
Quantitative Microbial Risk Assessment of Cryptosporidium and Giardia in Public Drinking Water in China*
2021-07-14 01:43:38CAOShengKuiJIANGYanYanYUANZhongYingYINJianHaiXUMengXUEJingBoTANGLinHuaSHENYuJuanandCAOJianPing
CAO Sheng Kui , JIANG Yan Yan , YUAN Zhong Ying , YIN Jian Hai , XU Meng ,XUE Jing Bo , TANG Lin Hua, SHEN Yu Juan,5,#, and CAO Jian Ping,5,#
Key words:Cryptosporidium;Giardia;Quantitative microbial risk assessment
Cryptosporidiumspp. andGiardiaspp. are important intestinal protozoa of humans and animals,causing severe diarrhea.To date,many outbreaks have been caused by both pathogens[1],most notably the massive waterborneCryptosporidiumoutbreak in Milwaukee,Wisconsin in 1993,which caused 400,000 infections and approximately 100 deaths.Fecal-oral transmission ofCryptosporidiumoocysts andGiardiacysts occurs through the consumption of contaminated drinking or recreational water or food or contact with infected people or animals.Risk assessments forCryptosporidiumandGiardiain bodies of water have become crucial tools in many countries to help public health practitioners make appropriate environmental decisions for the maintenance of public health.For example,the daily consumption of drinking water was identified as an important contributing factor for the high risk ofCryptosporidiumandGiardiainfections in Mexico[2].As recommended by the World Health Organization(WHO),quantitative microbial risk assessment(QMRA) permits the evaluation of the risk of infection by biological agents through data monitoring in the laboratory.The process includes four steps: hazard identification,exposure assessment,dose-response modeling,and risk characterization.ForCryptosporidiumandGiardia,the risks for individuals should be less than 10-4infections per year,according to the United States Environmental Protection Agency (USEPA).Furthermore,the acceptable threshold for disease burden from waterborne exposure has been set at 10-6disability-adjusted life years (DALYs) per person per year (pppy) by WHO,which is approximately equivalent to a 10-5excess lifetime risk of cancer(i.e.,1 excess case of cancer per 100,000 people ingesting drinking water at the water quality target,daily over a 70-year period).
Epidemiological data on human cryptosporidiosis and giardiasis have confirmed that these organisms are ubiquitous in China.For example,the occurrence rates were found to be 2.0% forCryptosporidiumand 1.4% forGiardiain children with a history of diarrhea in Wuhan,Hubei Province[3].However,the routes ofCryptosporidiumandGiardiainfections have received little attention.A series of outbreaks have been associated with the presence of both protozoa in surface water,and most of these have occurred in developed countries[1].Water is a significant route of transmission for both protozoa,which should be of great concern,especially in bodies of water used for the production of domestic drinking water and recreational activities.
The objective of this study was to determine the prevalence of both protozoa in source water and treated drinking water of waterworks in three densely populated countryside regions: Jintan,Jiangsu Province (eastern China);Ezhou,Hubei Province (central China);and Binyang,Guangxi Zhuang Autonomous Region (southern China).Based on the survey data,the risks of protozoan infection and disease burdens were assessed for the populations supplied by these drinking water samples,taking into account the water consumption habits of the Chinese population and two subpopulations with different immune statuses.Our study may be the first QMRA ofCryptosporidiumandGiardiain these regions,which will be helpful in prompting actions to reduce the disease burden of protozoan infections in China.
Cryptosporidiumoocysts andGiardiacysts are highly resistant to chemical disinfection and environmental stressors,and may survive for a long period of time in water.They cannot be completely inactivated by conventional waterwork treatment methods (comprising coagulation,flocculation,sedimentation,sand filtration,chlorination,and fluoridation),thus affecting the health of surrounding residents. In the regions we investigated,the waterworks were the sole source of drinking water for surrounding residents and they used conventional water treatment practices.Consequently,CryptosporidiumandGiardiawere considered to pose a threat to local residents.
Samples were collected from Jintan District,Ezhou City,and Binyang County in China from June to December 2014,which included both the rainy and dry seasons.Five different waterwork facilities were sampled in each region,and at each sampling site,three parallel water samples were collected at different times.The volume of each sample was 10 and 100 L for source and treated water,respectively.All samples were flocculated and filtered within 24 hours of sampling.Clean polypropylene containers(15 L) were used for the collection of source water,which was collected from approximately 10-20 cm below the surface of the surface water sites,e.g.,a river or lake.Treated water samples were collected directly through taps in the waterwork facilities.
The detection of (oo)cysts has been described elsewhere.Each source water sample was processed using the calcium carbonate flocculation (CCF)modified Method 1623[4].The number of (oo)cysts was recorded as the detected number in 10 L of source water.Each treated water sample was concentrated on site using a 3.0-μm pore-size cellulose acetate membrane modified Method 1623[5].The number of (oo)cysts was recorded as the detected number in 100 L of treated water.Simultaneously,the recovery efficiencies (R) forCryptosporidiumandGiardiawere evaluated using seeded water containing 99 ± 1.1 oocysts and 99 ±1.5 cysts (EasySeed,ESCG100-5;BioPoint,Sydney,Australia) in purified water samples.TheRvalue was expressed as a percentage and was calculated as follows:

whereCiis the initial known concentration of(oo)cysts in the seeded water,andCis the detected concentration of (oo)cysts.The concentrations and the recovery efficiencies ofCryptosporidiumandGiardiaare presented as the arithmetic mean ±standard deviation (s).
In consideration of the habits and customs of local residents and the coverage of sampling sites,the exposure was evaluated based the entire local resident population.Exposure to source and treated water was estimated using two different approaches.
For source water,exposure (Ns) was calculated using the following Equation[6]:

whereNsis the exposure of individuals to (oo)cysts;Cis the mean detected concentration of (oo)cysts[(oo)cysts/L];Ris the recovery efficiency of the CCFmodified Method 1623;Iis the fraction of infective protozoa [assuming that all (oo)cysts were viable and infectious];Vis the daily consumption of unboiled water by individuals,which was considered to include two main exposure routes: direct consumption of tap water and the intake of residual water during tooth-brushing or washing.The mean ingestion volume of unboiled tap water was approximately 21 mL/day and the residual water remaining in the mouth after tooth-brushing or washing has been estimated to be approximately 7-71 mL/day for Chinese individuals[5].TRis the removal efficiency of (oo)cysts by the waterwork facility,which was inferred to approximately 2 log10and 3 log10units for oocysts and cysts,respectively,when using conventional treatment methods.
For treated water,the exposure (Nt) was calculated using the following Equation[2]:

whereNt,C,R,I,andVare the same as those used for the source water calculation andRis the recovery efficiency of membrane-modified Method 1623.
The probability of infection by (oo)cyst ingestion was determined using the exponential doseresponse model.
The daily risk of infection (Pd) for individuals was estimated using the following Equation:

whererrepresents infectivity constants of 0.09 forCryptosporidium[7]and 0.0199 forGiardia[2].
The annual risk of infection (Py) for individuals was estimated using the following Equation:

wherenis the number of days for an individual exposed to the pathogens per year.In these regions,the investigated waterwork facilities were the sole local water sources,and thus,nwas assumed to be 365 days.
The risk was characterized by calculating DALYs,which represents disease burden and includes the years of life lost due to mortality and the loss of healthy years due to disability.In consideration of different disease burdens in different individuals,two subgroups were evaluated:immunocompetent(99.945%) and immunodeficient individuals(0.055%)[8]. Disease burdens associated withCryptosporidiumandGiardiafor the entire population were calculated as follows[8]:

wherePillyearis the annual probability of illness for the population;Pill/Infis the probability of developing an illness after being infected,i.e.,morbidity,which is 0.39 for the immunocompetent population and 1 for the immunodeficient population forCryptosporidiuminfection[9]and 0.5 forGiardiainfection[8];?is the susceptibility fraction of the total population,which is considered to be 100% here because tap water and residual water from toothbrushing or washing affect all individuals;Bis the disease burden;iis the population subgroup number;DBPCiis the disease burden per case in theith subgroup,which was estimated to be 0.32 DALYs and 1.91 × 10-3DALYs per case for the immunodeficient and immunocompetent population,respectively,due to cryptosporidiosis,and 1.7 × 10-3DALYs per case due to giardiasis in China[8];andPiis the proportion of theith subgroup in the total population,as previously mentioned.
In total,45 source water samples and 45 treated water samples from 15 different waterworks were collected and examined forCryptosporidiumandGiardiausing CCF-modified Method 1623 and membrane-modified Method 1623,respectively.The mean concentrations in each region are shown in Table 1.For source water,4Cryptosporidiumpositive samples (mean concentration:0.020-0.033 oocysts/L) and 3Giardia-positive samples (mean concentration:0-0.033 cysts/L) were found.For treated water,1Cryptosporidium-positive sample(mean concentration:0-0.013 oocysts/L) and 2Giardia-positive samples (mean concentration:0-0.0013 cysts/L) were found.In a real waterwork treatment system,the water samples taken before and after the treatment zone are almost unpaired because of a time delay during the water treatment process,i.e.,they are not exactly the same water sample. Meanwhile,the occurrence of both protozoa in environmental water samples is influenced by many factors,including the timing and frequency of sampling and the sampling site characteristics (e.g.,rainfall or distance from pathogen sources).This resulted in inconsistencies in concentrations between source water and treated water samples collected from the same region.Furthermore,a large number of samples are needed to achieve consistent results due to the low density,motility,and variability of both protozoa.
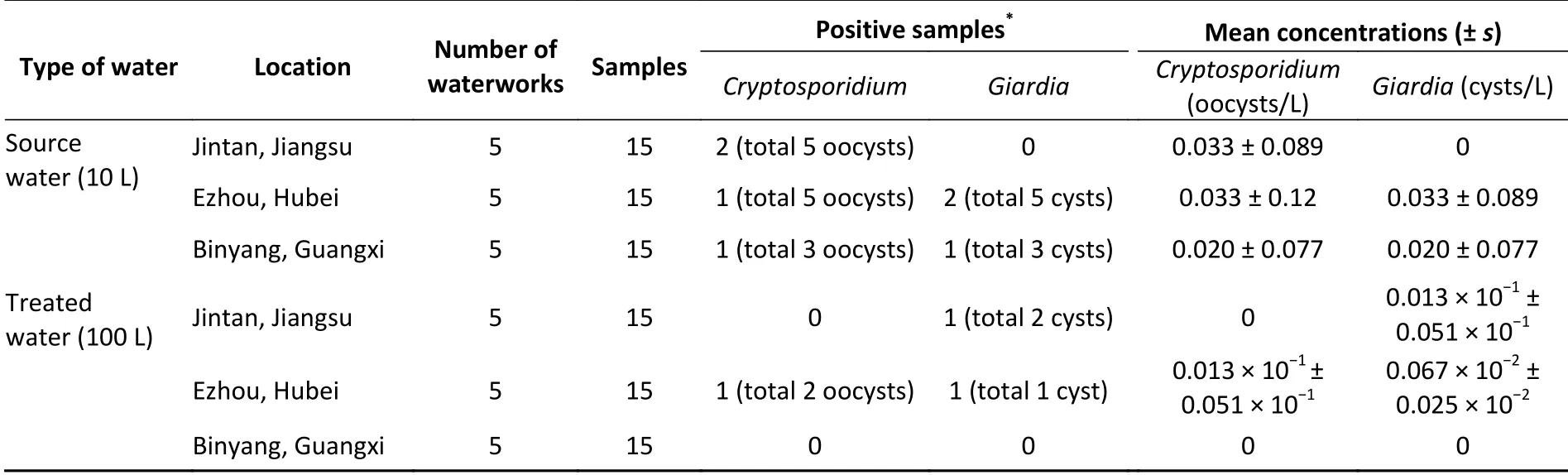
Table 1. Occurrence of Cryptosporidium and Giardia in source and treated water samples from three regions in China
The recovery efficiencies forCryptosporidiumandGiardiafrom source water samples were 48.5%± 0.5% and 52.5% ± 0.8% using CCF-modified Method 1623,respectively,and from treated water samples,the recovery efficiencies were 35.4% ±0.4% and 37.4% ± 0.6% using membrane-modified Method 1623,respectively.All of these recovery efficiencies met the acceptable level described in Method 1623 (24%-100%).
People living in Jintan,Ezhou,and Binyang were exposed to 0-6.26 × 10-5,1.91 × 10-5-3.38 × 10-4,and 0-3.79 × 10-5oocysts and 0-3.20 × 10-4,1.76 ×10-6-1.65 × 10-4,and 0-3.50 × 10-6cysts per day,in the best and worst exposure scenarios based on water consumption,respectively.These data were obtained from the integration of calculated results,including source and treated water samples.The annual probability of infection and DALYs per person per year caused by (oo)cysts are shown in Table 2.In the three regions studied,the estimated risks ofCryptosporidiumorGiardiainfection for individuals per year ranged from 0-1.10 × 10-2and from 0-2.32 × 10-3,respectively,and the corresponding disease burdens ranged from 0-1.01 × 10-5DALYs pppy and from 0-1.97 × 10-6DALYs pppy,respectively.

Table 2. Annual probability of individual infection and disease burdens caused by Cryptosporidium and Giardia
Many previous studies have performed health risk assessments ofCryptosporidiumandGiardiausing the annual probability of infection for individuals (QMRA);however,except for several publications by Xiao et al.appraising DALYs[5,6],there is a sparsity of data with respect to drinking water in China.QMRA is the most commonly used method for microbiological risk assessment.The annual risk threshold of 10-4suggested by the USEPA and the acceptable disease burden threshold of 10-6DALYs pppy from waterborne exposure set by the WHO have been adopted for the evaluation ofCryptosporidiumandGiardiainfections.In this study,as shown in Table 2,the annual probability of infection for individuals in Jintan (CryptosporidiumandGiardia),Ezhou (CryptosporidiumandGiardia),and Binyang (Cryptosporidium) exceeded the USEPA threshold.The cryptosporidiosis burden per person per year due to the direct consumption of drinking and residual water in these three regions and the giardiasis burden in Jintan and Ezhou exceeded the tolerable value.A recent study showed that the occurrence rates ofGiardiain humans were 0.15%,2.08%,and 1.35% in Jiangsu Province,Hubei Province,and the Guangxi Zhuang Autonomous Region,respectively[10]. However,the annual probability of developing giardiasis for individuals(Pillyear) in our study was 0-1.16 × 10-3,5.45 ×10-6-6.00 × 10-4,and 0-1.27 × 10-5in Jintan,Ezhou,and Binyang,respectively.The main reason for the differences in Ezhou and Binyang may be that transmission through the daily consumption of water occupies only a small part of the various waterborne routes of transmission ofGiardiain both studied regions,eg.,swimming may also be an important route of transmission in these regions. The estimated disease burdens caused byCryptosporidiumandGiardiathrough the direct consumption of drinking and residual water in our study were lower than previous estimates in Zhejiang Province,China (6.51 × 10-5DALYs pppy forCryptosporidiumand 6.25 × 10-6DALYs pppy forGiardia),where swimming is considered to be the major exposure route[5,6].In Ezhou,the risk estimates based on treated water samples tended to be higher than those based on source water samples,which may imply ineffective treatment of source water in these waterwork facilities.Improved management and regular disinfection may be needed in these facilities.
The probability of infection from source water listed in Table 2 may be underestimated,since there are other exposure routes associated with infection,e.g.,irrigation and swimming.These have not been considered here when assessing the risks of infection byCryptosporidiumandGiardiain water.On the contrary,the risks may be overestimated because all the detected (oo)cysts were assumed to be viable and different species were not be discriminated.Not allCryptosporidiumandGiardiaspecies are pathogenic to humans. These non-pathogenic species may have been included in positive samples,but they do not result in clinical infection.In addition,chlorine dioxide used by Hubei province and the Guangxi Zhuang Autonomous Region,may have improved the removal efficiency for both protozoa,but this was not factored into the analysis due to its low dose and irregular use.Despite the potential under-and over-estimation of the risks,the information generated in this study is useful in drawing the attention of health administration departments endeavoring to develop strategies to reduce the exposure of local residents to (oo)cysts.
In conclusion,the QMRA conducted in these three densely populated regions of China demonstrated that the infection risks and disease burdens caused byCryptosporidiumandGiardiaare potentially significant.The protection of water sources should be implemented by the government.For local residents,drinking boiled water is recommended,and residual water consumption should be reduced to the greatest extent.
Authors' ContributionsSHEN Yu Juan,CAO Jian Ping,and CAO Sheng Kui conceived and designed the experiments;CAO Sheng Kui,JIANG Yan Yan,YUAN Zhong Ying,and YIN Jian Hai performed the experiments;XU Meng and XUE Jing Bo analyzed the data;CAO Sheng Kui wrote the manuscript;CAO Jian Ping,SHEN Yu Juan,and TANG Lin Hua revised the manuscript.All authors read and approved the final version of the manuscript.
AcknowledgementsWe thank HE Zu An,ZHANG Qiong,and WANG Jing (Hubei Provincial Center for Disease Control and Prevention),HE Jian Feng and LE Hai Hua (Changzhou Jintan District Center for Disease Control and Prevention),YANG Yi Chao and LIN Yuan (Guangxi Center for Disease Prevention and Control),LI Wei (Guangxi Binyang County Center for Disease Control and Prevention),and ZHANG Bo(Guangxi Lingshan County Center for Disease Control and Prevention) for assistance in water sample collection.
Conflict of InterestThe authors declare that no competing interests exist.
 Biomedical and Environmental Sciences2021年6期
Biomedical and Environmental Sciences2021年6期
- Biomedical and Environmental Sciences的其它文章
- Collaborative Efforts of Families,Schools,Health Care Providers,and the Government to Control Childhood Obesity in China
- The Improved Lipid Accumulation Product is an Accurate Index for Predicting Metabolic Syndrome in the Xinjiang Population
- Benzodiazepines and Amphetamines Use among Methadone Maintenance Participants and Their Associations with Treatment Adherence
- Campylobacter Outbreak Associated with Duck Blood Curd in 2019 in Shunyi District,Beijing,China
- Phylogenetic Analysis of Legionella Strains and ldentification of Serogroups by Lipopolysaccharide-and O-antigen-based PCR Assay*
- Development of a High-Resolution Melting Curve Analysis to Differentiate Candida parapsilosis Complex Species