
Tendon-regulating and bone-setting manipulation plus endurance resistance exercises for female with chronic neck pain
2021-10-27 08:27ZhangWendi張文娣ChenZhaohui陳朝暉ZhangHui張慧LiMengxing李夢醒ChengLulu程露露
Zhang Wen-di (張文娣), Chen Zhao-hui (陳朝暉),2, Zhang Hui (張慧), Li Meng-xing (李夢醒), Cheng Lu-lu (程露露)
1 College of Acupuncture-moxibustion and Tuina, Anhui University of Chinese Medicine, Hefei 230038, China
2 The First Affiliated Hospital, Anhui University of Chinese Medicine, Hefei 230031, China
Abstract
Keywords: Tuina; Massage; Science of Tuina (Traditional Chinese Medicine); Neck Muscles; Resistance Training; Neck Pain;Women
The full name of chronic neck pain (CNP) is nonspecific chronic neck pain (NCNP), which refers to a syndrome with a group of symptoms including neck pain,discomfort and limited movements as the chief complaints, with or without symptoms involving the head, shoulders, back and upper limbs. The duration of symptoms is not less than 3 months[1]. Epidemiological investigation shows that females are more prone to suffer neck pain than males, and the incidence ratio between males and females is close to 1:2[2-3]. Compared with males, the neck pain in female patients is more difficult to recover and more likely to develop into chronic neck pain[4], which is related to their weak strength of neck muscles and the smaller anteriorposterior diameter of thorax[5]. With the accelerated pace of life, the changed working style and the increased mental stress, the incidence and recurrence rates of CNP are gradually increasing, and the age of patients is getting younger. The disease not only brings physical and mental sufferings to patients, but also brings a great economic burden to their families and society. As a chronic musculoskeletal disease, conservative treatment is often adopted in clinical settings. Combined therapy is recommended in the guidelines for neck pain in Canada and the United States due to the limited effect of monotherapy[6-7]. Manipulation combined with functional exercises can improve both the short-term and long-term efficacy, and thus is highly recommended.We applied tendon-regulating and bone-setting manipulation combined with endurance resistance exercises in treating female CNP patients between January 2017 and November 2018, and tried to explore the mechanism. The details are as follows.
1 Clinical Materials
1.1 Diagnostic criteria
Patients experienced neck, shoulder and occipital pain with tenderness points, neck muscle tension, and limited head and neck movements. The lateral X-ray of cervical spine showed the change of curvature; the posterior edge of cervical spine and facet joint showed partial ghosting, and dynamic radiography might show the instability of intervertebral joint[8].
1.2 Inclusion criteria
Those who met the above diagnostic criteria with neck pain as the main complaint; female aged between 18 and 60 years old; with a duration ≥3 months; voluntarily participated in this study, were willing to cooperate with treatment and follow-up, and signed informed consent.
1.3 Exclusion criteria
Those whose neck pain was caused by fracture,dislocation, tumor, infection or other specific factors;those who were with obvious symptoms involving the nerve root, vertebral artery and spinal cord; with local skin ulceration, skin diseases or skin sensory disorders;with cognitive impairment, sensory aphasia, severe vision or hearing impairment; with such severe medical diseases as cardiovascular diseases, hematopoietic diseases, or endocrine diseases; were receiving treatment or received other effective treatments for CNP in the past month; were in pregnancy or lactation period.
1.4 Statistical methods
The SPSS version 23.0 statistical software was adopted for data analysis. Measurement data which met normal distribution were expressed as mean ± standard deviation (±s), andt-test was adopted. Measurement data which did not meet normal distribution were expressed by median (interquartile range), and the nonparametric rank sum test was adopted.P<0.05 indicated statistical significance.
1.5 General data
A total of 57 female CNP patients who received treatment from the tendon injury outpatient of the First Affiliated Hospital of Anhui University of Chinese Medicine and Guoyitang Outpatient Department of Anhui University of Chinese Medicine between January 2017 and November 2018 were recruited in the study.They were randomly divided into two groups: a manipulation group (29 cases) and a medium-frequency electrotherapy group (28 cases). All the 57 patients completed the treatment and follow-up. There were no significant differences in general data between the two groups (allP>0.05), indicating that the two groups were comparable (Table 1).
Table 1. Comparison of the general data of the two groups ( ±s)

Table 1. Comparison of the general data of the two groups ( ±s)
Group n Average age (year) Average duration (month) Head lowering time (hour)Manipulation 29 35.0±9.3 41.5±14.8 7.9±2.5 Medium-frequency electrotherapy 28 33.4±8.0 41.1±14.1 7.9±1.7 t-value 0.697 0.098 -0.056 P-value 0.489 0.922 0.955
2 Therapeutic Methods
Patients in both groups did the same endurance resistance exercises that were taught by the professional therapist. The therapist guided the patients once a week to ensure that they completed the exercises correctly.The exercises lasted about 30 min each time, and were did once a day, 6 times a week for total 5 weeks. The details are as follows[9].

Figure 1. Neck self-stretching exercise
Neck self-stretching exercise: Before resistance exercise, the patient relaxed relevant muscle groups by stretching including posterior occipital minor muscle group, sternocleidomastoid muscle, scalene muscle,trapezius muscle and levator scapulae muscle. Bent or rotated to the opposite side along the direction of the muscle to find the position with a sense of tension. Held the posture for 15 s, and stretched each part for 3-5 times (Figure 1).
Head resistance exercise: This exercise included resistance nodding and resistance raising. The patient took a sitting position with feet shoulder-width apart and back straight. When performing resistance nodding, put folded hands on the forehead to give it a slight resistance,and pull the jaw in (Figure 2). When performing resistance raising, put folded hands on the occipital part to give it a slight resistance, and make mandibula adduction (Figure 3). Held the final position for 10 s, and then returned the neck to the median position against the resistance. Did the exercises 15 times in each direction and rested for 3 s every 2 times.
Neck resistance exercise: This exercise was done in four directions, including forward flexion, backward extension and left and right lateral flexion. The patient took a sitting position with feet shoulder-width apart,back straight and jaw in. Put the hands on the forehead,occipital part or both sides of the head to give resistance.The cervical spine was naturally and slowly against the resistance to complete the full range of joint movements.Held the final position for 10 s, and then returned the neck to the median position against the resistance. Did the exercises 15 times in each direction and rested for 3 s every 2 times (Figure 4).
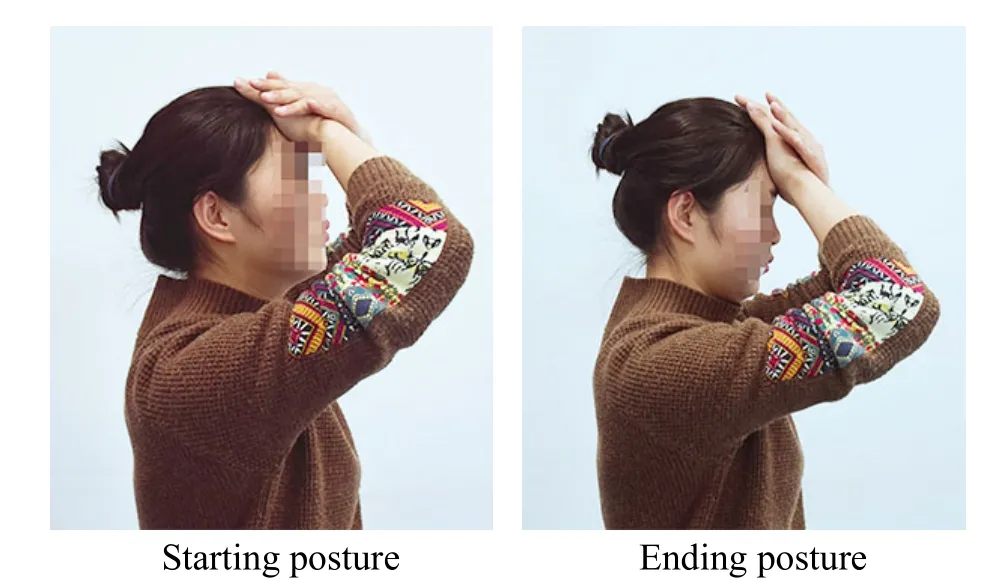
Figure 2. Resistance nodding
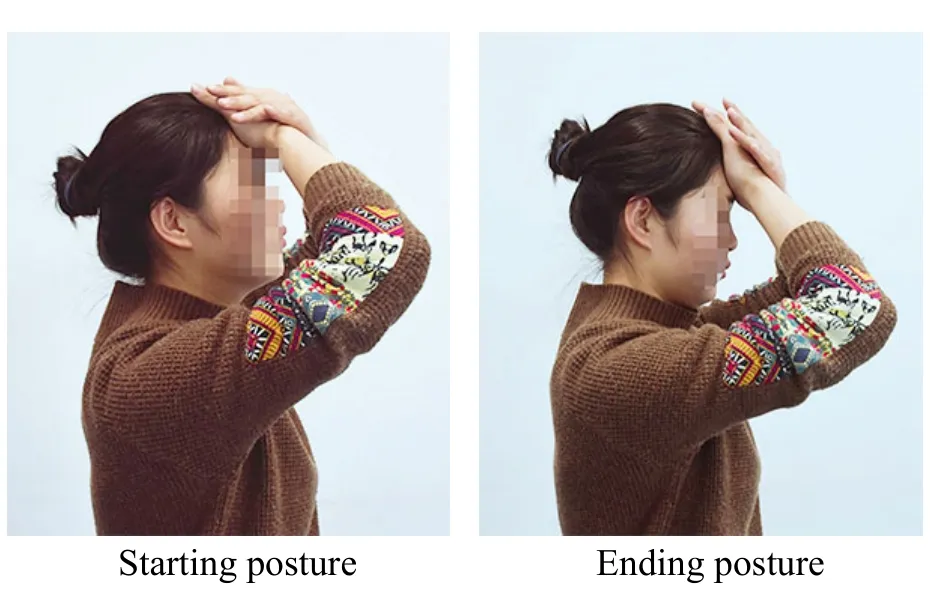
Figure 3. Resistance raising

Figure 4. Neck resistance exercise
Chest-opening and shoulder-lifting exercise: The patient took a sitting position with feet shoulder-width apart. Fully extended the shoulders backward, and then slowly lifted them upward. Held the final position for 10 s. Did the exercise 15 times and rested for 3 s every 2 times (Figure 5).

Figure 5. Chest-opening and shoulder-lifting exercise
Ending exercise: The patient continued the previous exercise, An-pressed and Rou-kneaded Fengchi (GB 20)on both sides with the thumbs 7 times for each side, and then used the palm to Rou-knead along the posterior hairline of the neck to the 7th cervical vertebra for about 30 s until she experienced hot sensation.
2.1 Manipulation group
Patients in the manipulation group received additional treatment of tendon-regulating and bone-setting manipulation. Before treatment, the treatment scheme was determined and the therapist was trained to ensure the standardized manipulation[10-11]. Each time the treatment lasted about 25 min, once every 2-3 d, 3 times a week for 5 weeks. The details are as follows.
Tendon-regulating manipulation: The patient took a sitting position. The therapist first relaxed the patient's neck, shoulder and upper back muscles with Gun-rolling,Rou-kneading, Nian-twisting and Na-grasping manipulations. Then digital An-pressed and Nian-twisted the clustered nodules. Generally, tenderness points or nodules can be found around the sternocleidomastoid muscle, scalene muscle, superior trapezius muscle and cervical transverse process. In addition to finding and loosening local tenderness points, potential trigger points can also be found along the meridian route (Figure 6 to Figure 8).
Bone-setting manipulation: The first one was the manipulations of relaxing intervertebral joints and costa vertebral joints. The patient took a sitting position. The therapist stood behind the patient's side to find the cervical dislocation. The purlicue of the same hand was stuck to the dislocation, and the purlicue of the other hand was stuck to the upper segment of the dislocation.The two hands formed an opposite force to perform a small-range relaxing manipulation at a regular rhythm at the end of the displaced cervical segment. The same relaxing manipulation was applied to the first and second costa vertebral joints. The manipulation was performed for 3 to 5 times at each joint (Figure 9). The second was to adjust the sternocostal joint. The patient took a sitting position, and the therapist stood behind his affected side.The therapist put a hand over the patient’s shoulder joint and pressed the thenar against the first and second sternocostal joints. Then the therapist put the other hand behind his shoulder and pushed the joint upward with both hands at the same time. The main force was from the front hand. The manipulation was performed for 3-5 times at each joint (Figure 10). The last one was the rotation method. The patient took a sitting position.The therapist stood behind the patient's affected side,held the patient's jaw with an elbow, and held the other hand on the occipital part. Then the therapist gently shook his neck several times to relax the muscles, and then maintain the traction to turn his head to the healthy side to the maximum range. The force was functioned on the affected side. When a sense of fixation was reached,the therapist suddenly and quickly pulled the cervical spine on the affected side. Joint clicking could often be heard. The same manipulation was then performed on the healthy side (Figure 11). Bone-setting manipulation lasted about 8 min.
Ending manipulation: Pi-chopping manipulation and neck Guihe-resetting manipulation were adopted for relaxation (Figure 12 to Figure 13).

Figure 6. Gun-rolling manipulation

Figure 7. Rou-kneading and Nian-twisting manipulations

Figure 8. Na-grasping manipulation
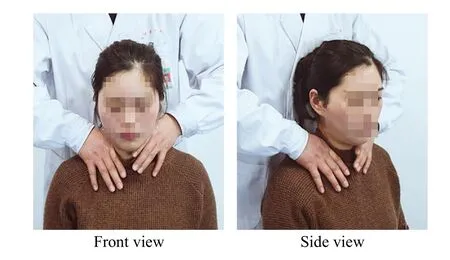
Figure 9. Relaxing the intervertebral joints and costovertebral joints
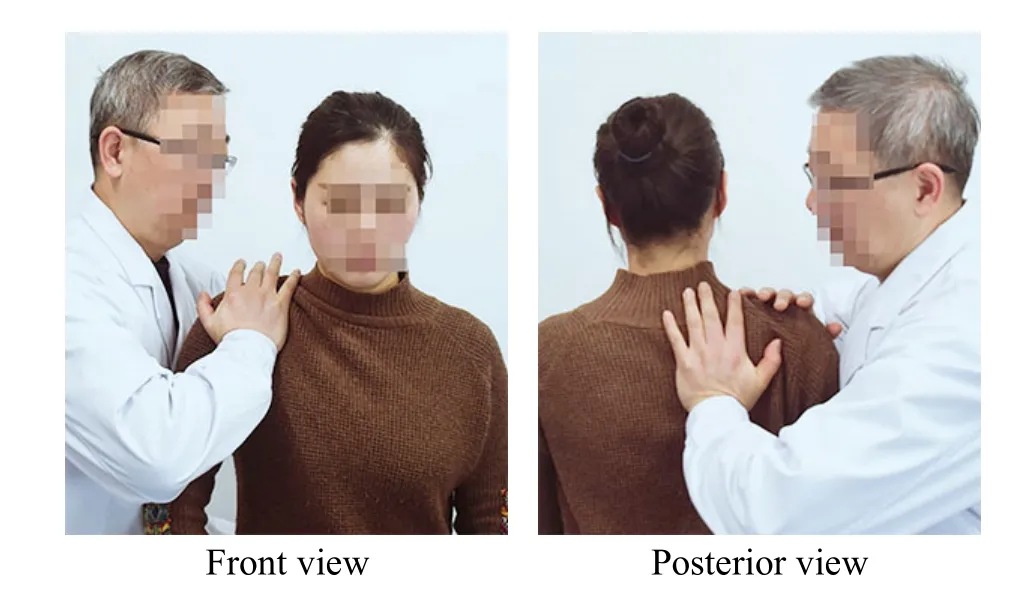
Figure 10. Adjustment of the sternocostal joints

Figure 11. Rotation manipulation

Figure 12. Pi-chopping manipulation

Figure 13. Guihe-resetting manipulation
2.2 Medium-frequency electrotherapy group
Patients in the medium-frequency electrotherapy group received additional medium-frequency electrotherapy by adopting the modulated mediumfrequency therapeutic instrument.
The patient took the prone position and exposed his neck and shoulders. After local disinfection with 75%alcohol cotton ball, 2 to 3 layers of 8 cm × 4 cm wet cotton cloth were pasted on the skin behind the neck as pads. The electrodes were pasted on the cloth and fixed with sandbag or elastic bandage (Figure 14). The parameters could be adjusted until the patient experienced tolerable sensations of tingling, tremor or muscle contraction under the electrodes. Each treatment lasted for 20 min, once a day. The patient rested for one day every 6 times and the treatment lasted for 5 weeks.

Figure 14. Medium-frequency electrotherapy
3 Observation of Clinical Efficacy
3.1 Observed items
Visual analog scale (VAS) and Northwick Park questionnaire (NPQ) were used to evaluate the degree of neck pain and neck dysfunction before and after treatment, and at follow-up. The score of VAS was between 0 and 10 points. The higher the score, the higher the degree of pain[12]. The NPQ included 9 items,with each item between 0 and 4 points, and the total score between 0 and 36 points. The higher the score, the worse the patient's neck function[13-14].
Wagner Force TenTM-Model FDX hand controlled digital pressure gauge (Wagner Instruments, USA) was used to evaluate the tenderness of patients before and after treatment.
Flexcomp Infiniti 10 surface electromyography (sEMG)detector (Thought Technology, Canada) and Biograph Infiniti software system were used to collect the root mean square (RMS) and median frequency (MF) under isometric contraction of sternocleidomastoid muscle and posterior cervical extensor muscle before and after treatment.
3.2 Results
3.2.1 Comparison of the VAS score
After treatment, the VAS scores of both groups were lower than those before treatment (bothP<0.05), and the VAS score of the manipulation group was lower than that of the medium-frequency electrotherapy group(P<0.05). At follow-up, the VAS score of the manipulation group was lower than that before and after treatment(bothP<0.05), and lower than that of the mediumfrequency electrotherapy group at the same time point(P<0.05). Check Table 2 for details.
3.2.2 Comparison of the tenderness values
After treatment, the neck tenderness values of patients in both groups were higher than those before treatment (bothP<0.05), and that in the manipulation group was higher than that in the medium-frequency electrotherapy group (P<0.05). Check Table 3 for details.3.2.3 Comparison of the MF and RMS values
After treatment, the MF and RMS values of sEMG of the sternocleidomastoid muscle and cervical extensor muscle in the two groups were higher than those before treatment (allP<0.05), and those in the manipulation group were higher than those in the medium-frequency electrotherapy group (allP<0.05). Check Table 4 for details.
Table 2. Comparison of the VAS score between the two groups ( ±s, point)

Table 2. Comparison of the VAS score between the two groups ( ±s, point)
Note: VAS=Visual analog scale; compared with the same group before treatment, 1) P<0.05; compared with the same group after treatment,2) P<0.05; compared with the medium-frequency electrotherapy group at the same time point, 3) P<0.05
Group n Before treatment After treatment Follow-up Manipulation 29 5.90±1.29 3.14±0.641)3) 2.07±0.591)2)3)Medium-frequency electrotherapy 28 5.43±1.10 4.04±0.741) 3.75±0.701)
Table 3. Comparison of the tenderness value between the two groups ( ±s, N)

Table 3. Comparison of the tenderness value between the two groups ( ±s, N)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the medium-frequency electrotherapy group after treatment,2) P<0.05
Group n Before treatment After treatment Manipulation 29 20.62±5.43 50.45±8.501)2)Medium-frequency electrotherapy 28 20.29±8.29 42.66±9.011)
Table 4. Comparison of the MF and RMS values between the two groups ( ±s)

Table 4. Comparison of the MF and RMS values between the two groups ( ±s)
Note: MF=Median frequency; RMS=Root mean square; compared with the same group before treatment, 1) P<0.05; compared with the medium-frequency electrotherapy group after treatment, 2) P<0.05
Group n Position MF value RMS value Before treatment After treatment Before treatment After treatment Manipulation 29 Sternocleidomastoid muscle 52.62±5.84 82.34±7.831)2) 252.24±16.09 384.28±11.661)2)Cervical extensor muscle 104.10±10.79 133.41±6.491)2) 23.59±4.35 40.45±7.511)2)Medium-frequency electrotherapy 28 Sternocleidomastoid muscle 54.00±4.64 67.14±7.921) 251.36±13.98 341.82±10.461)Cervical extensor muscle 107.54±8.83 117.61±5.871) 25.75±5.47 33.82±6.791)
3.2.4 Comparison of the NPQ score
After treatment, the NPQ scores of the two groups were lower than those before treatment (bothP<0.05),and that in the manipulation group was lower than that in the medium-frequency electrotherapy group (P<0.05).At follow-up, the NPQ score in the manipulation group was lower than that before and after treatment, and also lower than that in the medium-frequency electrotherapy group at the same time point (allP<0.05). Check Table 5 for details.
Table 5. Comparison of the NPQ score between the two groups ( ±s, point)

Table 5. Comparison of the NPQ score between the two groups ( ±s, point)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the same group after treatment, 2) P<0.05; compared with the medium-frequency electrotherapy group at the same time point, 3) P<0.05
Group n Before treatment After treatment Follow-up Manipulation 29 17.86±3.85 9.21±2.691)2) 7.69±2.691)2)3)Medium-frequency electrotherapy 28 18.07±3.29 12.57±3.241) 12.50±3.241)
4 Discussion
There is no proper disease name for CNP in traditional Chinese medicine (TCM). It falls under the category of Biimpediment syndrome and stiff neck, which is mostly caused by the pathogenic wind, cold and dampness. The internal cause of CNP is deficiency of healthy qi and the external cause includes contraction of the six excesses,overexertion and traumatic injury. The pathogenesis can be identified as deficient root and excessive superficial manifestations. The root includes insufficiency of the liver and kidney, deficiency of qi and blood, and malnourishment of the tendons and bones. The superficial is caused by the obstruction of wind, cold and dampness in the meridians and collaterals, and qi stagnation and blood stasis. Compared with males,females are more prone to have deficiency of the liver and kidney, and are more vulnerable to negative emotions. Therefore, they are more likely to experience neck discomfort. Long term pain and discomfort will in turn affect the mind to aggravate patients' anxiety and depression. Thus, female CNP patients were selected as the research object in this study.
Modern medicine has confirmed the multifactorial pathogenic characteristics of CNP, but its pathogenesis has not been completely clear. There is a consensus that muscles play a significant role in the occurrence and development of CNP. The neck muscle groups have their own features[15]: first of all, the muscle bundles are few and slender, with small muscle strength and poor endurance, which cannot withstand large external loads and cannot complete long term loaded work; secondly,the neck muscles have sufficient innervation, rapid and sensitive response and high coordination, but it is sensitive to external noxious factors and easy to be unbalanced. Cervical muscles, especially deep cervical muscles, play an important role in forming cervical curvature, maintaining cervical stability and completing cervical movements. When the local part is damaged, it is easy to affect the overall coordination, and subsequent dysfunction of the head and neck[16]. Specifically, the strength and endurance of multiple neck muscle groups in CNP patients will be reduced, especially the endurance[17]. Atrophy of deep cervical muscles in CNP patients can be found via muscle bone ultrasonic imaging equipment[18-19]. In addition, the decrease of neuromuscular coordination ability of deep and superficial, flexor and extensor muscles are also among the pathogenic factors of CNP. Falla D,et al[20-21]detected through EMG equipment that the activation level of deep neck muscles decreased while the superficial muscles were recruited first in neck movement due to compensation, and the recruitment degree was higher,resulting in faster fatigue and exhaustion. Although it is an effective compensatory strategy to activate the deep and superficial muscles of the neck in the early stage during exercise, which can alleviate acute neck pain, the change of exercise mode will further reduce the stability and coordination of the cervical spine, thus aggravating the injury[22]. And there is evidence that this abnormal movement pattern of neck muscle group will not return to normal with the relief of neck pain[23]. When the soft tissues of the neck are damaged and the normal balance of the cervical spine is broken, aseptic inflammation and pain will present locally. Patients would reduce neck movements to avoid pain, which will lead to the decline of strength, endurance and stability of local muscle groups. This abnormal change of cervical muscle group will affect the feedback mechanism of nervous system,further lead to the decline of neuromuscular coordination ability, aggravate the injury, and thus form a vicious circle. Therefore, in the clinical treatment of CNP,improving the strength, endurance and coordination of cervical muscle group and strengthening the dynamic stability of cervical spine can achieve therapeutic effects.
Tendon-regulating and bone-setting manipulation,laying stress on both muscles and bones, is one of the commonly used external treatment methods in TCM.The manipulation is light and gentle, and is widely used in the treatment of musculoskeletal diseases. This method has the functions of dredging meridians and collaterals, regulating qi, blood and tendons, smoothing joints and adjusting Zang-fu organs. In this study, the tendon-regulating manipulations included Gun-rolling,Na-grasping, Rou-kneading and Nian-twisting manipulations. In addition to relaxing the local painful nodules, we also identified the location of the disease along the meridian route and found the potential trigger points. From the perspective of muscle region, the muscle region of the three yang meridians of hand pass through the neck, and the Hand Taiyin Meridian is also closely related to the neck. These muscle regions originate from the extremities and are distributed centripetally. Therefore, in clinical treatment, we can adjust and relax the whole muscle region by manipulating the starting points to obtain effects more with less. In addition to the tendon-regulating manipulation, bone-setting manipulation is also essential. Since this disease involves the muscles and bones, both of them are emphasized in treatment[24-25].The relaxing manipulation of intervertebral joints and costovertebral joints acts on the adjacent cervical intervertebral joints and the first and second costovertebral joints, which can smooth the joints,improve the range of joint movement, and enhance the proprioception of the neck. Sternocostal joint adjustment can improve the patient's bad posture such as hunchback and shoulder buckle, and reduce the abnormal tension of the superficial muscles in the front of the neck. The rotation method can adjust the disorder of cervical facet joints and release the adhesion of soft tissues. In clinical settings, the best therapeutic effects can be achieved by tendon-regulating manipulation combined with bone-setting manipulation.
In addition, in the treatment of CNP, attention should be paid to the combination of dynamic and static exercises and functional exercises. Targeted endurance resistance exercises can improve the muscle strength and endurance of neck muscle group, enhance the stability of neck, improve muscle fatigue, increase blood circulation, promote the metabolism of inflammatory substances and relieve pain. And the exercises can further maintain and consolidate the efficacy of manipulation. Therefore, tendon-regulating and bonesetting manipulation combined with corresponding exercise therapy has been a conventional model for treating chronic musculoskeletal diseases.
sEMG, also known as dynamic electromyography, is a simple, effective and non-invasive objective measurement tool to evaluate such indicators as muscle strength, muscle group coordination and muscle fatigue.In this study, MF and RMS values were used to evaluate the improvement of fatigue and recruitment strength of cervical flexor and extensor muscles. MF value belongs to frequency domain analysis index, with good specificity and sensitivity for evaluating the fatigue degree of muscle activity[26]. The RMS value belongs to the time domain analysis index, directly related to the energy of EMG signal, and can effectively evaluate the recruitment degree of muscle fibers[27]. The results of this study showed that after treatment, the fatigue of cervical flexor and extensor muscles decreased and the recruitment degree increased, and the improvement in the manipulation group was more notable than that in the medium-frequency electrotherapy group.
In conclusion, the results of this study suggests that tendon-regulating and bone-setting manipulation combined with endurance exercises can effectively relieve the pain and dysfunction in CNP patients, and the efficacy was better than that of medium-frequency electrotherapy combined with endurance exercises. This may be related to the increase of pain threshold, the increase of neck muscle recruitment and the reduction of fatigue. The results of this study also demonstrated that manipulation can not only treat tendon and bone diseases, but also relieve the emotional sufferings of patients. Therefore, they cannot be replaced by modern instruments.
Some shortcomings also emerge from this study. For example, the inclusion of female CNP patients from only one region demonstrates a certain selective bias. Besides,the intervention scheme used in this study is the combination of the two therapies, and which therapy should the efficacy be attributed to needs to be explored in future studies. Besides, we can also use the self-rating anxiety scale to further explore the psychological changes in the patients.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by General Project of National Nature Science Foundation of China (國家自然科學(xué)基金面上項(xiàng)目, No. 81674076); Key Project of Natural Science Foundation of Anhui Provincial Education Department (安徽省教育廳自然基金重點(diǎn)項(xiàng)目, No. KJ2018A0273).
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 29 October 2020/Accepted: 19 December 2020
猜你喜歡
教育家(2022年17期)2022-04-23
國際放射醫(yī)學(xué)核醫(yī)學(xué)雜志(2021年6期)2021-11-30
國際放射醫(yī)學(xué)核醫(yī)學(xué)雜志(2021年1期)2021-11-30
花火·繪閱讀(2021年2期)2021-09-10
西安航空學(xué)院學(xué)報(bào)(2018年5期)2018-10-15
中國氣象科學(xué)研究院年報(bào)(2017年0期)2017-07-19
文藝論壇(2015年23期)2015-03-04
中國篆刻·書畫教育(2014年1期)2014-03-10
中國醫(yī)藥生物技術(shù)(2012年5期)2012-02-03
 Journal of Acupuncture and Tuina Science2021年5期
Journal of Acupuncture and Tuina Science2021年5期
- Journal of Acupuncture and Tuina Science的其它文章
- Exploring the effect of acupuncture plus mild hypothermia on miRNA-204 and its target gene expressions in CIRI rat brain tissues based on MAPK signal pathway
- Experimental observation of effects of acupoints,cone numbers and durations of moxibustion with different moxibustion methods on skin surface and inside temperature
- Therapeutic massage for knee osteoarthritis:a systematic review and meta-analysis of randomized controlled trials
- Clinical efficacy observation of ‘Tong Du Yun Pi’manipulation for infantile diarrhea in autumn
- Clinical observation on moxibustion therapy plus tuina in treating children with recurrent respiratory tract infections due to qi deficiency of spleen and lung
- Effects of acupuncture plus language training on language function and cerebral blood flow in patients with motor aphasia after ischemic stroke