
Effective of exercise therapy on functional balance, physical performance and quality of life among patients undergoing hemodialysis:randomized controlled trial
2022-02-15 04:54AhmedLateefAlkhaqani
Nursing Communications 2022年13期
Ahmed Lateef Alkhaqani
1College of Nursing,University of Kufa.
Abstract Background: Patients undergoing hemodialysis suffer from deteriorating physical health,impaired physical function, and have a low quality of life, that explained by insufficient metabolic clearance. To overcome these obstacles, cost‐effective strategies must be developed, including exercise as a complement to hemodialysis therapy. Objective: To determine the effectiveness of exercise therapy on functional balance, physical performance,and quality of life among patients undergoing hemodialysis: a randomized controlled trial.Methods: This randomized controlled trial study was carried out on 68 patients with chronic kidney disease undergoing hemodialysis for at least six months and had a medically stable condition who were randomly divided into training (n = 32) exercise therapy and (n= 31) control, groups. The training group participated in 8‐week (3 sessions per week)resistance exercise therapy in three sets of 10 repetitions of knee extension, hip flexion, and hip abduction with the use of an elastic band under the supervision of a training physiotherapist and researcher during the first hour of the three routine hemodialysis treatment session per week. But the control group did not experience any intervention. To analyze the data, two‐way analysis of variance and Bonferroni statistical tests were used at the significant level of (P= 0.05).Results: 6 Minute‐Walk Test (6MWT) (0.013),and in the Physical Activity Scale for the Elderly (PASE) (0.014), and Short Survey Form 36 (SF‐36)questionnaires and health‐related quality of life (HRQOL) (0.001) had significant improvements in the training group in comparison to the control group from pre to post‐test,also physical performance (0.001) was improving as compared with control group (0.89) at(P = 0.05). Conclusion: Resistance exercise therapy interventions for eight weeks effectively improve the physical function and performance, activity levels, and health‐related quality of life of patients with chronic kidney disease and undergoing regular hemodialysis compared with a control group.
Keywords:functional balance; hemodialysis;exercise therapy; physical performance
Highlights
The global burden of CKD is increasing, and it's projected to become the 5th most common cause of life‐years globally by 2040. The problems may impair the patient’s ability to carry out activities of daily living. Therefore, poor physical performance is a common complication associated with CKD; low physical activity and impairment are associated with elevated risks of disability and death.In addition, patients with CKD on maintenance HD suffer from a progressive deterioration of impaired physical function and is associated with increased mortality and morbidity and the reduced quality of life and leads to decreased physical activity of patients.
Introduction
Chronic kidney disease (CKD) is a worldwide health burden with high costs to the health system. It is one of the significant health problems,and it is a general term that describes kidney damage or lower glomerular filtration rate (GFR) [1]. End‐stage renal disease (ESRD),the last stage of chronic kidney disease, is a common chronic disease with increasing prevalence and incidence [2]. Hemodialysis (HD) is the primary treatment option for patients with end‐stage renal disease.Chronic disease is a challenge for patients who have suffered from it for a long time[3].Anemia,bone diseases,heart diseases,and oedema are the most common complications of chronic renal disease [4].Chronic Kidney Disease is an exponentially growing disease that accounts for a world prevalence of 9.1% and shows even bigger numbers in countries such as Spain, which has a prevalence of 15.1%.Patients with CKD on maintenance hemodialysis suffer from a progressive and gradual deterioration of impaired physical function.This is associated with a higher risk of mortality and morbidity and leads to decreased physical activity and health‐related quality of life levels [5].
In addition, sleep disorders, fatigue, and sexual dysfunction [6].These problems may affect patients’ ability to perform daily activities.Consequently, low physical function is a common problem associated with chronic kidney disease; low physical activity and disability are associated with an increased risk of disability and death [7].Furthermore, patients with CKD on maintenance HD suffer from a progressive deterioration of impaired physical function, which is associated with increased mortality and morbidity and reduced quality of life and leads to decreased physical activity of patients [8].
Worldwide chronic kidney disease is causing an increase in the global burden, and it is predicted that by 2040 it will become the fifth most common cause of death worldwide [9]. The cost of hemodialysis and kidney transplantation consumes about 2‐3% of the annual healthcare budget in high‐income countries; Spending on less than 0.03% of the total population of these countries [10, 11]. In low‐ and middle‐income countries, most people with kidney failure do not have enough access to life‐saving dialysis and kidney transplants [1].Chronic kidney disease is an exponentially growing disease that accounts for a world prevalence of 9.1% [12]. It shows even bigger numbers in countries such as Iraq, which have a prevalence of 6.6%.
According to the reported “World Health Organization", “physical inactivity is already a major global health risk and prevalent in both industrialized and developing countries, causing approximately 5.2 million deaths.Physical inactivity is the primary cause of most chronic diseases, and it is one of four main risk factors of CKD” [13]. Today’s society is very important for physical activity. Exercise maintains the body’s strength and health [14]. Therefore, increased physical activity is an important aspect of preventing and managing patients with CKD[15]. The "National Institute for Health and Care Excellence" “NICE”recommends in guidelines for CKD in adults the following: Encourage patients suffering from chronic kidney disease to take exercise, stop smoking and achieve a healthy weight [16]. The "American National Kidney Foundation" (ANKF) These guidelines contain similar statements that encourage CKD to exercise, stop smoking, and lose weight [17]. Physical activity improves various metabolic benefits,thereby reducing the long‐term risk of recurrence of kidney dysfunction and easing.
Despite this, exercise programs are not commonly implemented on dialytic routines in many countries due to a myriad of existing barriers that healthcare professionals have to face when trying to propose an exercise intervention during dialysis. These barriers include lack of knowledge, fear of injury or medical complications, fatigue, or just simply a lack of motivation by both the patient and the healthcare professional[5]. Many studies focus on overcoming these barriers. For example, nurse‐led exercise interventions have been previously proven to be efficient in physically impaired populations, such as the elderly, complex ambulatory, or diabetic patients [18]. In studies involving patients with CKD, these types of interventions have also improved clinical outcomes and reduced hospitalization rates.Although it is increasingly recognized that physical activity needs to be promoted, the existing evidence base for the cost‐effectiveness of relevant interventions appears to be weak and dispersed. This experimental study contributes to the most important topic in medical studies to fill and address the literature gap. This study aimed to determine the effectiveness of exercise therapy on functional balance,physical performance, and quality of life among patients undergoing hemodialysis:a randomized controlled trial
Patients' quality of life undergoing hemodialysis can be affected by social factors causing major changes in the life of patients with CKD,also affected by clinical changes caused by the disease and its complications. Therefore, getting information about this subject can be useful in identifying patients at risk. Decreased quality of life in hemodialysis patients may affect different aspects of their life.Impaired quality of life from the physical perspective can change the patient's functional status. So that, the patients' daily physical activity is disrupted, and their ability to perform daily activities is decreased.Changes in living patterns and their limitations impose complex and changed lives on the patients and their families and, finally, reduce their quality of life [19].
Materials and methods
Ethical Considerations and Administrative Agreements
Before conducting the study, a legal and government agreement was approved for ethical study by the University of Kufa’s Research Ethics Committee, Medicine College., Ministry of Planning/Central Council for Statistics, according to the standards for researching with human beings. In addition, the researcher also obtained the approval of the designer's short physical performance battery to use this tool. Also, in order to respect the principles and desires of the participants in the study, the researcher obtained informed consent from each study participant using the subjects’ agreement sheet, which was formed according to scientific resources. The purpose and right to participation and withdrawal from the study are clearly explained to participants and voluntary participation.
Study design
Randomized Controlled Trial (RCT) with two arms was chosen to be applied to patients assigned into two groups (exercise therapy and control group) in the current study to determine the program's effectiveness on participants' physical performance. The study was carried out for eight weeks, from 21/12/2020 to 18/2/2021.
Participants Selection
According to the "National Kidney Foundation" (NKF) and “American Society of Nephrology”, chronic kidney disease diagnosis clinical practice guidelines, 68 participants, 43 male and 20 female eligibles,were recruited to participate in the present study (selected randomly 34 patients from each center, "Al‐Sadder Medical City" and"Al‐Hakeem General Hospital"/Hemodialysis Center) (68 patients)who admitted there during the period study. All participants with ESKD meet the inclusion criteria for participation [20]. And each group has 34 patients.
Sample and Sampling Technique
63 patients were selected and included in the current study. Those who were subjected to taking a medical history and completing a clinical examination were performed. The researcher uses the following criteria to specify subjects to be present study. Excluded basically all patients out of these criteria; These criteria were determined with the help of nephrologists.
(1). According to the Oklahoma Health Care Authority policy and rules, all patients have three or more sessions weekly; rehabilitation programs cannot be applied in less than two sessions because of time intervals between sessions,there is no evidence of progress.
(2). Because of the need to measure subjectively, the study should warn patients and exempt any consciousness level changes.
(3). Participants to have been treated with hemodialysis for at least three months.
(4). To avoid complications, medically stable patients, as reported verbally by doctors.
Exclusioncriteria:Patientswithabsoluteorrelative contraindications to exercise tests.
Sample Size
In randomized controlled trials, statistical power is usually set to 0.80,and many clinical experts are now advocating 0.90 power sets [21].The sample size estimated to be needed for this research, based on the criteria for entering the research purposefully using G*Power 3.1.7 software and considering an alpha level of 0.50 and the average effect size,and the desired power of 0.08 was about 54.Including a 10%loss during the study.But the researcher set the statistical power at 0.99 to reduce to 0.01 the possibility of a “false negative” result and to increase the study's power; the researcher increased the sample size to(63) patients. The researcher based on the confidence interval (0.99)to determine the effectiveness of the program and whether there(P‐value < 0.01) was a considered a statistically significant difference.
Groups Assignment
63 patients’ sample was randomly assigned to two groups. The study group included 32 patients who were exposed to the research intervention program of exercise training. The non‐intervention group was considered a control group consisting of 31 patients who didn’t expose to the exercise training program.
Randomization
After the initial assessment, the patients were randomly assigned by computer with a list of random numbers created by investigators who did not participate in the study. The allocation aims to prevent selection biases and ensure control against accidental confusion. The study followed the guidelines established to maintain the separation of the control group from the study group and avoid contact between them. The patient was assigned to each group once a week. See participant’s flowchart (Figure 1). Consequently, the outcome data and analysis of the post‐study; the total sample of the study (50).
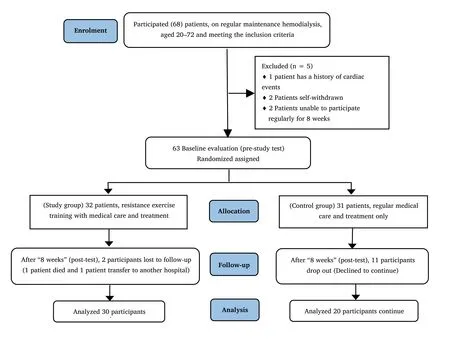
Figure 1 Flowchart of participant
Blinding
The current study used a double‐blinded technique; the data analyst doesn't know the study groups allocation. Furthermore, the researcher and participants who have obtained outcomes are unaware of the control and study groups.
Exercise therapy group
32 patients received resistance exercise training with medical care and treatment applied by the researcher. Two patients have not completed the program after eight weeks (post‐test) (one patient transferred to another hospital, and one patient died). In the study group, the intervention program was provided for eight weeks under therapist(physiotherapist) and researcher supervision during the first hour of the three routine hemodialysis sessions weekly and during self‐training. Performed all exercises with the help of a seated position or a supine position. The training sessions were usually warm‐up and cool‐down periods for the group. They are composed of 15 to 20 minutes of stretching exercises for the hip's triceps sural, hamstrings,and external rotator muscles.
The Control Group
31 patients were only on regular treatment and medical care. After an eight weeks follow‐up (post‐test). In the control group, patients were guided to maintain their routine medical care and their usual study physical activity. Still, they didn’t engage in any exercise program.Participants in control groups were exposed only to center‐only normal activities.
Collection of Data
used face‐to‐face interviews for socio‐demographic purposes. Before Administering the intra‐dialytic resistance exercise training to the patients, clinical data and physical performance status were assessed as a pre‐test for both groups. The Data Collection was done at Al‐Sadder Medical City and Al‐Hakeem Hospital/The specialized center for kidney diseases and transplant/Hemodialysis Unit.Regarding physical performance assessment, Sit‐to stand‐to‐sit 10 and 60 tests(STS),6 Minute Walk Test(6MWT),Physical Activity Scale for the Elderly (PASE), the researcher uses the guided observation technique to assess the patients’ physical performance, STS‐10,STS‐60, 6MWT, PASE, before and after application of the program.The method of started data collection on 21/12/2020 to 18/2/2021.The outcome was evaluated by collecting patient requests using resistance training and monitored closely. The researcher uses post‐test assessment periods after eight weeks of the program application. Each patient needs 15 to 20 minutes to answer questions and checklists. The protocol was registered at the "International Clinical Trials Registry Platform" (ICTRP) in WHO (Registration Number IRCT20210312050679N1).
Statistical Analyses
All continuous variables have been tested to be statistically normalized using the Shapiro–Wilk test and demonstrated to be normalized (normal distribution). Microsoft Excel (2019) and Statistical Package for the Social Sciences (SPSS) version 20 are used for statistical data analysis. Descriptive Analysis: presented as tables,percentages, frequencies, graphic presentation by using bar charts(statistical figures), and the participants' statistical mean and standard deviation were calculated. Inferential Analysis: Statistical tests were applied according to the type of variables and distribution. Used chi‐squared tests to compare baseline characteristics; the homogeneity test was used to confirm that there was a significant difference between the control and intervention groups. The baseline of mean changes was compared between two samples using t‐tests.
Description of the exercise therapy programs
The main researcher performed the intervention and physical therapy staff members. The nursing staff delivered trial exercise sessions for two weeks with the assistance of the main researcher, a physical therapist who specialized in exercise interventions, in order to familiarize with the procedure and the equipment. This intervention lasted for eight weeks, where participants performed 1‐hour exercise sessions three times a week for a total of 24 exercise sessions. Exercise progression was discussed by both the nursing staff and the main researcher based on Borg’s perceived exertion scale, which was routinely passed to the participant. Participants were asked to perceive around 12 points on this scale, equivalent to a “somehow hard”effort.
Group sessions began with a 5‐minute warm‐up consisting of active joint mobilizations, followed by a strengthening section. Exercises training program composed of 3 sets of 10 repetitions of Knee extension, Hip flexion, and Hip abduction with the use of an elastic band "TheraBand Resistance Band Loops, THERABAND, Ohio, USA",surrounding the ankles or above the knees are in a sitting or lying position, depending on the patient’s preference or ability. The intervention of resistance exercises was carried out with slow movements. Participants were instructed to “cool down” with active joint mobilizations and stretching exercises when finished.
Outcomes
Every test was performed an hour before the dialytic treatment in the same order for every participant at baseline and after eight weeks of intervention. Selected a two‐month interval and used post‐test measure with high test‐retest validity and reliability in the populations' hemodialysis among older adults to assess physical performance [22]. Both assessments were administered by the same researcher, blinded to allocation, for every participant in order to avoid possible interrater bias. Tests were administered following specific scripted instructions.
Primary outcome measures
Outcome measures assessed change from baseline at eight weeks for the following: “Short Physical Performance Battery” (SPPB): A combination of physical tests that assess balance, gait speed, and lower limb functional strength that total score ranging from (0 to worst) to (12 best); each test was scored on a scale of (0 to 4 points)with using cut point criteria established by Guralnik et al., as follows:low performance (0‐6 points), intermediate performance (7‐9 points),and high performance (10‐12 points) [23]. The Short Physical Performance Battery is widely used in both clinical and research settings also, it’s a validated measure function of the lower extremity in patients with chronic kidney disease and is predictive of mortality and disability [24].
Secondary outcome measures
Sit‐to stand‐to‐sit 10 and 60 tests (STS): Used for resistance and strength assessment, respectively, of the lower limbs muscle capacity force. STS‐10 is calculated as the total time needed to complete 10 consecutive repetitions of standing up and sitting down again,whereas the STS‐60 registers the number of repetitions performed in 60 seconds. This test is simple, inexpensive, rapid, and reproducible and is included in the battery of tests used for people with renal disease. The STS10 and STS‐60 have been found to be valid measures of lower body muscle endurance force. The 6 Minute Walk Test(6MWT) was conducted according to the recommendations of the American Thoracic Society. The 6MWT is an indicator of the participant’s functional capacity. It registers the maximum number of meters the participant is able to walk in a 30‐m distance corridor. The 6MWT is a simple, valid tool for testing the ability to perform daily life activities, e.g., walking; And Physical Activity Scale for the Elderly(PASE) addressed the participant’s physical activity level. Medical outcomes survey short form 36 (SF‐36) analyzes the participant’s health‐related quality of life (HRQOL) levels.
Results
The study participants' baseline socio‐demographic and clinical characteristics are summarized in Table 1. There were no differences between groups at the beginning of the study in any functional tests.There were significant improvements in the SPPB evaluations in the study group that improved their general physical performance at the end of 8 weeks. There was a significant improvement in the 6MWT for the study group and the STS‐10 test regarding physical functioning tests. Questionnaires showed a significant improvement in the PASE for both groups,and regarding HRQOL, the SF‐36 showed a significant improvement in quality of life and self‐care performance.
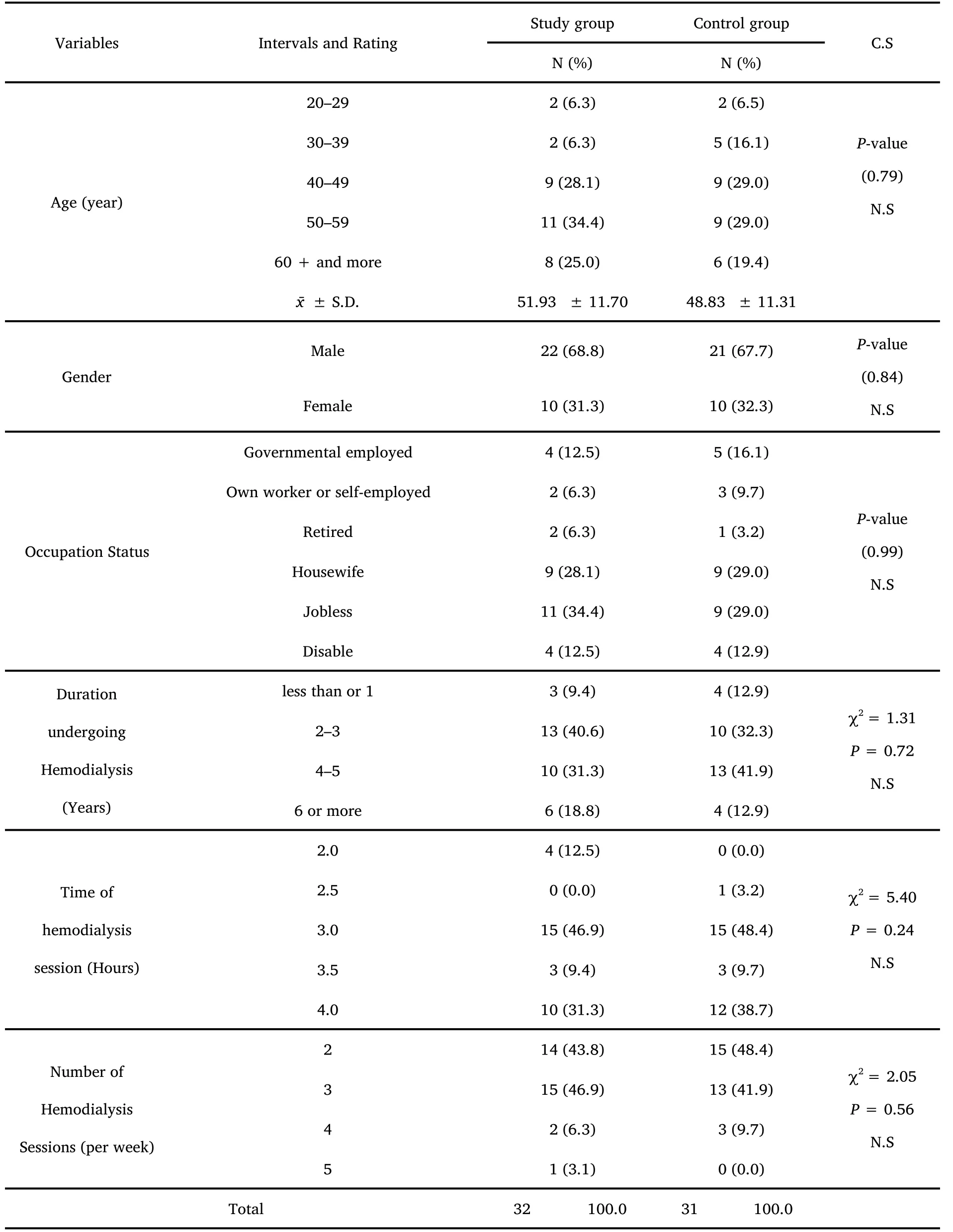
Table 1 Study and control groups baseline characteristic
Table 2 shows the comparison between the study and control group.SPPB scores were recorded before the study; physical performance was similar in both groups. Similarly, SPPB scores did not differ significantly between groups. The study results at post‐test indicate a highly significant difference, withP‐value less than 0.01. Figure 2 shows the mean difference in physical performance between groups,i.e., there were significant improvements in the SPPB evaluations in the study group that improved their general physical performance at the end of 8 weeks.
The effects of intervention programme on participants
Tables 3 and 4 display an STS‐10, STS‐60, 6MWT, PASE, HRQOL and perform self‐care behavior differences in the study sample (study and control group) pre and post evaluation. Table 4 shows a highly significant between the pre‐intervention and post intervention overall evaluation. Based on the mean of statistics, the study results indicate that the PASE, HRQOL, and perform self‐care behavior improved later in applying for the interventional program.
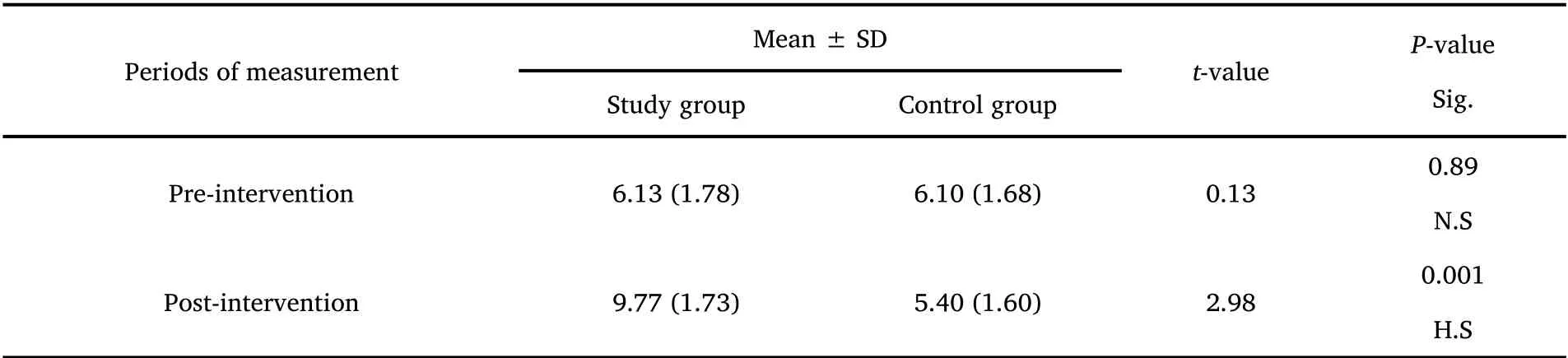
Table 2 Physical performance battery scores change (pre-Intervention- post-Intervention in two groups )
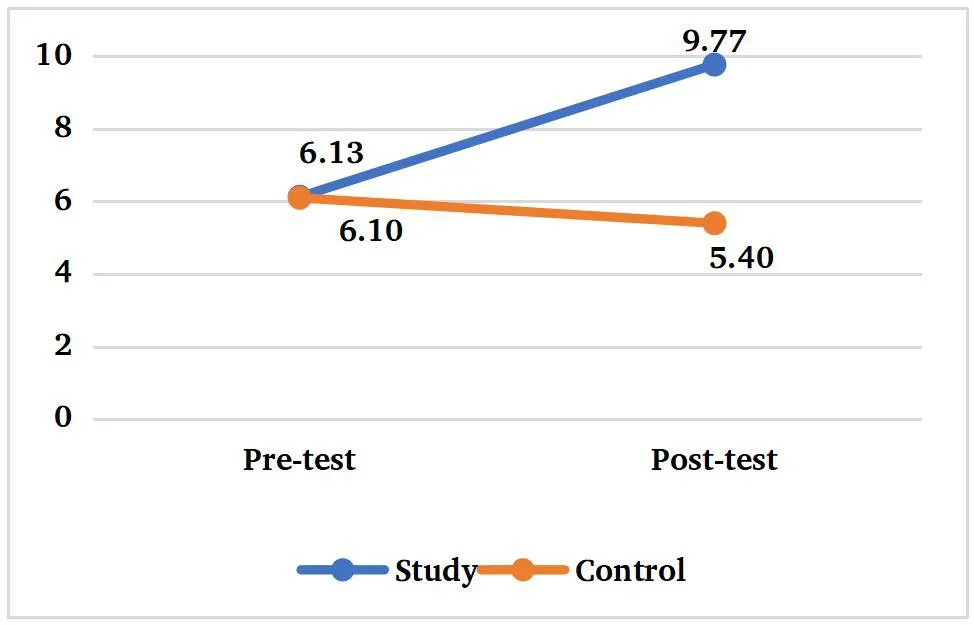
Figure 2 Mean of physical performance between groups
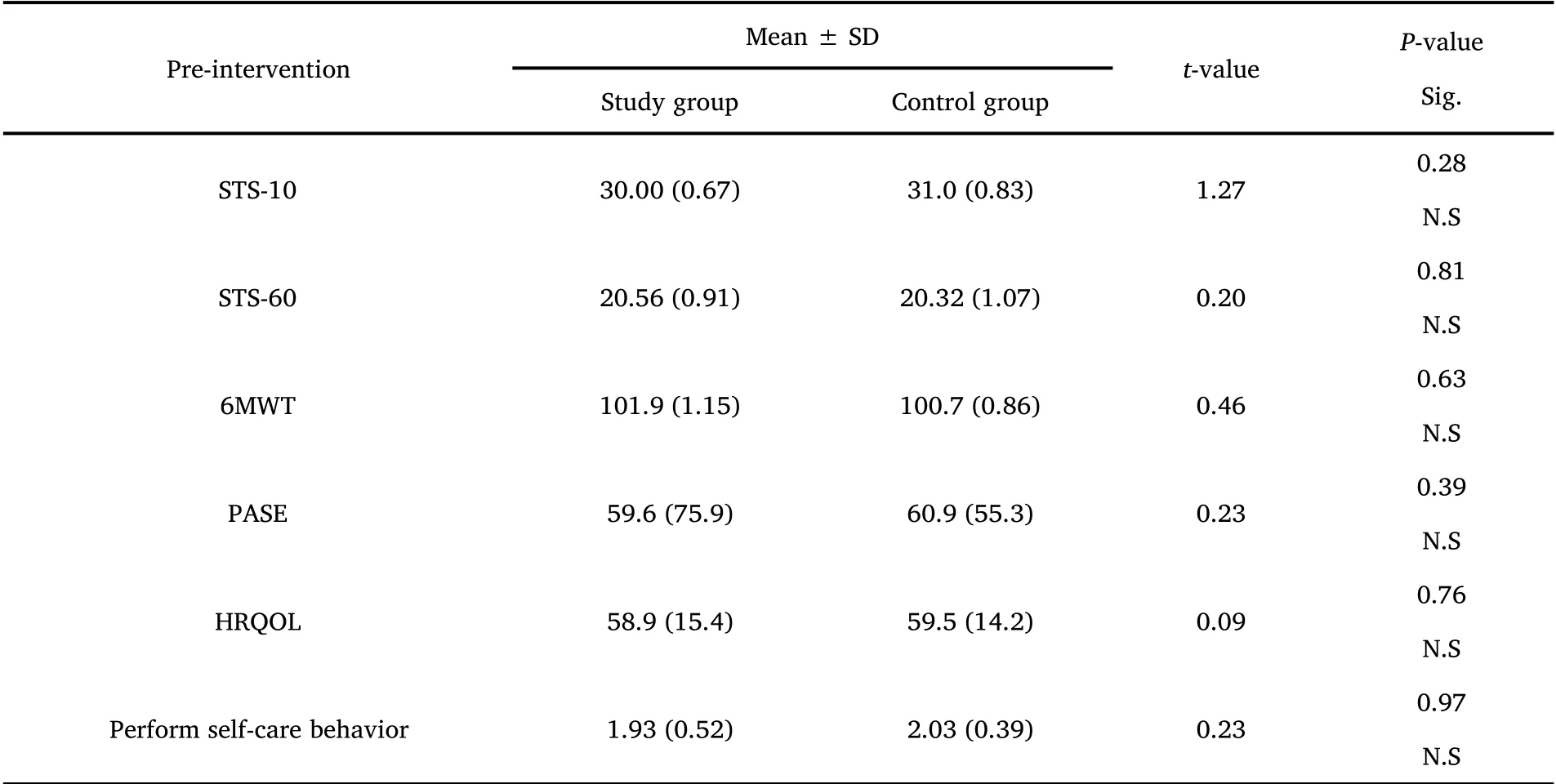
Table 3 Comparison of baseline evaluation between groups
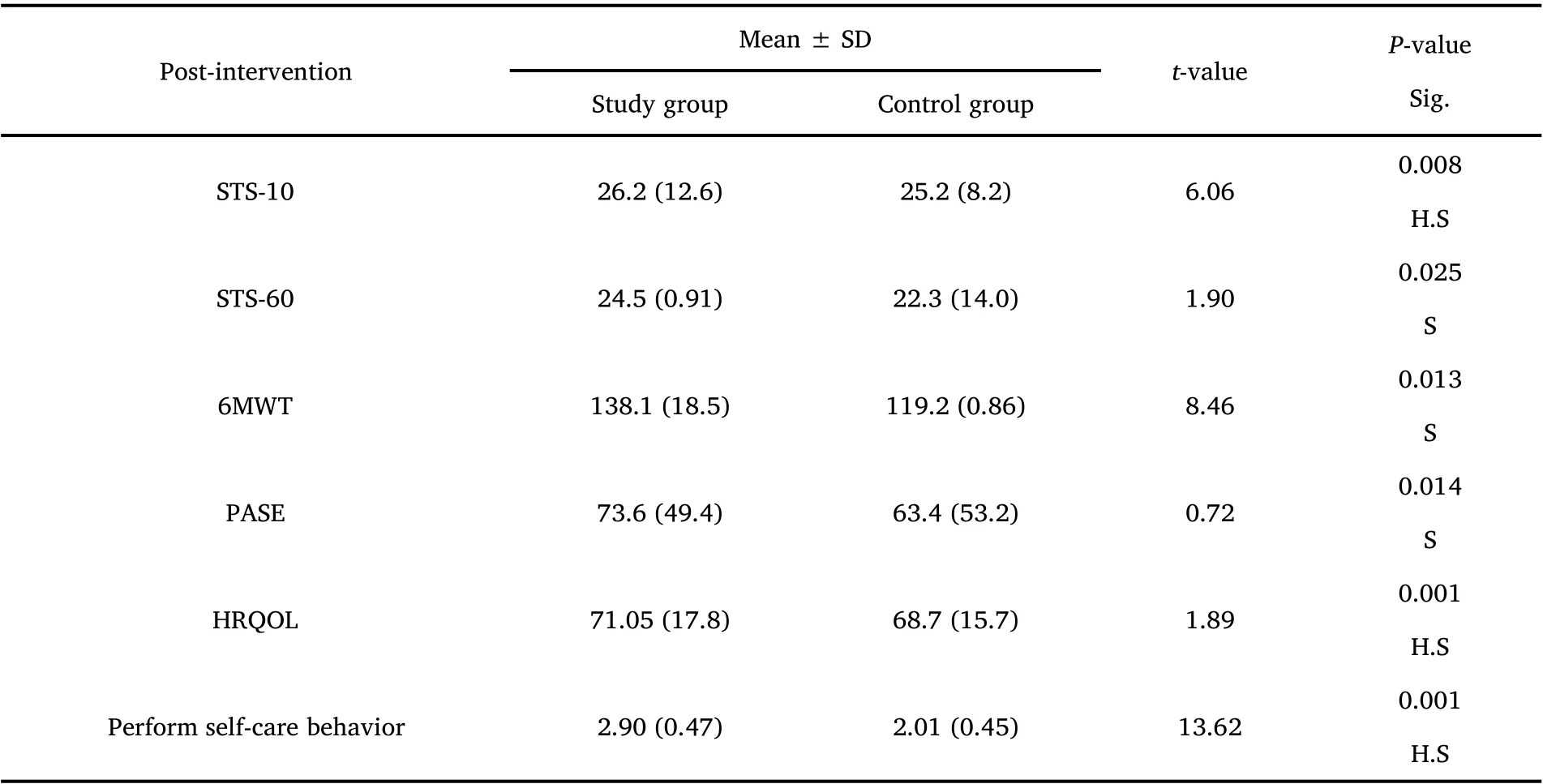
Table 4 Mean and standard deviation of pre-test and post-test STS-10, STS-60, 6MWT, PASE, HRQOL in two groups
Discussion
Exercise and physical activity are essential parts of lifestyle healthy for all adults, especially those in their early years [25]. However, new evidence suggests that resistance training can effectively reduce the risk of various chronic diseases. Most exercise or physical activity guidelines emphasize 75‐minute exercise weekly to decrease the risk of chronic diseases[26].
After applied of the intervention program of resistance exercise training through the current study, the present study results showed that after eight weeks of intervention, there are significant differences were found between groups (i.e., the applied method effectively improves patients' functional capacity, physical performance, and HRQOL of patients with ESKD and under hemodialysis treatment).This study highlighted the effectiveness of a multidisciplinary approach to exercise and indicated that trained nurses can implement exercise interventions and their daily job responsibilities [27].
Several studies had previously proven the beneficial effects of an exercise intervention in this population [28, 29] showed the impact of regular exercise training generally is associated with improved health outcomes in individuals with CKD, but in most of them, the intervention used aerobic training. Other studies [30, 31] used strength training as well. The study shows a significant improvement in the SPPB for the study group, similar to what Pu J [32] found in their study. This occurred even though our sample had high baseline values for this test, so there is an encouraging range of improvement for future studies. The study results agree with several other studies.Martins do Valle F conducted a randomized clinical study to evaluate the effectiveness of intradialytic resistance training on daily physical activity life and quality of life in patients undergoing hemodialysis[33]; and reported that resistance exercise training during hemodialysis was able to increase the capacity of physical.
In another multicenter retrospective observational study by [34], to evaluate the resistance training and strength of muscle and the relationship between physical function in patients undergoing regular hemodialysis, they stated that resistance training significantly improved patients' physical performance. Similar results were found in the 6MWT, a test widely used for functional capacity that also showed improvements in previous studies [35] with different exercise interventions, so we can understand that diverse exercise interventions have positive effects on these patients' functional capacity. Significant improvements were also found in the STS‐10 test for the intradialytic exercise group. Other studies used the STS‐10 [36,37] as well, finding improvements in their results.
Physical activity levels and HRQOL were assessed with the PASE and the SF‐36 questionnaires, respectively. Significant improvements for the study group were found,so the researcher can say that exercise interventions improved physical activity levels in patients with HD, as found in other studies [38]. In the SF‐36 significant and non‐significant improvements were found except for one of its subscales, and these results are similar to those who assessed the quality of life in these patients in other studies[39].
Propose Mcleod et al. [40] promoting the training of resistance exercise should be taken more seriously in training guidelines,especially for elderly people with chronic diseases. And in previous studies of scoping review, Asadzadeh et al. [41] conclusion: Exercise therapy has proved to be effective in improving rehabilitation results.Furthermore, regular physical activity can improve strength and endurance. Resistance exercises effectively increase the oxygen and nutrients delivered to tissues and contribute to improving cardiovascular performance. When the health of the heart and lungs improves, it increases the energy needed to deal with daily tasks. So,the physical performance will be increased. Implementing resistance training programmes has resulted in a significant improvement in all areas of physical performance. In addition, the results of study sample of the overall evaluation and based on means of the statistical, which improved, findings of study indicate that the physical activity levels,physical function, and quality of life improved as the longer the program is applied.
Conclusion
Exercise interventions at least eight weeks showed improving results involving functional capacity, physical performance, quality of life,and activity levels of end‐stage kidney disease patients and those undergoing hemodialysis compared with a control group. These results support the idea that performing exercise is more important,so we encourage therapists to implement exercise in their daily hemodialysis routine no matter the resources they can count on.
 Nursing Communications2022年13期
Nursing Communications2022年13期
- Nursing Communications的其它文章
- Delphi and Analytic hierarchy process for the construction of a risk assessment index system for post-stroke shoulder-hand syndrome
- A review of obstacles and facilitating factors of implementing Clinical Ladder Programs in nursing
- Spiritual health, empathy ability and their relationships with spiritual care perceptions among nursing students in China:A cross-sectional correlational study
- Qualitative study on influencing factors of refusal of gastric tube placement in stroke patients with dysphagia
- The influence of professional identity and ageism on turnover intention in nursing homes: a cross-sectional study from suzhou, China
- The relationship of family separation and nutrition status among under-five children: a cross-sectional study in Panti Public Health Center, Jember Regency of East Java, Indonesia