis and invasiveness of glioma cells exposed to anesthetic gases are obviously inhibited.Therefore,anesthetic gas may play a special therapeutic role in gliomas.In this review,we aim to collect existing research and summarize the rules of using anesthetic gases on glioma,providing potential strategies for further clinical treatment.
Key words:anesthetic gases; glioma; invasion; isoflurane; metastasis; proliferation; sevoflurane
InTRODUcTIOn
Tumors derived from neuroepithelial cell are collectively referred to glioma,which account for 50% to 60% of the primary central nervous system tumors and is the most common intracranial malignancies.1In terms of current treatment methods,surgical treatment is the primary treatment for patients with glioma.Although most postoperative patients receive followup radiotherapy and chemotherapy,the recurrence rate is still high and the prognosis is poor.2,3
At present,gas gradually shows its enormous therapeutic potential in nervous system,4,5cardiovascular diseases6and cancers.7Anesthetic gases are administered as the primary therapy for sedation in the perioperative setting and critical care.Compared with current intravenous sedation agents,anesthetic gases-induced sedation may provide superior awakening and extubation times.Although they have been widely used,the mechanism by which they induce and maintain anesthesia has not been clarified.On the one hand,they can reduce presynaptic excitation and neurotransmitter release through inhibition of sodium (Na+) and several isoforms of calcium (Ca2+) voltage-gated channels; on the other hand,they also reduce neurotransmitter activity in the postsynaptic membrane by γ-aminobutyric acid,glycine,nicotinic acetylcholine,serotonin type 3,glutamate,N-methyl-D-aspartate,and α-amino-3-hydroxy-5-methyl-4-isoazolepropionic acid receptors.8,9
Numerous studies have found that anesthetic gases may influence tumor recurrence,metastasis,and long-term survival.10,11Due to the high degree of malignancy and recurrence rate of glioma,the application of anesthetics in glioma has also received more and more attention.In this article,we intend to summarize the previous studies and explain the effects of anesthetic gases on glioma,providing evidence for future gas therapy.
At present,sevoflurane and isoflurane are the two commonly used anesthetic gases in clinic.Due to research and space limitations,we only discuss the above two anesthetic gases in this review.
SEARcH STRATEGY
PubMed database was searched up to May 2019.The term“anesthetics”(including anesthetic gases,sevoflurane,or isoflurane) as a medical subject heading (MeSH) and key word,was combined with the term“glioma”as a medical subject heading (MeSH) and key word.
AnESTHETIcS GASES
Sevoflurane
Sevoflurane,a volatile anesthetic,is used to induce and maintain general anesthesia for outpatients and inpatients.12It has stable physical properties,rapid induction and minimal inhibitory effects on circulation.After being applied in more and more research,its special effects on cancer and tumors are discovered.For instance,it is well known that sevoflurane can play a protection for the lungs during surgery,and can also reduce the metastasis of cancer cells caused by surgery by promoting apoptosis of A549 cells (the human pulmonary adenocarcinoma cell line).10Fan et al.13have found that sevoflurane can reduce the metastasis and invasion of colorectal cancer cells.
Isoflurane
Isoflurane,a structural isomer to enflurane,is also a commonly used volatile anesthetic.But unlike enflurane,isoflurane carries a strong pungent odor that makes it difficult to use for inhalational induction of general anesthesia.14In addition to inducing anesthesia,isoflurane also shows the function of protecting organs from damage in hypoxic ischemic brain injury and myocardial ischemia-reperfusion injury.15,16The study has found that isoflurane can inhibit the expression of phosphatidylinositol 3-kinase and protein kinase B (AKT) and reduce the activity of nuclear factor kappa-B to inhibit the metastasis and invasion of liver cancer cells,and also can induce caspase 3 activation in cancer cells to induce apoptosis.17In addition,it also has a role in soft nest cancer18and lupus nephritis.19
EXPERIMEnTAL STUDIES Of AnESTHETIcS GASES In GLIOMA
It is well known that a treatment must be verified by large number of basic experiments before being applied to clinic.However,different studies may show different results.We collect several experiments related to gliomas and anesthetic gases and summarize the outcomes in this article (Table 1).Yi et al.20found that after sevoflurane treatment,the migration and invasion abilities of glioma cells were significantly reduced,17with increasing concentration.In another study,sevoflurane was found to inhibit the matrix metalloproteinase-2 (MMP-2) activity in glioma cells and reduced their metastasis and invasion.21Meuth et al.22and O’Leary et al.23found that isoflurane could promote the death of glioma cells.By comparing the effects of isoflurane,enflurane and sevoflurane on glioma cells,isoflurane is found to have the best anti-proliferative effect on C6 glioma,while sevoflurane has the worst.In addition to inhibition,some studies have the opposite conclusion.Shi et al.24found that sevoflurane promoted the production of hypoxia-inducible factors in a concentration-dependent manner and up-regulated the level of p-AKT,thereby promoting the proliferation of glioma stem cells.The same was true for isoflurane that exposure to isoflurane could promote the proliferation,survival and migration distance of human glioblastoma stem cells.25These conflicting results may be attributable to the heterogeneity of responses to the anesthetics gases depending on cell type,concentration,duration of exposure,or all.
cLInIcAL APPLIcATIOnS
Currently,most studies are limited to cellular levels.Although rats were used in one study,the anesthetic gas was not directly applied to rats with glioma.25Instead,the glioma cells were pretreated with anesthetic gas and injected into the right striatum to quantify the migratory potential capacity of cellsin vivo.The results showed that the migration ability of glioma stem cells pre-exposed to 1.2% isoflurane was significantly enhanced.In addition to ethical reasons,one important reason is that the research is not yet mature.First,there are many types of gliomas,and the characteristics of each are different.Therefore,different anesthetic gases may have different effects on different types of tumors.Secondly,the gas concentration,exposure time and adverse reactions are difficult to control.Therefore,further relevant research is needed.
MEcHAnISMS Of AnESTHETIcS GASES In GLIOMA
Metastasis and invasion are main causes of poor prognosis and relapse in patients suffering from glioma,and are receiving more and more attention in scientific and clinical research.26,27Anesthetics gases show an effective inhibitory effect on the survival,metastasis and invasion of glioma cells.However,due to the complexity of the processes,the molecular mechanisms have not been fully elucidated.
MicroRNAs (miRNAs) are a class of small noncoding RNAs with 21-25 nucleotides,which regulate the target gene expression by repressing translation or regulating mRNA degradation via binding to the 3′ untranslated region of their target genes.28They have important impacts on the progression of proliferation,migration and invasion.29-31A large number of studies have found that the effect of anesthetic gases on cancer cells is related to miRNAs.13,32And the same is true for gliomas.MiR-637 is considered to be an inhibitor of hepatocellular carcinoma and pancreatic cancer.33AKT is a target protein of miR-637,and AKT phosphorylation may promote tumor development and progression.34Compared to normal brain tissue,the level of miR-637 in glioma cells is low,and the combination of miR-637 and AKT is reduced in gliomas.35After treatment with sevoflurane,miR-637 is significantly up-regulated,and the expression and activity of AKT are also inhibited.20At the same time,metastasis and invasion of glioma cells are also inhibited.Emerging evidence has suggested that the pathogenesis of anesthetic gases on cancer cells is related to a group of miRNAs,not individual.Therefore,there may be more miRNAs involved.
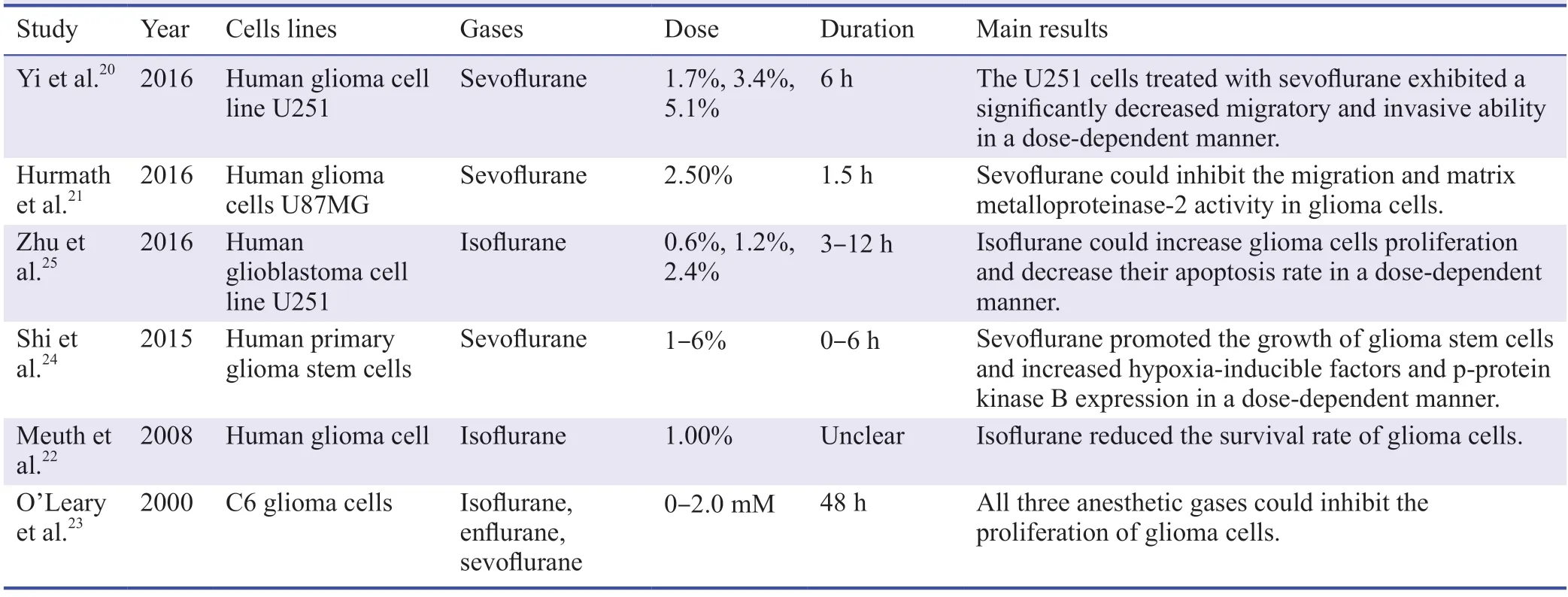
Table 1:The effects of aesthetic gases in glioma
Besides AKT,considerable evidence suggests that MMP-2 plays an important role in the metastasis and invasion of glioma cells.36In addition,MMP-2 is involved in the degradation of the blood-brain barrier,which will cause hematogenous metastases of cancer cells to form new cancer foci that cannot be distinguished by naked eye.37Therefore,the high expression of MMP-2 is an indication of poor prognosis.Moreover,there is also a close relationship between MMP-2 and AKT in gliomas.38Many substances can upregulate the expressions of MMP-2 through AKT signaling pathway in gliomas.39However,whether sevoflurane can affect the expression of MMP-2 through the AKT pathway needs further verification.
In addition to targeting proteins,anesthetic gases can also act on glioma cells by inhibiting the channel.40It is well known that ion channels are also involved in the migration and proliferation of tumor cells.41So they have been identified as promising therapeutic targets of brain tumor.One of the most important glioma-related channels is Ca2+-activated K+channels,being overexpressed in glioma patients.42,43Currently,there are some drugs targeting this channel for the treatment of gliomas.For example,Oxaliplatin,a third-generation organoplatinum,can suppress the amplitude of glioma cell K+currents by inhibiting Ca2+-activated K+channels,thereby affecting cell activity.
The above mechanism is mainly to explain the beneficial aspects of anesthetic gases,while one study has found that anesthetic gas can stimulate the proliferation of glial stem cells by up-regulating the expression of AKT.24,25And in addition to glioma,the effect on other tumors is not consistent.Therefore,the mechanism of anesthetic gases on glioma requires more types,more rigorous and more detailed research.
cOncLUSIOn
Although anesthetic gases have been used for decades,most of them are used as anesthesia inducers.So far,most of the experiments on gliomas are limited to the cell stage,and the application to the living body has not been reported.Anesthetics may have side effects on brain function due to its toxicity.44-46For example,it may cause apoptosis of normal nerve cells and affect the learning and behavior of humans and animals.14Therefore,there are still great challenges in the application of living organisms.As far as current research is concerned,different anesthetic gases have different effects on different types of glioma cells.
Moreover,there is also no consensus on the optimal concentration of the application.Clinically,the choice of anesthetic dose is based on the minimum alveolar concentration.It is defined as the concentration of inhaled anesthetic within the alveoli at which 50% of people do not move in response to a surgical stimulus.Many variables can alter minimum alveolar concentration,such as age,temperature and pregnancy.47-49Therefore,the minimum alveolar concentration should be monitored and adjusted to the appropriate range during sedation.Since most of the current studies are still limited to the cellular level rather than the living body,a fixed concentration is given,which leads to differences in the dose of intervention and application in clinic.
Therefore,whetherin vitroorin vivo,research will continue.Through the above introduction,anesthetic gas may become an emerging treatment of glioma.Although there are still many questions and problems at present,one day it will come to a conclusion.
Author contributions
Manuscript writing:XC; manuscript revision:YGM; review design:ZQY,JW,GC.All the authors read and approved the final version of the manuscript for publication.
conflicts of interest
The authors have no conflicts of interest to declare.
financial support
None.
copyright license agreement
The Copyright License Agreement has been signed by all authors before publication.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal,and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License,which allows others to remix,tweak,and build upon the work non-commercially,as long as appropriate credit is given and the new creations are licensed under the identical terms.
- Medical Gas Research的其它文章
- Respiratory gas conditioning with filters/heat and moisture exchangers can increase the duration of hyperthermia in patients under mechanical ventilation
- Correction:Retraction:A survey of anaphylaxis etiology and treatment
- Ozonated oil in wound healing:what has already been proven?
- Cardiac function dependence on carbon monoxide
- Neurocognitive sequelae after carbon monoxide poisoning and hyperbaric oxygen therapy
- A“philosophical molecule,”hydrogen may overcome senescence and intractable diseases