
Pediatric non-alcoholic fatty liver disease and kidney function: Effect of HSD17B13 variant
2020-10-22 04:31:52AnnaDiSessaGiuseppinaRosariaUmanoGraziaCirilloAntonioParidePassaroValentinaVerdeDomenicoCozzolinoStefanoGuarinoPierluigiMarzuilloEmanueleMiragliadelGiudice
World Journal of Gastroenterology 2020年36期
Anna Di Sessa, Giuseppina Rosaria Umano, Grazia Cirillo, Antonio Paride Passaro, Valentina Verde, Domenico Cozzolino, Stefano Guarino, Pierluigi Marzuillo, Emanuele Miraglia del Giudice
Abstract
Key Words: Hydroxysteroid; Dehydrogenase; Fatty; Liver; Renal; Function; Obese; Children
INTRODUCTION
Non-alcoholic fatty liver disease (NAFLD) and chronic kidney disease (CKD) represent worldwide public health concerns affecting up to 25%-30% and up to 10%-15% of the general population, respectively[1]. Both diseases are progressive chronic conditions representing a spectrum of diseases ranging from mild to severe disease with end-stage organ injury and sharing several pathogenic factors[1,2].In childhood, NAFLD has been recognized as the most common chronic liver disease, with a prevalence of 8% in the general pediatric population and up to 34.2% among obese children[3].To date, several studies demonstrated that NAFLD has been associated with increased prevalence of chronic kidney disease CKD (defined as sustained reduction in estimated glomerular filtration rate (eGFR) or evidence of structural or functional abnormalities of the kidneys on urinalysis, imaging or biopsy)[1,2,4,5]. In addition, it has been also showed that renal impairment obesity-related might occur already in childhood with a potential genetic influence[6-8].Recent data added novel pieces in the knowledge of the intriguing link between NAFLD and renal function[1,9,10]. Compelling evidence showed that the major genetic NAFLD risk factors such as the I148M polymorphism in thepatatin like phospholipasecontaining domain 3(PNPLA3)and the E167K allele in thetransmembrane 6 superfamily member 2 (TM6SF2)gene exert an effect on estimated glomerular filtration rate (eGFR) both in adults and children[1,5,9-12]. In particular, our group previously showed that children with obesity and homozygous forPNPLA3rare allele had lower eGFR levels compared to other genotypes both among patients with and without NAFLD, with a major effect of this polymorphism in NAFLD context[10]. In addition, we demonstrated that obese children carrying theTM6SF2E167K allele showed higher eGFR levels compared with the homozygous subjects for theTM6SF2E167 allele, irrespective of presence of NAFLD[9].
In the NAFLD susceptibility gene variants scenario, the role of the hepatic lipid droplet proteinhydroxysteroid 17-beta dehydrogenase 13(HSD17B13) gene in NAFLD has been recently studied[3,13,14]. A growing body of evidence shows the role of the rs72613567HSD17B13polymorphism in protecting against liver damage both in adults and children[3,13-15]. This variant represents a splice region characterized by an adenine (A) insertion in the coding region adjacent to the donor splice site of exon 6, leading to a frame-shift and premature truncation of HSD17B13 protein[3].
To date, there are no studies evaluating the effect of the rs72613567HSD17B13polymorphism on eGFR in obese children and adolescents. Considering the evidence of the data both in adulthood and childhood supporting a genetic link between NAFLD and CKD[5,8-11], we hypothesized that this variant, as demonstrated on NAFLD, could show the same protective effect on renal function in obese children and adolescents. We aimed to investigate the role of the rs72613567HSD17B13polymorphism on eGFR levels in obese children with and without NAFLD and without known primary kidney disease.
MATERIALS AND METHODS
Study population
We recruited 684 obese children consecutively attending our Obesity Clinic from February 1, 2017 to January 31, 2019. Both Body Mass Index (BMI) > 95thpercentile according to reference values and normal renal function (eGFR > 90 mL/min/1.73 m2)[6,16]were considered as inclusion criteria. Secondary forms of NAFLD or obesity, consumption of medications, eGFR < 90 mL/min/1.73 m2, presence of proteinuria or hematuria at urine dipstick on urine samples[17], missing eGFR levels, or denied consent for diagnostic procedures represented exclusion criteria. Patients presenting possible signs of underlining primary kidney disease (decreased eGFR and proteinuria/hematuria) were also excluded to avoid potential affection of our analysis. The ethical committee of University of Study of Campania “Luigi Vanvitelli” approved the study. A written informed consent was obtained before any procedure. Clinical parameters including pubertal stage and blood pressure were obtained as described[18]. Evaluation of patients’ growth charts was made to calculate duration of obesity.
Laboratory and ultrasound evaluation
Biochemical parameters were assayed and homeostasis model assessment (HOMA-IR) calculated[18]. Alanine transaminase (ALT) levels greater than 40 IU/L were considered as elevated. The Jaffè method was used to serum creatinine (mg/dL) measurement and the eGFR was calculated through the Schwartz equation[6,19]. The eGFR to the ideal body weight-derived body surface area was normalized.
A trained radiologist performed liver ultrasound imaging in order to detect the presence of steatosis. Liver steatosis was assessed as present or absent given the abnormally intense, high-level echoes arising from the hepatic parenchyma and liver–kidney differences in echo amplitude. NAFLD was defined by the presence of ultrasound detected liver steatosis and/or ALT levels > 40 IU/L.
Genotyping
At diagnosis, informed consent was collected for DNA extraction from peripheral whole blood.
Genomic DNA was extracted from peripheral whole blood with a DNA extraction kit (Promega, Madison WI, United States). All recruited subjects were genotyped for the single nucleotide polymorphism (SNP) rs72613567: TA allele of theHSD17B13gene using a TaqMan allelic discrimination custom assay (ID: ANNKVTJ) (Applied Biosystems, United States) on ABI 7900HT Real Time PCR system. Patients were also genotyped forPNPLA3I48M andTM6SF2E167K polymorphisms[3].
Statistical analysis
A Chi Square test was used to verify whether the genotypes were in Hardy-Weinberg equilibrium and to compare categorical variables. We classified the population according to the presence/absence of NAFLD and we compared eGFR levels in these two groups (with and without NAFLD) on the basis ofHSD17B13polymorphism.
Differences for continuous variables were analyzed using ANOVA if normally distributed, or the Kruskal-Wallis test if non-normally distributed. Not-normally distributed variables were log-transformed before the analysis, but raw means are shown.
The genotype was coded with an additive model of inheritance. It was coded 0 or 1 corresponding to the subjects homozygous for the wild type allele and carrying the A rare allele, respectively.
A general linear model (GLM) for eGFR variance including gender, duration of obesity,HSD17B13, PNPLA3, andTM6SF2genotypes, BMI-SDS, HOMA, LDL, and triglycerides was made both in patients with and without NAFLD. The non-normally distributed variables were log transformed for this analysis.
A comparison of regression lines by ANOVA was performed to examine the influence ofHSD17B13genotype on the relationship between eGFR and age both among patients with and without NAFLD.
The IBM SPSS Statistics software, Version 24 (IBM, Armonk, NY, United States) was used for all statistical analyses with the exception of the comparison of regression lines made by Stat-Graph XVII software for Windows. Data were expressed as means ± SD.P-values less than 0.05 were considered statistically significant.
RESULTS
We enrolled 684 obese patients with mean age of 10.56 ± 2.94 years and mean BMI-SDS of 2.98 ± 0.78. The frequency of theHSD17B13polymorphism distribution was in Hardy Weinberg equilibrium (P> 0.05).
Patients carrying theHSD17B13rare A allele showed higher eGFR levels compared with homozygous patients both among subjects with and without NAFLD (Table 1 and 2). As expected, ALT and aspartate transaminase (AST) levels were significantly lower in subjects carrying theHSD17B13rare A allele in both groups (Table 1 and 2). A general linear model for eGFR variance including gender, duration of obesity,HSD17B13,PNPLA3, andTM6SF2genotypes, BMI-SDS, HOMA, ALT and triglycerides confirmed a direct and significant association of eGFR values withHSD17B13genotype both in patients with and without NAFLD (Table 3).
A comparison of regression line slopes was performed to examine the influence ofHSD17B13genotype on the relationship between eGFR and age both among patients with and without NAFLD.Homozygous patients forHSD17B13genotype with NAFLD showed a significantly higher decline of eGFR with the increase of the age compared with the patients with NAFLD carrying theHSD17B13rare A allele (Pvalue for intercepts = 0.005;Pvalue for slopes = 0.94) (Figure 1). We also confirmed this effect among patients without NAFLD (Pvalue for intercepts = 0.0012;Pvalue for slopes = 0.87) (Figure 2).
DISCUSSION
The novel finding of our study was the association between thers72613567 HSD17B13polymorphism and higher eGFR levels in obese children and adolescents without evidence of primary kidney disease. We confirmed these results both in patients with and without NAFLD and independently of rs738409PNPLA3andTM6SF6E167K polymorphisms. Notably, carriers of theHSD17B13rare A allele both with and without NAFLD maintained significant higher eGFR levels increasing the age. Taken together, these results corroborate the protective role of theHSD17B13gene in both NAFLD and CKD.
Emerging evidence suggests a potential influence of the major NAFLD susceptibility gene variants such asPNPLA3 I148MandTM6SF2167K on CKD[9,10]. In fact, previous studies showed that both in adults and children with and without NAFLD thePNPLA3 I148Mvariant was associated with lower eGFR levels[1,5,10,11]. Interestingly, thePNPLA3GG genotype was associated not only with higher risk of early glomerular injury but also tubular damage in NAFLD patients with persistentlynormal ALT levels[12]. Further researches investigating the role of theTM6SF2167K allele on renal function showed a protective role of this variant on eGFR both in adults and children also regardless the presence of NAFLD[5,8,9].
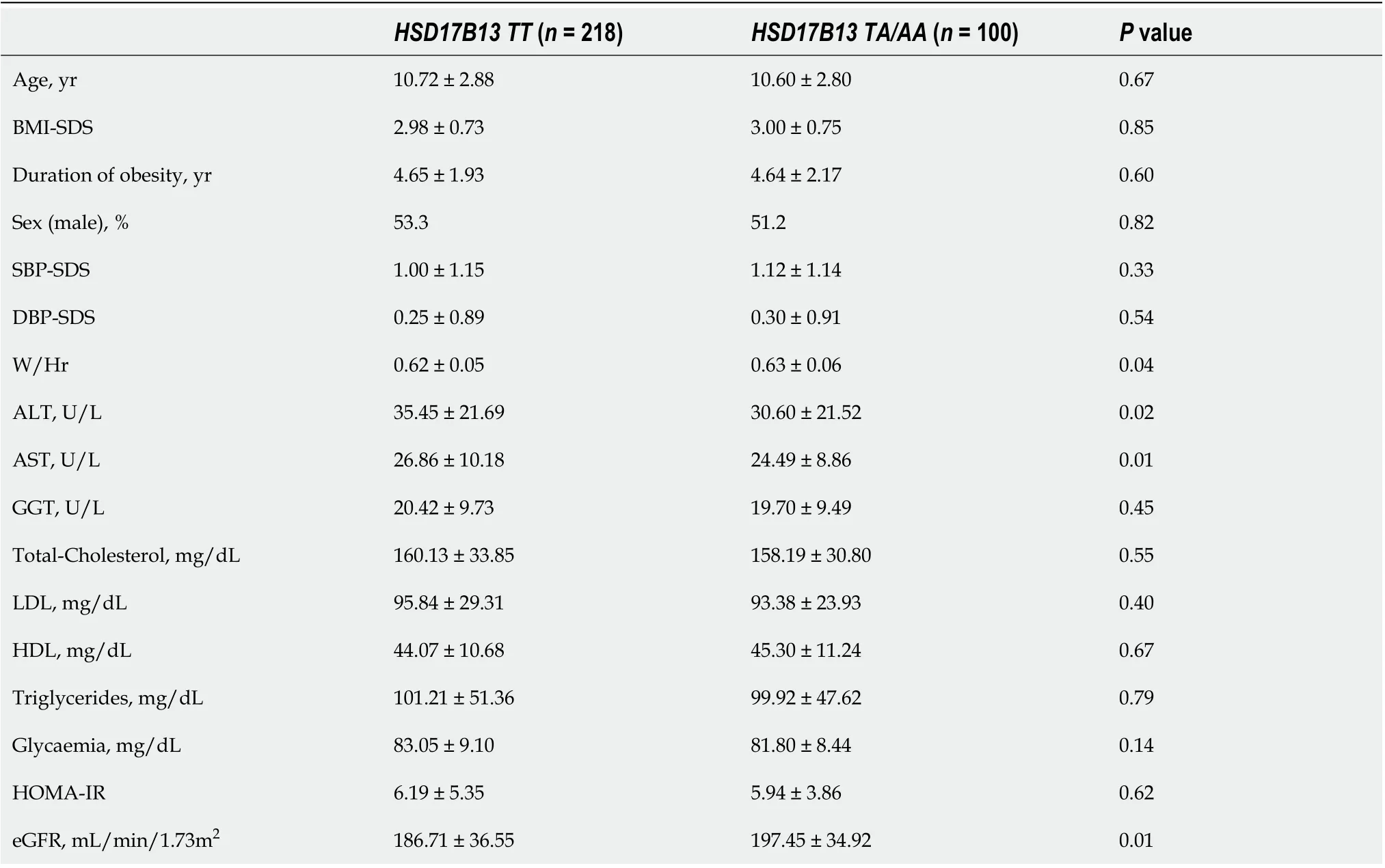
Table 1 Main features in patients with non-alcoholic fatty liver disease according to HSD17B13 genotypes
TheHSD17B13gene encodes the hepatic lipid droplet protein hydroxyl-steroid 17-beta dehydrogenase 13, an uncharacterized member of the hydroxysteroid 17-beta dehydrogenase family involved in sex hormone and mainly in fatty acid metabolism[13]. The rs72613567 HSD17B13 splice variant alters m-RNA splicing resulting in a truncated protein with reduced enzymatic activity against several proinflammatory lipid species[13,14]. The mechanism linking HSD17B13 to liver disease is not referred to hepatic fat accumulation, but directly involves modulation of inflammation and fibrogenesis through an involvement in retinol metabolism[20]. Taken together, these findings support the beneficial influence of thisloss-of-functionagainst risk of chronic liver disease and hepatocellular carcinoma as well[14,20].
To date, the exact pathophysiologic function remains still poorly elucidated, but the protective role of thers72613567HSD17B13 variant in NAFLD development and progression has been confirmed both in adults and children[3,13,15]. As observed in the liver context, we could speculate that thers72613567HSD17B13 variant might exert a “protective” role on renal function through its role in retinol metabolism by modulating both inflammation and fibrogenesis
Recent data showed a significant association between NAFLD and the long-term risk of incident CKD[1,2]. Moreover, it should be noted that NAFLD is closely linked to an increased risk of cardiovascular disease (CVD), independent of the coexistence of common cardiometabolic risk factors[21]. In addition, it has been well established that CKD represents a major risk factor for end-stage renal disease, CVD and premature death[2]. Despite several newer hypotheses (including gut microbiota, platelet activation, and dietary changes) the major pathogenic link underlying these chronic diseases is represented by the activation of the shared proinflammatory and profibrotic factors[1]. In this context, the role of theHSD17B13gene in retinol metabolism leading to lack of hepatic stellate cells activation might contribute to explain its protective effect on renal function[3]. Given that, this intriguing “vicious circle” among NAFLD, CVD and CKD represents a challenging field for clinicians thatshould be carefully evaluated. In fact, these findings emphasize the importance of an early detection of NAFLD diagnosis in order to potentially counteract the risk of both CKD and CVD. Beyond the established contribute in identifying subjects with greater susceptibility to NAFLD, a better NAFLD genetic characterization might be also helpful to individuate patients with NAFLD who may be at higher risk of chronic diseases such as CKD and CVD.
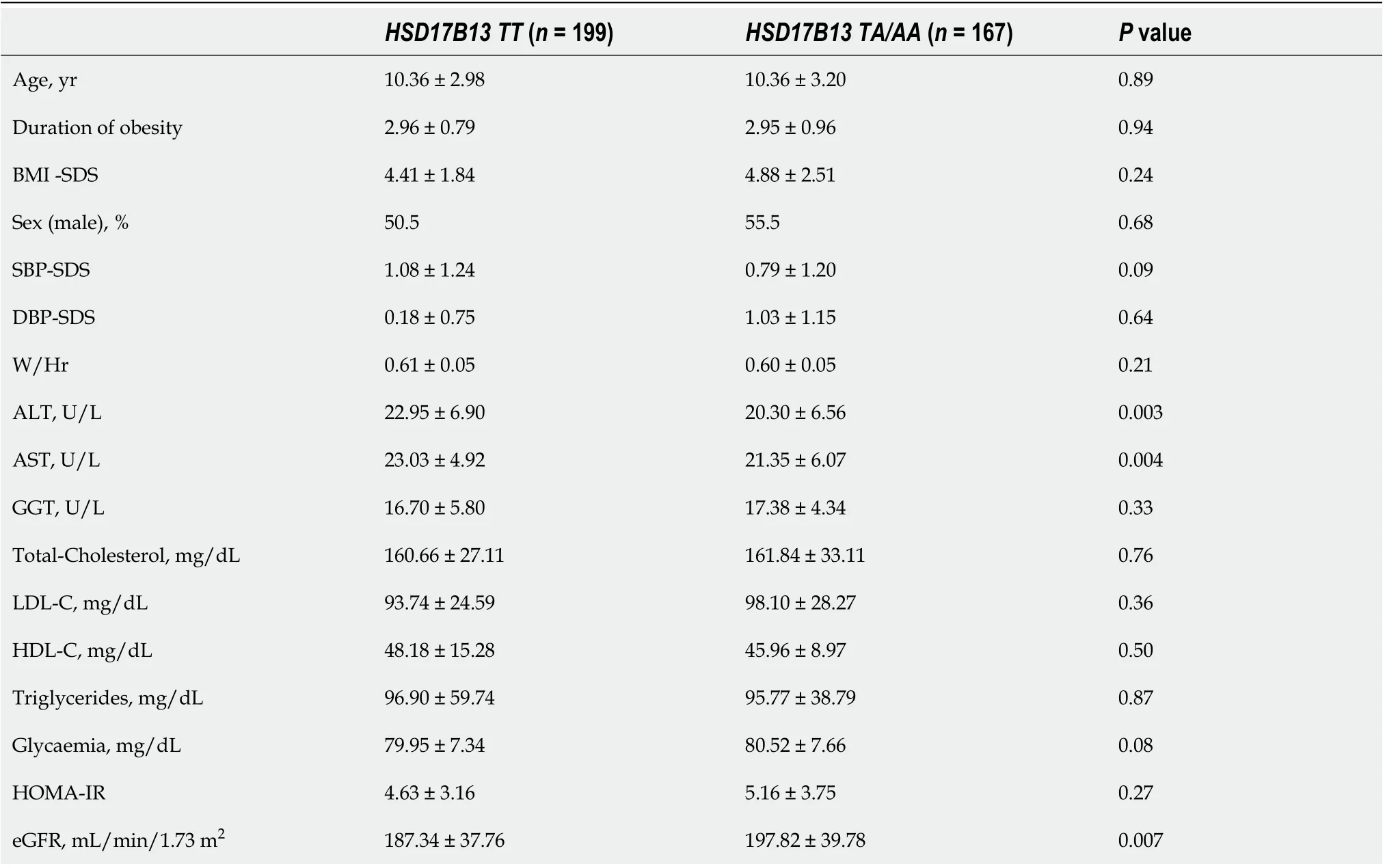
Table 2 Main features in patients without non-alcoholic fatty liver disease according to HSD17B13 genotypes
Our study has some limitations that deserve mention. First, there is a lack of a more accurate method to measure glomerular filtration rate (i.e., by cystatin C). NAFLD diagnosis has been performed by ultrasound and ALT levels and not by liver biopsy or magnetic resonance. Moreover, this is only a pathophysiological study evaluating only children with normal renal function, and as future perspective could be interesting to evaluate the effect of thers72613567 HSD17B13polymorphism on proteinuria.
CONCLUSION
In conclusion, for the first time in literature, we showed that thers72613567 HSD17B13polymorphism is associated with higher eGFR levels in obese children. This effect on renal function is confirmed in patients with and without NAFLD and independently ofPNPLA3I148M andTM6SF6E167K polymorphisms. Of note, this variant exerts a protective role against renal function decline increasing the age both in patients with and without NAFLD. Given these results, we added to the existing knowledge of the role of genetics on the association between NAFLD and renal function already in childhood. Collectively, these findings might also have significant clinical implications in improving both prevention and treatment strategies of obese patients with NAFLD.
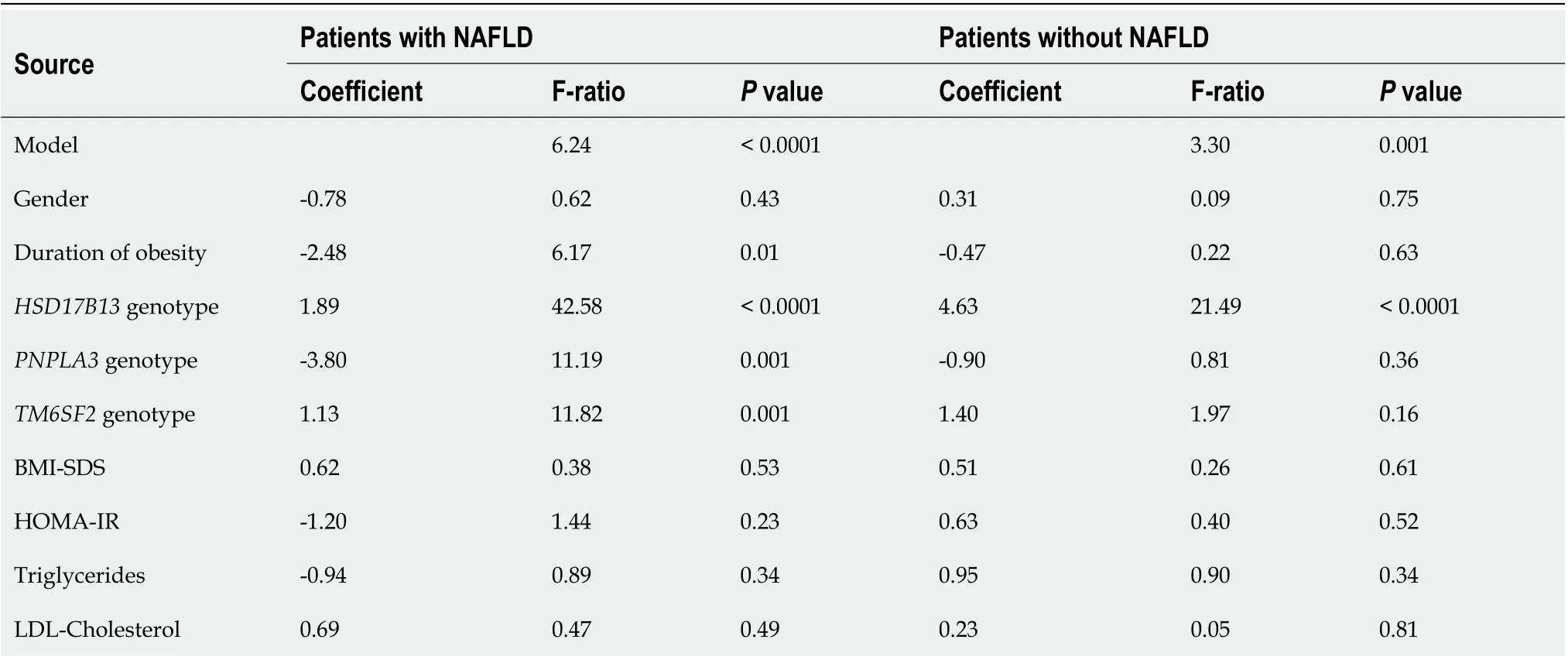
Table 3 General linear model for analysis of variance of estimated glomerular filtration rate both among patients with and without nonalcoholic fatty liver disease
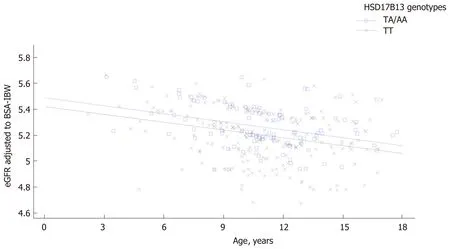
Figure 1 Regression analysis describing the relationship between estimated glomerular filtration rate and age according to HSD17B13 genotype in patients with non-alcoholic fatty liver disease. The regression is described by the equation y = 5.49596 – 0.0205849x – 0.0688943 × (hsd17b13 = 1) + 0.00054199x × (hsd17b13 = 1). P value for intercepts is 0.005 while for slopes is 0.94.
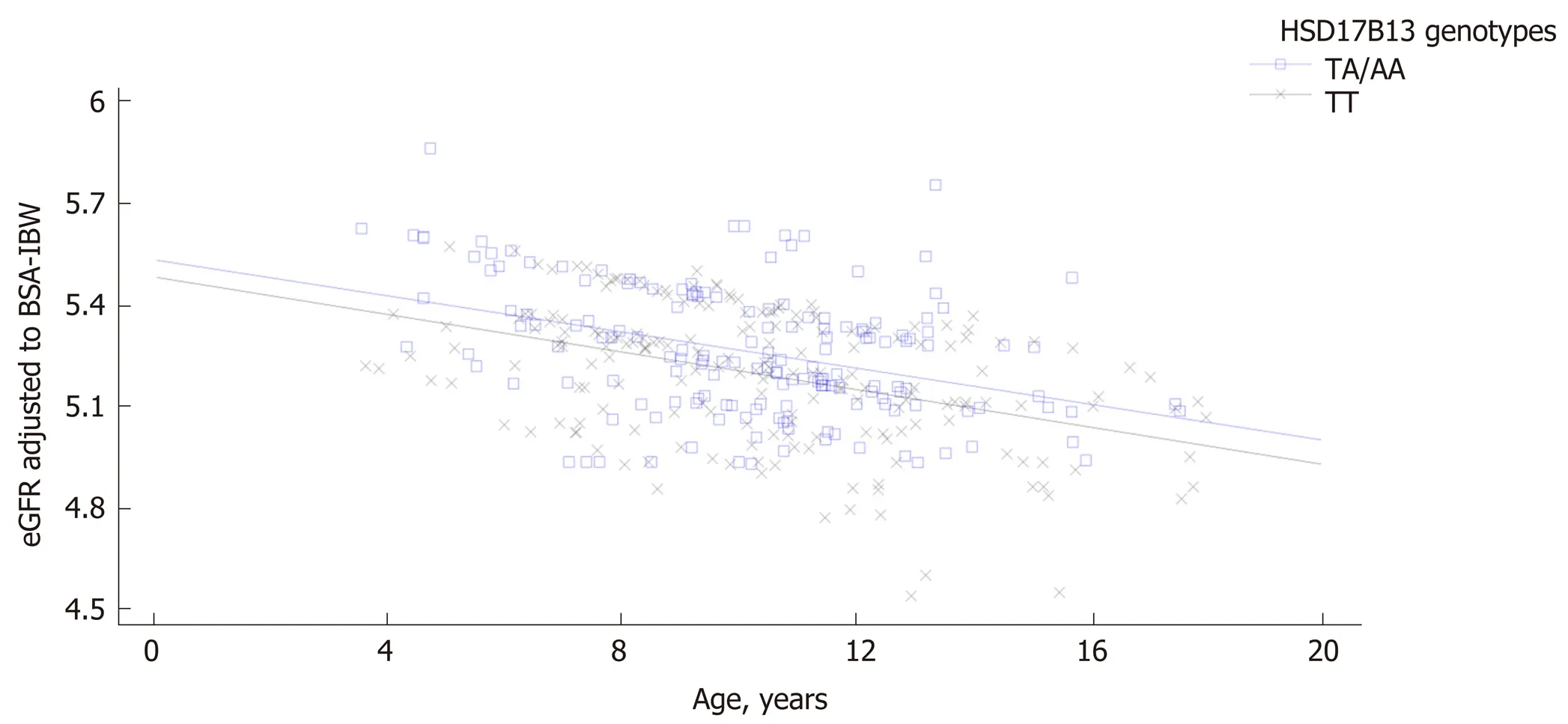
Figure 2 Regression analysis describing the relationship between estimated glomerular filtration rate and age according to HSD17B13 genotype in patients without non-alcoholic fatty liver disease. The regression is described by the equation y = 5.54093 – 0.0266856x – 0.0508993 × (hsd17b13=1) – 0.00105742x × (hsd17b13=1). P value for intercepts is 0.0012 while for slopes is 0.87.
ARTICLE HIGHLIGHTS
Research background
Accumulating data supports a genetic link between non-alcoholic fatty liver disease (NAFLD) and chronic kidney disease (CKD), mostly sustained by both the major NAFLD risk polymorphisms such as the I148M polymorphism in thepatatin like phospholipase containing domain 3(PNPLA3) and the E167K allele in thetransmembrane 6 superfamily member 2gene (TM6SF2). Recently thehydroxysteroid 17-beta dehydrogenase 13(HSD17B13) gene has been recognized as a novel genetic variant involved in NAFLD pathophysiology with a protective role against liver damage both in adults and children.
Research motivation
Despite a growing interest regarding the potential genetic link between NAFLD and CKD, available literature data showed no studies investigating the effect of thers72613567:TAvariant of theHSD17B13gene on estimated glomerular filtration rate (eGFR) in obese children.
Research objectives
In this study we aimed to evaluate the impact of thers72613567:TAvariant of theHSD17B13gene on estimated glomerular filtration rate (eGFR) in obese children.
Research methods
Anthropometric, laboratory, and instrumental evaluations were conducted in all the enrolled 684 obese children. NAFLD was defined by ultrasound detected liver steatosis and/or alanine aminotransferase (ALT) levels > 40 IU/L. Genotyping for thers72613567:TAvariant of theHSD17B13gene in all the enrolled subjects was also performed.
Research results
Patients carrying theHSD17B13rare A allele had higher eGFR levels than homozygous patients both among subjects with and without NAFLD. This association was independent ofPNPLA3andTM6SF2polymorphisms both in patients with and without NAFLD. The eGFR decline in homozygous subjects forHSD17B13genotype with and without NAFLD was more markedly with the increase of the age than in carriers theHSD17B13rare A allele.
Research conclusions
In line with the beneficial effect against NAFLD risk, thers72613567:TAvariant of theHSD17B13gene exerts a protective role also on renal function in obese children with and without NAFLD and independently ofPNPLA3 I148MandTM6SF6E167K polymorphisms.
Research perspectives
Findings from this study highlight the importance of a better NAFLD genetic assessment as possible clinical tool for improved strategies to identify patients at higher cardiometabolic risk already in childhood.
ACKNOWLEDGEMENTS
The authors are grateful to the patients and their families.
 World Journal of Gastroenterology2020年36期
World Journal of Gastroenterology2020年36期
- World Journal of Gastroenterology的其它文章
- Major gastrointestinal bleeding and antithrombotics: Characteristics and management
- Artificial intelligence in gastric cancer: Application and future perspectives
- Treatment of eosinophlic esophagitis with swallowed topical corticosteroids
- Granulocyte-macrophage colony-stimulating factor protects mice against hepatocellular carcinoma by ameliorating intestinal dysbiosis and attenuating inflammation
- SMARCB1/INI1-deficient pancreatic undifferentiated rhabdoid carcinoma mimicking solid pseudopapillary neoplasm: A case report and review of the literature
- Solitary peritoneal metastasis of gastrointestinal stromal tumor: A case report