
Nurse manager’s perception about clinical supervision at Madinah Hospitals in Saudi Arabia
2022-02-15 04:54AwatifOmarAlhawsawiAmenhMohammadAlahmdiSaharMohammedAly
Nursing Communications 2022年13期
Awatif Omar Alhawsawi,Amenh Mohammad Alahmdi,Sahar Mohammed Aly
1Faculty of Nursing,Umm Alqura University,Alabdiyah 24382,Saudi Arabia.
Abstract Aim: The present study assesses the nurse managers’ perception of clinical supervision.Method: A cross‐sectional, descriptive, non‐experimental quantitative research design was utilized in three governmental hospitals in Madinah Munawara city for a purposive sample of different levels of nurse managers (n = 84) by using a questionnaire. Results: The total knowledge of nurses managers regarding clinical supervision domains, where 59.5% of participants had a high level of knowledge, with mean ± standard deviation (47.262 ±11.151). The highest mean was in the clinical supervision – facilitating learning domain(18.464±4.155),with 69%of participants having a high level of knowledge regarding this domain. Safety and quality in the clinical supervision domain represent the lowest mean of knowledge (4.607 ± 1.628). The level of total skills of nurses managers regarding clinical supervision domains, where 54.8% of participants had a high level of total skill while the range 19–60, with mean ± standard deviation was (44.167 ± 8.958). The highest mean was in the clinical supervision –facilitating learning domain(17.405 ±3.671),with 48.8%of participants having an increased knowledge of this domain. Safety and quality in the clinical supervision domain represent the lowest mean of skills(3.952 ± 1.270),with more than half 58.3% of nurse managers having average skills in the same domain. Conclusion:In the Al‐Madinah region, there is no single policy or system of clinical supervision; rather,it is based on the needs of each organization. Clinical supervision should be handled appropriately and supportive. Hospital management should offer proper training for newly appointed first‐line nurse managers with adequate, regular, and timely feedback on their strengths and weaknesses in their skills. Clinical supervision should be taught as a separate curriculum in nursing administration courses. Hospital managers should create a system,culture and environment that fosters high ethical standards and competent clinical monitoring. The right to supervision, feedback, help, appropriate working circumstances,and respect must be guaranteed to trainees and supervisors in this system.
Keywords:nurse manager; perception;clinical supervision;Saudi Arabia
Background
Nurse managers play an essential role in fostering a healthy work environment, ensuring favorable patient outcomes, and achieving organizational objectives. However, developing crucial skills for success is sometimes overlooked, and new nurse managers face challenges as they move from clinical care to nursing leadership [1].Clinical supervision is a standard protocol of professional support,reflection, and learning that aids in the growth of individuals. Nurses,as a whole, work with patients who are likely to be in bodily and/or psychological discomfort, which can create demand and strain them,both testing and cumulative. Clinical supervision can help young and seasoned health professionals in their day‐to‐day jobs [2]. Clinical supervision has been pushed as a critical component of clinical governance to ensure the provision of and accountability for the quality of care provided to patients and reduce the risk of poor outcomes.Thus managers and employees face difficulty enhancing the quality of care in practice. Moreover, first‐line nurse managers are widely regarded as the most important connection in the nursing department. In addition, clinical supervision, according to many nurses and nurse managers,will be their most important responsibility in the future. As a result, most of the head nurse’s tasks centre around managing,developing,and maintaining the unit’s staff nurses’morale,interest and satisfaction [3].
Clinical supervision is a process that gives isolated time and an opportunity to further improve the supervisee’s skills and knowledge within an ongoing professional relationship, usually with an experienced practitioner or peers, for post‐qualification health professionals. Clinical supervision’s goal is for the supervisee to participate in guided reflection on current practice to improve and grow it in the future [4]. Empathetic supervisors are more effective because they understand their subordinates’ motivations and can modify their tactics to match their requirements.They also know how to give constructive criticism and encouragement while being supportive. Clinical supervisors should also be active, open and constructive in assisting supervisees in effectively exploring and developing clinical practice, as well as allowing them to openly discuss clinical and critical issues, as the culture of the clinical discussion appears to be evolving in a more open and directed manner[3].
Clinical supervision worldwide provides healthcare services to individuals, families and communities, helping them achieve optimal health [5]. They coordinate health care and support patients so that they can take care of themselves. Nurses and nurse managers have a lot to consider, and many are dealing with multiple crises at the same time. When nurses have other things on their minds, it’s too easy to lose sight of the need for clinical supervision.With clinical supervision in Arab nations, nurses are already overburdened, so finding time to listen to and respond to their experiences can be difficult[6].
Nursing services will advance because of good supervision. This is because implementing nurses will feel accepted, respected, and involved, resulting in a high dedication to developing nursing services. Clinical supervision increases clinical knowledge, personal confidence, greater interrelationships, professional development and support. The possibility of improving the quality of care is being studied [3]. The use of clinical supervision was explored and discovered to be a beneficial and fascinating technique. The reasons for this were its effectiveness and potential for resolving clinical practice obstacles among nurses, including burnout, a lack of knowledge and skills, and problems with staff relationships[7].
In addition, clinical supervision in Saudi Arabia is frequently ineffective because supervisors defer to their facility’s authority structure rather than engaging in open discourse with their employees[7]. Clinical supervision became a vital aspect of the management style in Kingdom of Saudi Arabia, resulting in staff members growing and flourishing on the job over time. Most studies on supervisory training, expanding supervisory standards and evaluating the supervisory process are conducted in counselling, psychotherapy, and other mental health services, so the importance of good clinical supervision was becoming more apparent within healthcare institutions [8]. Supervisors should be able to recognize specific nursing practices and encourage health professionals in their professional roles,continuous professional development, and ensuring patient safety and high‐quality care. They should also focus on the needs of their employees to deliver the best possible outcomes. To overcome obstacles, overcome challenges, and create a healthy work atmosphere, effective clinical supervision is required (according to AAl, 2015).
Furthermore, good clinical supervision allows for the transfer of skills and knowledge between the supervisor and supervisees,potentially improving the quality of patient treatment. In conclusion,while are studies that implement, measure,and evaluate the impact of clinical trials available. There is a scarcity of evidence focusing on supervisory programs Almadani (2019). So, assessment of knowledge and skills of clinical supervision is urgently needed in Saudi Arabia.The present study will assess the perception and knowledge of nurse managers regarding clinical supervision at Madinah hospitals in Saudi Arabia.
Methods
Study setting
This study was directed at three governmental hospitals in Madinah Munawara city in the Kingdom of Saudi Arabia operated by the Ministry of Health. The Saudi central board accredits all the hospitals for accreditation of healthcare institutions. The first hospital is King Fahad hospital which is the reference hospital of the Madinah region.It is in the city’s northwest area and provides value‐based healthcare services. It is accredited by Joint Commission International Accreditation as well.It consists of five floors with a 500 bed capacity.The second hospital is Ohud hospital which is in the environs of Madinah Munawara. It is located in the western part of the city. It consists of two floors with 280 beds capacity. The third hospital is Miqat hospital, located southwest of the city. It consists of two floors with 64 beds capacity. All the hospitals provide various medical services, including emergency, critical care and outpatient healthcare services.
Sampling
The study’s population was divided into two categories: the target population and the accessible population. The complete set of persons or things to whom the researcher seeks to extrapolate from a study’s findings is referred to as the target population. The target population comprises persons or objects that fulfill the researcher’s criteria.Using a random selection method technique to create a sample from a population’s members or elements is known as probability sampling or random sampling.
Sample method
The researchers selected a non‐probability sampling method by purposive sampling of nurse managers working in three hospitals.The sample elements are picked from the population using nonrandom procedures in nonprobability sampling. Nonrandom sampling methods are more prone to provide a skewed method than random sampling methods. Despite the drawbacks of sampling with a low probability, it is used in most nursing research projects. In nursing research, true random samples are uncommon [9]. The subjects for purposeful sampling are chosen by hand. Judgmental sampling is another name for this strategy. Participants may be recruited for the study if the researcher or an expert believes they represent the accessible population. This sampling method is founded on the fact that the examiner or designated proficient has sufficient knowledge of the study’s target population to select specific individuals from a defined population today [9].
Sample size
The study sample was calculated according to the total population,which is 122 sample was calculated electronically through https://goodcalculators.com/sample‐size‐calculator by using the following formula [10]: [z2*p* (1–p) / e2]/ [1 + (z2*p* (1–p) /(e2*N))] (https://goodcalculators.com/sample‐size‐calculator).
However, the number of participants who answered the electronic questionnaire was 84 participants with 90.3%responses.
For a quantitative investigation, there are no easy guidelines for establishing the appropriate sample size. The similarity of population,the grade of accuracy needed by the investigator, and the sampling process to be utilized are all considerations. A small number of samples may be enough if the group is similar or identical on all variables except the one being measured.Therefore if the investigator needs to be extremely accurate when creating a generalization about the population based on sample data, a high sample size may be required. Finally, smaller samples are necessary when using probability sampling methods rather than nonprobability sampling approaches [11].
Inclusion and exclusion criteria
The participants’ criteria to be enrolled in this study were the nursing staff occupying a managerial position, willing to participate voluntarily and agree by signing the consent, and understanding English to answer the questionnaire. In contrast, the participants excluded from the enrollment of this study are new managers under training or orientation or with less than one year of experience.
Instrument of data collection
The researchers used the electronic self‐administrative questionnaire form as a tool for the current study.It consists of two parts:
Part I Socio‐demographic characteristics: the researchers designed the questions of this part to include five items: gender, nationality,qualification, years of experience and working place.
Part II Clinical Supervision Self‐Assessment Tool (CSAT‐knowledge and CSAT‐skills).
The Clinical Supervision Self‐Assessment Tool is based on the basic clinical supervision competencies stated in Health Workforce Australia’s National Clinical Supervision Competency Resource(2014). It is used to assess knowledge, skill and confidence.
Both CSAT‐knowledge and CSAT‐skills are divided into six domains:prepare and plan (3 items), facilitating learning contains (12 items),problem‐solving (4 items), communication (4 items), safety and quality (3 items) and organization (4 items). In this study, two axes were adopted: skills and knowledge; confidence was excluded, with a total number of 30 items for each axis for knowledge and skills. The response was measured using a scale including Yes (2), with support(1) and No (0).
A two‐phase prospective study was carried out. During phase 1, the Clinical Supervision Self‐Assessment Tool was enhanced, and content validity and pilot testing were conducted on the upgraded version during phase 2. Phase 2 included the psychometric assessment of the updated Clinical Supervision Self‐Assessment Tool (MCSAT‐skills;MCSAT‐knowledge). The MCSAT‐knowledge and MCSAT‐skills portions had 30 items. The content validity of the MCSAT was assessed to be satisfactory in response to the expert panel’s assessment. The exploratory factor analysis revealed a three‐factor structure:measuring clinical learning,facilitating clinical learning and problem‐solving. Each of the three criteria was assessed separately.Cronbach’s alpha scores exceeded 0.90, indicating a high level of internal consistency. The construct validity of clinical supervision training was demonstrated by the fact that nurses who had completed it scored much higher on clinical supervision knowledge and skill assessments than those who had not [12].
The link for the study tool represented in the electronic questionnaire was distributed through social networking sites, email and various social media used by the study population to collect data related to the study.
Reliability and validity
The current study’s researchers assessed questionnaire reliability based on internal consistency. Cronbach alpha is > 0.90. An instrument’s stability reliability refers to its consistency throughout time. The total Alpha value for CSAT‐knowledge (0.959) and CSAT‐skills (0.90). The questionnaire was tested for validity by academic and nursing administration experts. The jury’s opinions and suggestions recommended no modifications.
Data collection procedure
The study tasks were distributed between the two researchers. The study approval of Institutional Review Board (IRB) forms was filled and reviewed by both authors. The 2nd author submitted the forms due to the proximity of the distance. While waiting for the study’s approval, both authors decided on the research design to be utilized.The 1st author designed the demographic data questionnaire,blended the tool items, and formed the final design of the questionnaire.
After the study’s approval was obtained from IRB. The 2nd author created the questionnaire link through google Forms, visited the selected hospitals, and met the nursing directors to explain the research objectives, the manner of data collection, the study population, the ethical considerations, and answer any questions inquires related to the study. The directors of nursing were friendly and requested to participate in testing the questionnaire’s validity.
The nursing directors published the questionnaire link among the nurse managers through WhatsApp and emails. Then 2nd author visited the hospitals to contact the directors to encourage their nurse managers to fill out the questionnaire. The questionnaire remained accessible for six weeks. After that, the questionnaire’s electronic link was locked, and the data obtained from the questionnaire’s responses were conveyed to an Excel sheet and kept in a locked folder on the personal device of the researchers. The excel sheet had been sent to the statistician by the 1st author.
Ethical considerations
This study is approved by Institutional Review Board at the general directorate of health affairs in Madinah(IRB 014‐22).The respondents are assured that no threats or coercion will be encountered while conducting this study, and they can freely withdraw whenever they want. Above all, informed, voluntary consent was distributed at the beginning of the questionnaire, so each participant requested to agree before participating for autonomy assurance.The participants’privacy is respected.Additionally,the responses to the study questionnaire are electronic. The names of the participants were optional to maintain their information’s confidentiality.
Data analysis
The research will use the SPSS 25 statistical program to analyze the data obtained through the questionnaire using the following methods:frequencies, percentages, mean, standard deviation, chi‐square,analysis of variance and Pearson correlation.
The study used Chi‐square to compare percentages in all domain points and used a T‐test to explain the relationship between knowledge and (gender, nationality) and so on with total skills. We used the analysis of variance(ANOVA) test to explain the relationship between knowledge and (qualification, years of experience and working place) with total skills. We used the Pearson correlation to explain the correlation between knowledge and skill.
Definition of research keywords
The important terms used have been defined to understand this study better. The following terms are: 1.Clinical supervision. It is a method of encouraging, monitoring, and directing an individual or group of people as a professional. Clinical supervision is the “formal provision of relationship‐based education and training by accredited supervisors that focuses on work and manages, supports, develops, and assesses the work of colleagues in a hospital” [13]. 2. Nurse manager. In a clinical context, someone with administrative responsibilities supervises the staff nurses [13]. 3. Perception. Perception refers to nurses’ beliefs, viewpoints, and understanding of the nursing profession because of their previous and current training experiences[14].
Results
The participants’ professional and demographic information is summarized in Table 1.Among the total subjects,79.8%were female,92.9% were Saudi, 76.2% had Bachelor’s, 44% had hospital work experience of 5‐10 years, 47.6% worked in King Fahad, and 34.5%from Ohud.
Table 2 show the level of total knowledge of nurses managers’regarding clinical supervision domains, where 59.5% of participants had a high level of total knowledge while the range 22–60,with mean± standard deviation (SD) were (47.262 ± 11.151). The highest mean was in the clinical supervision – facilitating learning domain(18.464 ± 4.155). With 69% of participants had a high level of knowledge regarding this domain. While safety and quality in the clinical supervision domain represent the lowest mean of knowledge(4.607 ± 1.628). More than half 59.5%) of nurse managers have a high level of knowledge regarding the same domain.
Table 3 show the level of total skills of nurses managers’ regarding clinical supervision domains, where 54.8% of participants had a high level of total skill while the range 19–60., with mean ± SD was(44.167 ± 8.958). The highest mean was in the clinical supervision –facilitating learning domain (17.405 ± 3.671). With 48.8% of participants had a high level of knowledge regarding this domain. In contrast, safety and quality in the clinical supervision domain represent the lowest mean of skills (3.952 ± 1.270). More than half 58.3% of nurse managers have average skills in the same domain.

Table 1 Demographic and professional characteristics of the participants

Table 2 Mean and standard deviation of nurse managers’clinical supervision knowledge domains
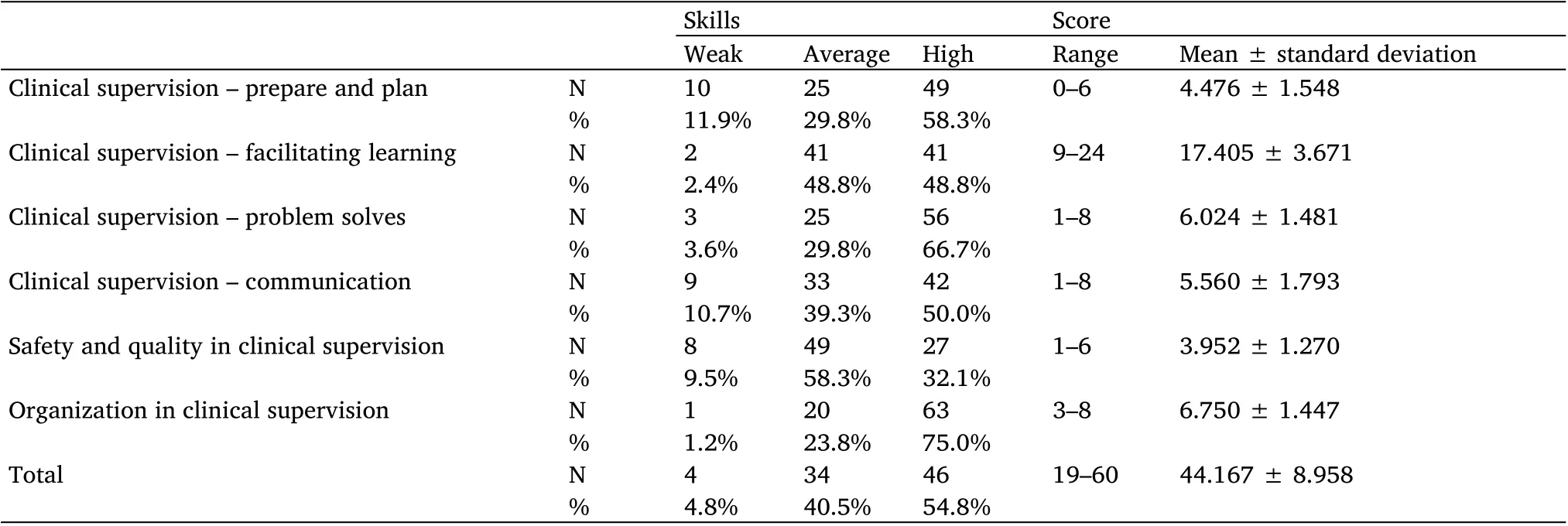
Table 3 Mean and standard deviation of nurse managers’clinical supervision skills domains
Table 4 show that is a significant between total knowledge and working place (increase in Ohud hospital) where F = 41.559 andP‐value=0.000 less than significant level 0.05 and this significant we can see it from difference between means the mean ± SD for Ohud hospital (55.483 ± 7.125). But no significant relation with other variables (gender, nationality, qualification and years of experience)where allP‐values more than a significant level of 0.05.
Table 5 show that is a significant between total Skills and working place (increase in Ohud hospital) where F = 16.966 andP‐value =0.000 less than the significant level of 0.05 and this significant we can see from difference between means the mean ±SD for Ohud hospital(49.034 ± 76.248). But no significant relation with other variables(gender, nationality, qualification and years of experience) where allP‐values more than significant level of 0.05.
Table 6 and Figure 1 show that is a significant positive correlation between knowledge and skills for each domain:(clinical supervision –prepare and plan, clinical supervision – facilitating learning, clinical supervision – problem‐solving, clinical supervision – communication,safety, and quality in clinical supervision and organization) where allP‐value <0.001*and the correlation coefficient’s equal 0.820, 0.809,0.783,0.648, 0.684, 0.891 and 0.855 with respectively.
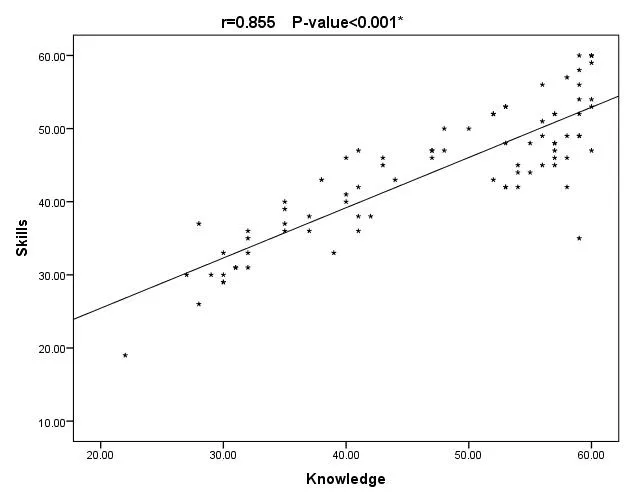
Figure 1 The relation between nurse managers’ knowledge and skill for each domain
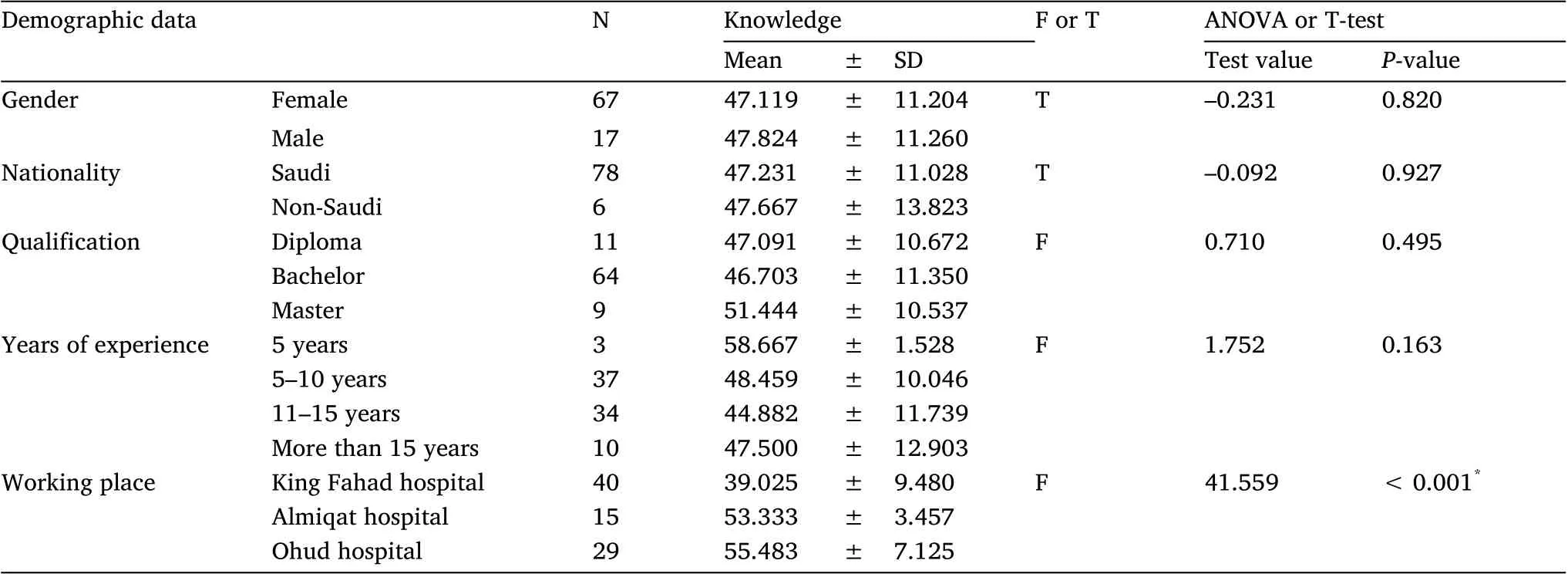
Table 4 The relation between nurse managers’knowledge and demographic data
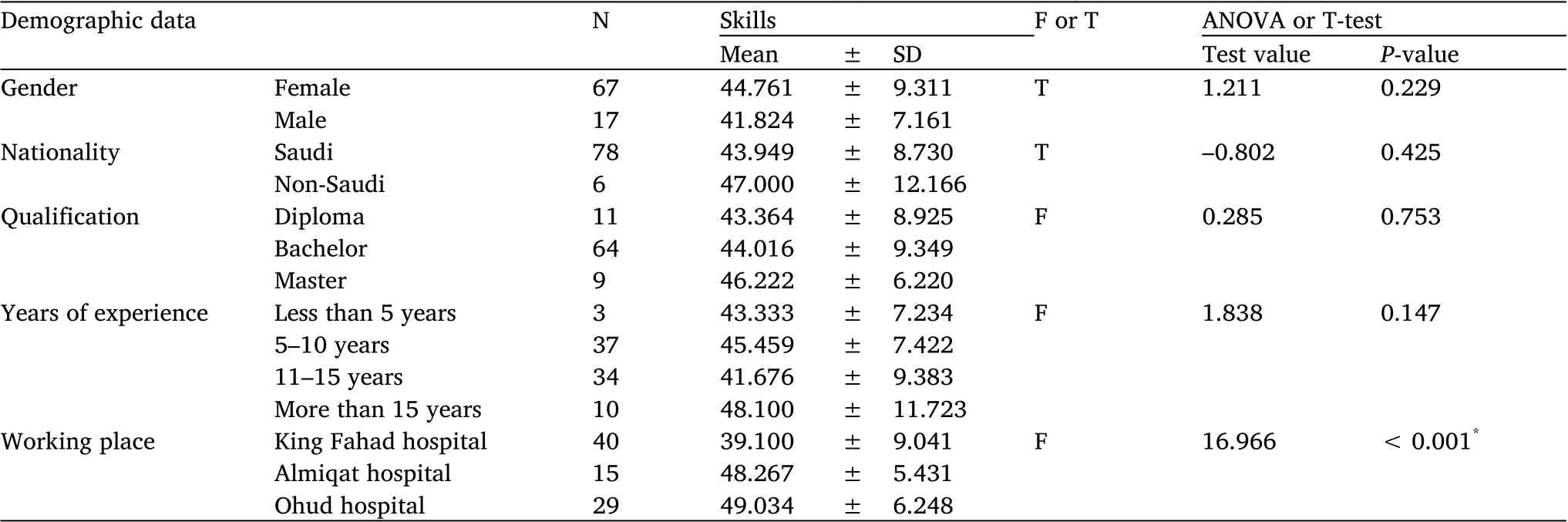
Table 5 The relation between nurse managers’skills and demographic data

Table 6 The correlation between nurse managers’ knowledge and skills for each domain
Discussion
Clinical supervisors are crucial in ensuring the quality of care,enhancing patient care, and monitoring the professional development of staff nurses [15]. The present study assesses the nurse managers’perception of clinical supervision. Table 2 presented the level of total knowledge of nurses managers’ regarding clinical supervision domains, where more than half of the participants had a high level of total knowledge. Furthermore, the total knowledge of head nurses regarding clinical supervision improved statistically considerably immediately after the program and three months after the program compared to their knowledge before the program. According to the results, the level of overall practice among head nurses improved statistically significantly before and within three months of the program’s introduction [16]. It was found that training in clinical supervision improved work performance in terms of clinical supervision abilities. In recent years, nurse education has enhanced the overall quality of healthcare services, particularly nursing care[17].
Table 2 and Table 3 presented that the highest mean was in the clinical supervision – facilitating learning domain of knowledge and skills.This finding could be explained in the light that individuals and groups can benefit from using educational tools to help them learn more successfully. Nurses have the chance to engage in critical discussion about professional practice in a supportive setting, where they can question, reflect, and explore topics. This result is supported by Achempim‐Ansong, et al., who reported that clinical supervision had been shown to improve effective learning [18]. With good supervision, supervisees become more focused and willing to learn,resulting in improved results. More competent, knowledgeable and skilled. Clinical supervisors must work with health professionals to enhance their knowledge, skill, and attitude to continue graduating safe and qualified health professionals. According to the literature,feedback enhances student engagement with learning,achievement of clinical competence, and involvement with self‐evaluation, whereas insufficient or improper feedback might stymie student growth [19].
One of the many benefits of clinical supervision is stress reduction.Other benefits include problem‐solving skills, change management,and increased prioritization. Competing for work needs, staffing challenges, and the duration, location, and supervision procedure were all obstacles that had to be overcome.It was suggested that more time be added to the allotted supervision hour, that participants be aware of peer group clinical supervision in advance, and that experts be trained as supervisors [20].
While safety and quality in the clinical supervision domain represent the lowest mean of knowledge and skills. Clinical supervision is critical when it comes to the development of non‐technical abilities and patient safety competencies in nurse specialist students. Finding the time to reflect on and learn from the supervision; on the other hand, it was thought to be difficult. In addition, half of the students said they didn’t have enough time to supervise their peers [21]. Clinical supervisors must give students critical knowledge, skills, support and encouragement, while the placement organization must negotiate and arrange student semester breaks and the preceptors’ general schedule[22].
Table 4 and Table 5 revealed a considerable gap between total knowledge, skills, and working environment (increase in Ohud hospital). Nurse Managers who have worked in Ohud hospital had a higher degree of clinical supervision knowledge and abilities than nurse managers in other hospitals. This could be due to the establishment of a strong education department and equal opportunities for nurse supervisors at the Ohud hospital to attend intensive courses focused on enhancing knowledge and skill based on their specific needs.
Figure 1 discovered a positive association that is statistically significant between knowledge and skills for each domain (clinical supervision – prepare and plan, clinical supervision – facilitating learning, clinical supervision – problem‐solving,clinical supervision –communication, safety, and quality in clinical supervision and organization link between head nurse knowledge and skills.This study result is in the same line as those ElZeneny, et al. and El‐Rahman and El‐Hessewi[23,24].
Limitations
This study was conducted using a sample of managers from Al‐Madinah Al‐Manwarh, which may limit the generalizability of the finding.
In addition, there were inadequate responses to the questionnaire,which affected the completion of the research sample due to the long questionnaire,the workload of nurse managers during COVID‐19, and the delay in obtaining ethical approval for data collection. The delay in obtaining approvals to start collecting data had an impact on the search result. There is a lack of recent research studies on the topic.
Due to time constraints, the study used a self‐administered questionnaire, relying on self‐reported replies, just as students have deadlines to turn in their class assignments. As a result, the reactions could have been altered by the passage of time. There were 30 questions in total, divided into six sections. Given that nurses were required to complete the questionnaire on top of their regular workload, it’s possible that the tool’s length, combined with the participants'competing interests, constrained response rates.
Recommendation
Ministry of health could develop specific and unified policies and standards for the practice of clinical supervision in healthcare organizations,taking into account familiarity with clinical supervision knowledge and skills.
Ministry of education can approve clinical supervision as a separate curriculum in nursing administration courses.
Hospital administrators may construct a system, environment, and culture that promotes competent clinical oversight that guarantee supervisors the right to practice supervision starting from supervisors’selection criteria and conducts educational activities to keep the supervisors updated about clinical supervision.
Conclusion
Nurse managers’ total knowledge and skills in clinical supervision domains,with more than half of the participants having a high level of total knowledge and abilities. There is no unified policy or clinical supervision system in the Al‐Madinah region’s ministry health hospital,but it is biased on each organization’s needs.
For each domain (clinical supervision – prepare and plan, clinical supervision – facilitating learning, clinical supervision –problem‐solving, clinical supervision – communication, safety and quality in clinical supervision and organization), there is a positive correlation between knowledge and skills. These findings emphasize the importance of continuing education and developing tools to assist nurses who oversee nursing students. Continuous professional growth and training are required to support such initiatives.Other approaches can potentially improve nurses’clinical knowledge,abilities,and skills in clinical supervision.
 Nursing Communications2022年13期
Nursing Communications2022年13期
- Nursing Communications的其它文章
- Delphi and Analytic hierarchy process for the construction of a risk assessment index system for post-stroke shoulder-hand syndrome
- A review of obstacles and facilitating factors of implementing Clinical Ladder Programs in nursing
- Spiritual health, empathy ability and their relationships with spiritual care perceptions among nursing students in China:A cross-sectional correlational study
- Qualitative study on influencing factors of refusal of gastric tube placement in stroke patients with dysphagia
- The influence of professional identity and ageism on turnover intention in nursing homes: a cross-sectional study from suzhou, China
- The relationship of family separation and nutrition status among under-five children: a cross-sectional study in Panti Public Health Center, Jember Regency of East Java, Indonesia