
The effect of compassion levels and empathic tendencies of intensive care nurses on quality of life:a cross-sectional study
2022-02-15 04:54SibelentrkErgMeltemMeri
Nursing Communications 2022年13期
Sibel ?entürk,Gül Ergün,Meltem Meri?
1Department of Nursing,Bucak School of Health,Burdur Mehmet Akif Ersoy University,Bucak-Burdur 15325,Turkey. 2Department of Nursing,Faculty of Health Sciences,Burdur Mehmet Akif Ersoy University,Burdur 15030, Turkey. 3Department of Nursing, Faculty of Health Sciences, Lokman Hekim University,?ankaya 06510,Turkey.
Abstract Objective: This study was conducted to determine the effect of compassion levels and empathic tendencies of intensive care nurses' on quality of life. Methods: This descriptive and cross‐sectional research study was completed with a total of 202 nurses. The data were collected using the Personal Information Form,Compassion Scale, Empathic Tendency Scale and Professional Quality of Life Scale. The data were analyzed using descriptive statistics,Student t test, Mann‐Whitney U test, Kruskal‐Wallis Test, One‐way analysis of variance(ANOVA), Spearman correlation and Multiple regression analysis. Results: As a result of multiple regression analysis, it was found that the variable of compassion(β= –0.263,P <0.01) had a negative and significant effect on the quality of life of employees; and the empathic tendency (β = 0.385, P <0.01) variable had a positive and significant effect on the quality of life of employees. Conclusion: As the compassion levels of intensive care nurses increase, their quality of life decreases; as their empathic tendencies increase, their quality of life also increases. Psychoeducation about compassion and empathy should be given to nurses who work in intensive care units with the aim of reducing compassion fatigue.
Keywords:intensive care nursing;compassion;empathy; quality of life
Background
Nursing is a profession that involves helping others and that relies on compassion and other universal values. Nurses perform their nursing roles using interpersonal communication techniques such as empathy.However, undesirable situations may arise from time to time due to nurses having too much empathy and this can lead to unprofessional behavior. When professional limits are exceeded, feeling empathy can be detrimental for the employee. Nurses are the healthcare professionals who have the most contact with the patient, and may sometimes experience stress in their working lives due to misplaced empathy. For a nurse who cannot cope with stress effectively, this situation may become chronic and turn into compassion fatigue [1].When nurses are helping a very traumatized patient, they sometimes unintentionally establish an intense emotional bond, identify with them and develop the idea that, “I am important, I am necessary for this patient”; they believe that if they are not there for the patient,there will be no one to help them [2]. Indifference to the patient,exposure to a traumatic situation, traumatic experiences gained as a result of working with patients, and a decrease in leisure time can all affect the development of compassion fatigue [3, 4]. The concept of compassion fatigue was first defined by Joinson in 1992. She stated that compassion fatigue occurs when nurses lose their nutritional abilities.It is stated that compassion fatigue is caused by working with people who have experienced a lot of trauma while having a powerful and private sense of empathy. Compassion fatigue has been observed to be more common among nurses working in units with critical patients, including hospice nurses and pediatric nurses, psychiatric nurses, community health nurses working with disaster victims,oncology nurses and emergency nurses and intensive care nurses[5‐8].
Professional quality of life concept consists of compassion satisfaction and compassion fatigue dimensions [5].It has been stated that professional quality of life is affected by various causes like traumatism, worry, life expectancy, high level empathy,developmental crises, coping with stress at work and health‐maintaining behaviors, professional resources, training programs, personal resting areas and hours, the clinic they work in,year of professional experience and age[5, 9].
When nurses’ levels of compassion are low, this may also cause a decrease in empathy and thereby reduce their professional quality of life. This study was carried out to identify the factors that affect the quality of life of the nurses who care for individuals in need of long‐term and complex care, such as intensive care, and to develop appropriate strategies for nurses to cope with this situation. There are various studies available in the literature on compassion fatigue,empathic and quality of life among nurses [7, 9‐12]. However, there are no studies in the literature in which nurses are studied in terms of these three concepts together. Therefore, it is thought that this study will guide other studies to be conducted. This study was conducted to determine the effect of compassion levels and empathic tendencies of intensive care nurses'on quality of life.
Methods
This is a cross‐sectional and descriptive study. The universe of the research consisted of all the intensive care nurses (220 nurses) who were working in the University Training and Research Hospital and the State Hospital between July and November 2019.The study aimed to reach the whole universe by not selecting samples, and a total of 202 people were reached. The percentage of participation in the research was 91.8%.The inclusion criteria were that the nurses(a)did not have communication and perception problems, (b) were working in intensive care units at the time of the study, and (c) agreed to participate in the study and signed informed consent. In order to conduct the study, the necessary ethics committee approval was received from the Burdur Mehmet Akif Ersoy University Ethics Committee (GO 2019/5).
Data collection tools
Nursing information form. The nursing information form included 24 questions about the nurses' features, “age, gender, marital status,education level, whether they had children, place of residence,employment unit, years of employment in the profession, time spent working in the intensive care unit, position, working style, weekly study period,whether they were satisfied with the work environment,whether they felt appreciated by their superiors,whether their anxiety level had increased in the intensive care unit, whether they put themselves in the place of the patient, how they thought their patients saw them, and their understanding of empathy”.
Compassion Scale (CS). The CS, consisting of 24 items, was developed by Pommier [13] in 2010. The Turkish validity and reliability study was conducted by Akdeniz and Deniz [14] in 2016.The scale is a 5‐point Likert type with 1=never and 5=always.The scale has six sub‐dimensions: kindness (items 6, 8, 16, and 24),indifference(items 2, 12,14,and 18), common humanity (11, 15,17,and 20), separation (items 3, 5, 10, and 22), mindfulness (items 4, 9,13, and 21) and disengagement (items 1, 7, 19 and 23). The indifference, separation and disengagement sub‐dimensions of the scale are reverse‐scored.The average total score is then taken [15]. In cases that require the sub‐dimensions to be analyzed separately,reverse‐scoring is not carried out. On the scale, 24 means the lowest score and 120 means the highest score.The increase in the total score indicates an increase in the level of compassion. In the study of Akdeniz and Deniz15 the Cronbach’s alpha value of the scale was 0.85.In our study,it was determined to be 0.88.
Empathic Tendency Scale (ETS). The ETS is defined as a concept that includes the attitudes and behaviors of individuals about feeling and expressing empathy. The ETS was developed by D?kmen in 1988 and aims to evaluate individuals' potential to establish empathic relationships in daily life[15]. The scale is 20‐item and 5‐point Likert type (1 = “completely contradictory”, 2 = “highly contradictory”, 3= “unstable”, 4 = “fairly appropriate”, 5 = “entirely appropriate”).Eight items of the scale (3, 6, 7, 8, 11, 12, 13, and 15) are inversely stated. The lowest score that can be obtained from the scale is 20,and the highest score is 100. Higher scores from the scale indicate that individuals' empathic tendencies are also higher. In 1988, D?kmen20 determined the correlation coefficient for reliability as r = 0.82, and Cronbach's alpha value was 0.88.
Professional Quality of Life Scale (ProQOLS). The ProQOLS, which was created by Stamm in 2005, was added to the Turkish literature in 2010 by Ye?il et al. [16, 17]. The scale has three sub‐dimensions, 30 items and 6‐point Likert type ("Never" (0) to "Very often" (5).“Compassion satisfaction” (items 3, 6, 12, 16, 18, 20, 22, 24, 27, and 30) is the first of the sub‐scales and it expresses the feeling of content and satisfaction experienced by the employee for helping others with an issue related to their profession. The high scores of this sub‐dimension indicate that it creates a high level of satisfaction when helping someone else. The Cronbach’s alpha reliability value of the original scale was 0.87, while it was 0.83 in our study. The second subscale, "burnout", (items 1, 4, 8, 10, 15, 17, 19, 21, 26, and 29) is used to determine burnout caused by helplessness and difficulties in coping with problems in the working environment. As the score obtained from the subscale increases, the level of burnout also increases. The Cronbach’s alpha reliability value in the original scale was 0.72, while it was 0.64 in our study. The third subscale,"compassion fatigue", (items 2, 5, 7, 9, 11, 13, 14, 23, 25, and 28) is used to evaluate symptoms due to a stressful situation.Employees who score high in this scale are encouraged to get support or help. The Cronbach’s alpha reliability value in the original scale was 0.80,while it was 0.84 in our study. In evaluating the scales, items 1, 4, 15, 17,and 29 are scored in reverse. It has been reported that the scale is an effective measurement tool in data collection especially for occupational groups working under intense stress.
Data analysis
Statistical evaluation was made using the NCSS (Number Cruncher Statistical System) 2007 (Kaysville, Utah, USA) program. Descriptive statistics and Shapiro‐Wilk test were used to analyze the data. In addition, One‐way ANOVA and Student T Test in normal distribution,Kruskall‐Wallis and Mann‐Whitney U tests in non‐normal distribution were used. Spearman correlation analysis and multiple linear regression analysis were used to define the relationship of quantitative data. The significance level was set atP<0.01 andP<0.05 for all statistical tests.
Results
While 68.3% (n=138) of the participants were under the age of 30,23.3%(n=47)of them were between the ages of 30 and 39 and 8.4%(n=17)of them were in the 40‐and‐above group of age.While 76.7%(n = 155) of the participants were women, 23.3% (n = 47) of them were men. While 48% (n = 97) of the participants were working in general intensive care, 12.4% (n = 25) of them were working in coronary intensive care, 5.4% (n = 11) in neonatal intensive care,7.4% (n = 15) in cardiovascular surgery (CS) intensive care, 0.5% (n= 1) in pediatric intensive care, 17.3% (n = 35) in anesthesia intensive care, and 8.9% (n = 18) were working in other units.While 70.3% (n = 142) of the participants chose the profession willingly,29.7% (n = 60) of them chose it unwillingly. While 61.4% (n =124)of the participants were working in intensive care willingly, 11.9% (n= 24) of them were working unwillingly and 36.7% (n = 54) were working partly willingly. While 30.2% (n = 61) of the participants were happy with their professional life, 24.8%(n = 50) of them were not happy with it, and 45% (n = 91) were partially happy. While 71.8% (n = 145) of the participants believed that an intensive care unit reduces the quality of life, 28.2%(n =57) of them did not.
A statistically significant difference was found among the compassion scale scores by age groups (P=0.025;P<0.05). The compassion score of the group aged 40 and over was higher than the other age groups (P= 0.001;P<0.01). The compassion score of the group women is higher than men (P= 0.001;P< 0.01). The compassion score of the group who chose the profession willingly was found to be higher than the group who chose the profession unwillingly (P= 0.001;P< 0.01). It was found statistically significant that the compassion score of the group which believed that the intensive care unit reduces the quality of life was lower than that of the group which believed that it does not (P= 0.001;P<0.01)(Table 1).
A statistically significant difference was found among the quality of life scores by intensive care units(P=0.002;P<0.01).The fact that the quality of life scores of people who were working in anesthesia intensive care unit was lower than the scores of those who were working in the general intensive care unit was found to be statistically significant (P= 0.001;P<0.01) (Table 1).
The ETS scores showed statistically significant differences according to whether the nurses were working willingly in intensive care units(P= 0.016;P<0.05). The empathic tendency score of the group that worked willingly was higher than that of those who worked partly willingly (P= 0.001;P<0.01). The empathic tendency scores showed statistically significant differences according to professional satisfaction (P= 0.006;P<0.01). The empathic tendency score of the group that was more satisfied with their profession was higher than those who were partially satisfied (P= 0.001;P<0.01) (Table 1).
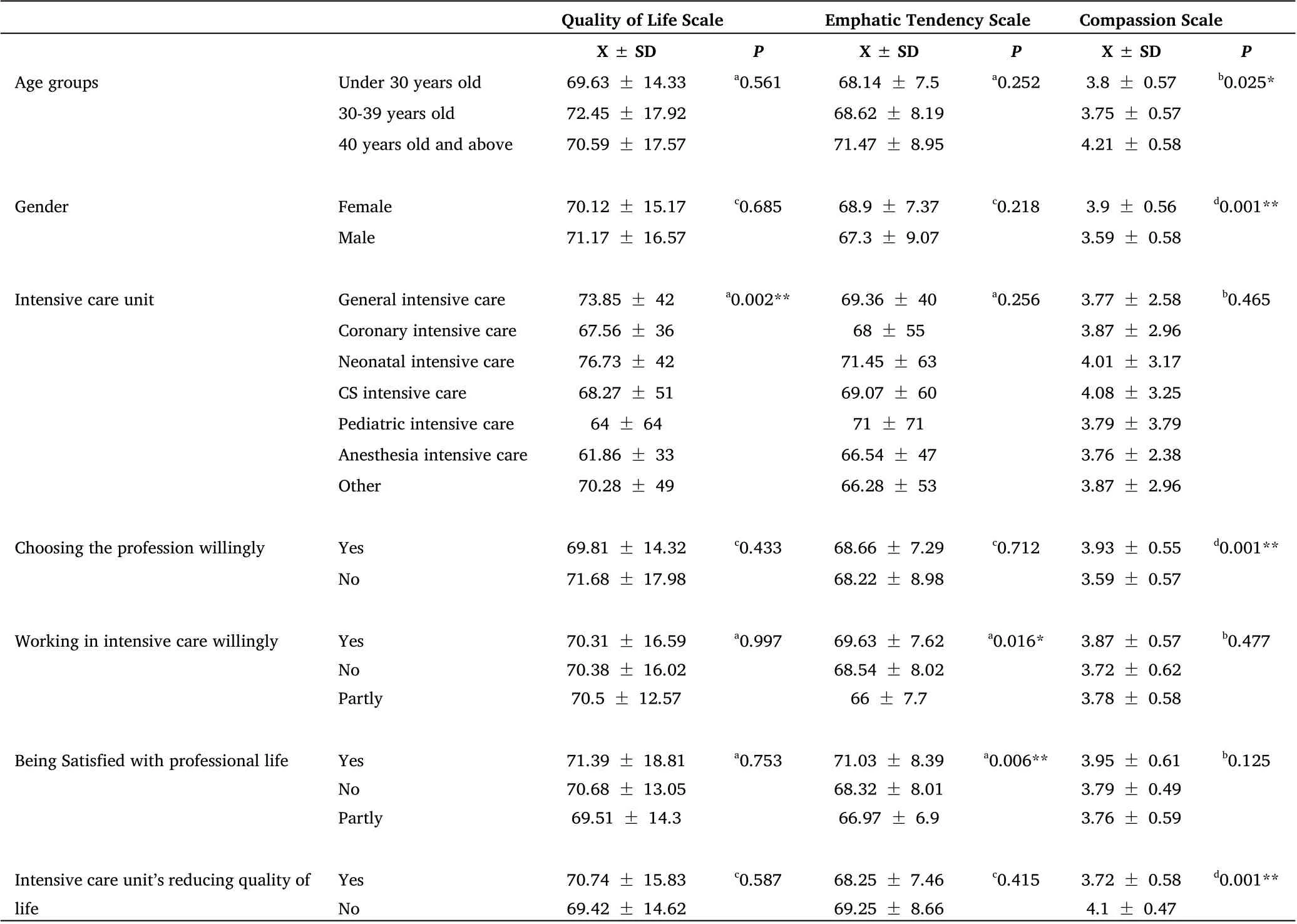
Table 1 Analysis of sociodemographic data according to scales
It was determined that there was a positive and moderately significant relationship among compassion satisfaction and ProQOLS(r = 0.405;P<0.01). It was determined that there was a positive moderately significant relationship among compassion satisfaction and the compassion scale (r =0.405;P<0.01). It was determined that there was a negative and moderately significant relationship among burnout and indifference (r = –0.403;P<0.01). It was determined that there was a negative and moderately significant relationship among burnout and the CS (r = –0.447;P<0.01).
It was determined that there was a positive and a very high level of significant relationship among compassion fatigue and ProQOLS (r =0.878;P<0.01).It was determined that there was a positive and very weak level of significant relationship among compassion fatigue and the ETS (r = 0.190;P<0.01). It was determined that there was a positive and weak significant relationship among ProQOLS and ETS (r= 0.295;P<0.01). It was determined that there was a negative and very weak level of significant relationship among ProQOLS and the compassion scale(r=–0.161;P<0.01).It was determined that there was a positive and weak significant relationship among ETS and CS (r= 0.290;P<0.01) (Table 2).
According to the correlation analysis between scales, it was determined that there was a positive and weak significant relationship among ProQOLS and ETS (r = 0.295;P<0.01). It was determined that there was a negative and very weak level of significant relationship among the ProQOLS and the CS (r = –0.161;P<0.01).It was determined that there was a positive and weak significant relationship among the ETS and the CS (r = 0.290;P<0.01).
Examining the relationships between the sub‐scales of the ProQOLS and the other scales, it was determined that there was a positive and moderately significant relationship among compassion satisfaction and the CS (r = 0.405;P<0.01). It was determined that there was a negative and moderately significant relationship among burnout and the CS (r = –0.447;P<0.01) (Table 2).
When Table 3 is analyzed, the multiple linear regression analysis performed to define the effect of compassion and empathic tendency on the professional quality of life found that these effects were statistically significant (F (2.199) = 19.973,P<0.01).The variables of compassion and empathic tendency in the model explain 17%of the total variance in professional quality of life (R2 = 0.17,P<0.01).When the regression coefficients are reviewed, it can be observed that the variable of compassion(β=–0.263,P<0.01)had a negative and significant effect on professional quality of life. The variable of empathic tendency (β = 0.385,P<0.01) appeared to have had a positive and significant effect on professional quality of life. As the scores for compassion increase, the professional quality of life scores decrease; as the empathic tendency scores increase, the professional quality of life scores also increase.
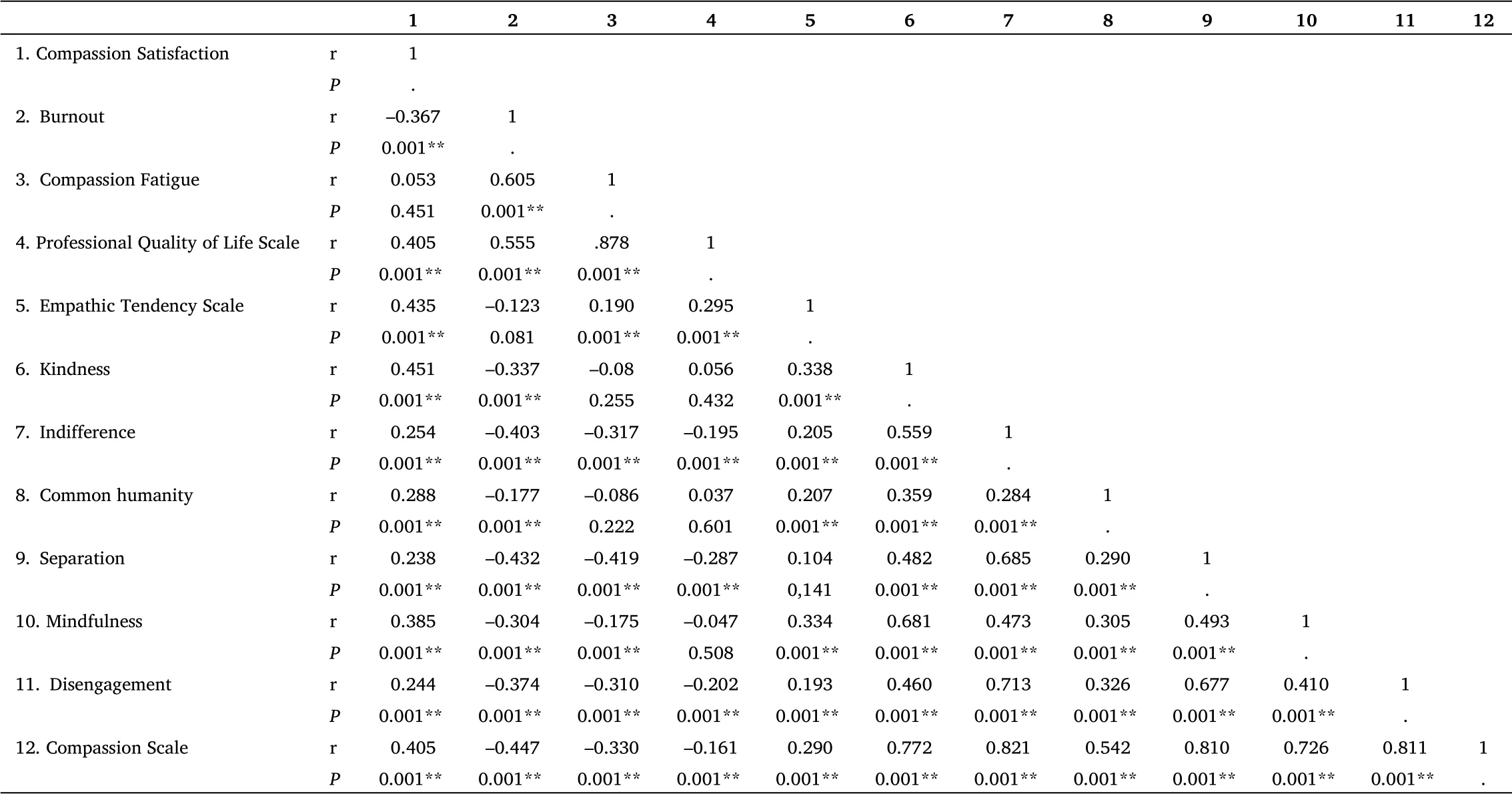
Table 2 Cross-scale correlation analysis

Table 3 Simple linear regression analysis findings on employee regression on quality of life
Discussion
Intensive care nurses are happy to provide compassionate care to patients and their families and to show an empathetic approach.However, nurses are at risk of compassion fatigue. The balance between satisfaction and fatigue expresses professional quality of life.The imbalance between these two concepts negatively affects the quality of life of intensive care nurses[6,7,8].This research indicated that there was an effect of compassion levels and empathic tendencies of intensive care nurses' on quality of life.
In this study,found that the level of compassion in females is higher than that in males. Similar to our study, the literature has found that the level of compassion in females is higher than that in males [8].Women are sensitive, compassionate and matronly by nature [18].Women are more emotional and compassionate as a result of hormonal factors as well [19]. This result in the current study may have arisen due to the fact that women are able to integrate these innate characteristics into all areas of their lives. In the present study,as in most studies in the literature, the level of compassion increased with age[20,21].The sense of compassion of a nurse,who constantly sees the problems and the pain that patients encounter, increases over time; this causes nurses to feel compassion fatigue and burnout [5].Those who chose the profession willingly had high compassion scores.Nursing is generally chosen because it seems an easy and guaranteed form of employment [22]. Nurses who have chosen the profession willingly may be more affected by the patients they encounter and their traumatic experiences. This may cause them to grow more compassionate. The level of compassion of those who believed that intensive care units reduced their quality of life was found to be low.Those nurses who do not enjoy working in an intensive care unit, and who feel that their quality of life is decreasing, may have developed defense mechanisms in order to protect their mental health.Traumatic experiences,pain and loss are often experienced in intensive care units caring for critically ill patients. Therefore, compassion fatigue may be experienced more by the nurses who work in these units [23].However, sometimes nurses isolate themselves from this environment and hide their feelings of compassion. The results of the current research may be indicative of that process. Among the intensive care units,the quality of life of nurses working in anesthesia intensive care units was the lowest. In the literature, it is emphasized that nurses who work in intensive care units have a lower quality of life than the nurses who work in other units [24]. In some studies, it has been reported that nurses who work in units that require both intensive and more acute intervention, such as anesthesia intensive care and emergency medicine, have a low quality of life due to the many stressful situations they have to face[12, 25]. In the current research,the quality of life of anesthesia intensive care nurses may have been low for reasons such as the presence of critical patients,which leads to more stressful conditions.
In the current research, the empathic tendencies of the nurses who worked willingly in intensive care were high. This was an expected result. A person who does a job willingly can fulfill the requirements of that job more easily. A nurse who works willingly in intensive care will tend to use empathy, which is one of the most effective communication techniques, and see it as a requirement of the profession. Intensive care nurses are more sensitive than nurses in units for patients who need support to identify and meet their immaterial needs,which is part of holistic care[26].Just as the nurses who have willingly chosen the unit they work in have high levels of empathy, those who are satisfied with their professional life also have high empathy.These situations reinforce each other positively.As well as being useful in planning nursing interventions suitable for each patient's condition, empathy enables the nurse to see positive developments in the patient and achieve professional satisfaction[21]. Among intensive care and emergency service nurses,professional satisfaction is reported to be less due to both the intensity of the work and the working conditions, and the characteristics of the patients they care for [11]. Therefore, nurses with higher empathy levels can be expected to be selected by the managers to work in emergency services and intensive care units [27].
A nurse who is happy in their unit will have a high‐quality professional life. In this situation, it is likely that the nurse's empathy will increase. Likewise, as the empathy increases, so the quality of the nurses’ professional life will also increase as they receive positive feedback from patients and team members [12]. The increase in the empathic tendency levels of the participants indicates that the nurses use empathy, which is one of the therapeutic communication techniques, and behave more professionally. And these professional behaviors lead to a higher quality of professional life for the nurses[28]. Sometimes nurses are faced with diseases and situations that require very heavy workloads, lack of materials, and empathic abilities. Although empathy is one of the core values for the nursing profession, if it is not used correctly, it may have harmful results for nurses [10]. In our study, as the professional quality of life of the nurses’ increases, the scores they obtained from the CS decreased.After some time, nurses who feel too much compassion may experience burnout and fatigue owing to the internalization of all the distress and pain experienced by the patients and their families. On the other hand, an increase in compassion leads to a move away from professional communication techniques, an increased inability to protect themselves from harmful emotions and ultimately, to compassion fatigue [7, 9, 10, 20]. Especially in intensive care units with patients who are critical, compassion fatigue and the associated decrease in quality of life are experienced very frequently.Compassion fatigue caused by excessive compassion in healthcare workers and especially in nurses is frequently mentioned in the literature, and it has been found that compassion fatigue is observed more frequently in oncology and intensive care units(ICUs)[3,4,11].It was determined that there was a positive and weak significant relationship among the ETS and the CS indicates a different point. A nurse who has an empathetic approach is also compassionate at the beginning. However, a nurse who goes beyond what is professionally required may over time lose the ability to be empathic. Thus, the nurse may encounter burnout and compassion fatigue. The relationship between these two concepts reveals the importance of nurses’ learning compassion and empathy during their education. In their study, Richardson and Hughes determined that teaching these two concepts increases productivity in professional life [28].
It has been found that compassion satisfaction is associated with increase in compassion. This, though, is a situation that may cause risks for the nurse if too much emphasis is placed on it, just as with empathy and compassion.It is natural for nurses who feel compassion to experience compassion satisfaction from the feedback they receive[4]. However, problems may arise in the compassion satisfaction of nurses due to compassion fatigue faced as a result of feeling too much compassion [29]. In this case, burnout, which is another sub‐dimension of quality of life, will come into play. In the current research, as the nurses’ feelings of burnout increased, their sense of compassion gradually decreased. The nurse may thus enter a vicious circle in which psychopathologies such as anxiety, burnout syndrome and depression develop [30]. According to the multiple regression analysis, the level of compassion had a negative effect on the quality of life. It was found that as the level of compassion in increased, the quality of life decreased. However, many factors mentioned above have an effect on this. If nurses who work in the intensive care units do not use professional communication techniques effectively, they gradually become less professional, and internalize the pain of their patients and their families [11, 24]. The physical and psychological burnout of nurses who work in intensive care units, and are responsible for the care of patients with high levels of emotional and physical pain, thus increase, while their quality of life decreases [19,23].The present study identified positive effects on quality of life from the increase in the nurses' empathic tendencies. Empathy is one of the primary structures that form the basis for connection between those who need help and those who can provide it. If nurses bear a constant emotional load, even though they may take steps to practice self‐care,their feelings of empathy may lead to a sense of suffocation and being overburdened [31]. Moreover, high levels of empathy can be a risk factor for compassion fatigue, whereas self‐compassion may often be protective. Therefore, it is important to teach self‐compassion and self‐care in interventions aimed at reducing burnout and compassion fatigue and improving quality of life [10].
As the nurses' compassion scores increased, their quality of life scores decreased. As their emphatic tendency scores increased, their professional quality of life scores also increased. In this study, we can say that we have found the following: the effective use of empathy,which is one of the professional communication skills, by those nurses who are responsible for the care of patients with critical conditions in intensive care, prevents them from feeling compassion at a level that leads them to become less professional, and increases their professional quality of life.
In line with these results, the researchers present the following recommendations: it is important that nurses learn about these concepts in communication lessons while they are still students; that curricula in universities be revised in this direction; that psychoeducation about these concepts be developed, with the aim of teaching nurses’ self‐compassion and self‐care skills to reduce compassion fatigue; and that more comprehensive qualitative studies be planned to deeply explore compassion levels, empathic tendencies,quality of life and relationships among nurses who work in different units.
Study limitations
The research has some limitations. The results cannot be generalized since the research was conducted in the intensive care units of the hospitals. The other limited aspect of the study is that the data of the study was collected during the working hours of the nurses, which may have caused the nurses to fill out questionnaires quickly due to time pressures and the intensity of work. In order to support the results of the research, studies with larger samples are needed.
Conclusion
Compassion and empathy are important concepts for patient care in intensive care units. As the intensive care nurses' compassion scores increased, their quality of life scores decreased. As their emphatic tendency scores increased, their professional quality of life scores also increased. Understanding the situations to increase the quality of professional life can contribute positively to the working environment of nurses working in intensive care. Therefore, attempts can be made to improve the standards of working environments. Moreover,psychoeducation about compassion and empathy should be given to nurses who work in intensive care units with the aim of reducing compassion fatigue and policies should be developed for the personnel who may develop compassion fatigue by the hospital management. It is recommended to support nurses with evidence‐based studies.
 Nursing Communications2022年13期
Nursing Communications2022年13期
- Nursing Communications的其它文章
- Delphi and Analytic hierarchy process for the construction of a risk assessment index system for post-stroke shoulder-hand syndrome
- A review of obstacles and facilitating factors of implementing Clinical Ladder Programs in nursing
- Spiritual health, empathy ability and their relationships with spiritual care perceptions among nursing students in China:A cross-sectional correlational study
- Qualitative study on influencing factors of refusal of gastric tube placement in stroke patients with dysphagia
- The influence of professional identity and ageism on turnover intention in nursing homes: a cross-sectional study from suzhou, China
- The relationship of family separation and nutrition status among under-five children: a cross-sectional study in Panti Public Health Center, Jember Regency of East Java, Indonesia