
Health literacy, behavioral and psychosocial characteristics in coronary artery patients: A hospital-based study in Turkey
2022-02-18 08:10:56AsumanAhciogluGulayYilmazel
Journal of Acute Disease 2022年1期
Asuman Ahcioglu, Gulay Yilmazel
Public Health Department, Hitit University, ?orum, Turkey
ABSTRACT
KEYWORDS: Coronary artery disease; Health literacy; Risk-factors;Patients
1. Introduction
Globally, non-communicable diseases (NCDs) were responsible for 71% of the deaths, and 43.6% of these deaths were due to cardiovascular diseases (CVD) in 2021[1]. It is predicted that CVD will continue to be the first cause of death worldwide for a long time[2]. It has been reported that the burden of NCDs is also rising in Turkey, 89% of all deaths resulted from NCDs, and the highest proportion of these deaths (34%) were due to CVD[2]. Considering Turkey's NCD profile, multiple behavioral factors seem to lead to an increase in the incidence of these diseases[2-4].
A high increase in NCDs has made societies responsive to decision-making in health-related issues. For NCDs, the ability to keep up with modern healthcare systems and navigate in a complex structure has made health literacy compulsory. Health literacy acts as a bridge in preventing NCDs and controlling the risk factors[4].
Health literacy is defined as gaining health competence in the field of acquiring, understanding, and using health-related information[4,5]. However, lack of health literacy has existed in many European countries[6-8] which is increasingly recognized as a serious, public health concern and is the main cause of unwillingness to disease prevention, early diagnosis, and treatment adherence[4,9].
Limited health literacy is a risk factor of NCDs [asthma, chronic obstructive pulmonary disease (COPD), kidney diseases, etc.][10,11]. Coronary artery disease (CAD) is a common disorder characterized by insufficient blood and oxygen for heart muscle due to the accumulation of plaque in the coronary arteries that requires a holistic bio-psychosocial evaluation and requires adequate health literacy[12,13]. A primary concern of CAD is mental health problems which are explicitly mentioned[13,14].
CAD requires a range of self-care skills based on collaboration between the patient, healthcare system, and service providers[12,15].Increasing the quality of life in these patients depends on the ability to prevent possible comorbidities and sequels, adherence to the treatment and diet regimen, and to manage the self-care process. Patients with CAD are expected to take an active role in disease management and develop interactive partnerships with care providers. Adequate health literacy skills can play an important role in meeting all these expectations. Even though several studies examined the health literacy levels of different groups in our country[16,17], one major issue is a gap in the literature on limited health literacy, psychosocial and behavioral factors among CAD patients. The present study aims to examine the health literacy level and associated factors among CAD patients.
2. Patients and methods
2.1. Study design
This descriptive and correlational study was carried out in a state hospital in the Western Black Sea Region of Turkey from March 2019 to March 2020.
2.2. Study population
The study population consisted of hospitalized patients diagnosed as any CVDs [including atrial fibrillation (AF), ventricular tachycardia (VT), supraventricular tachycardia (SVT), heart failure(HF)] in the cardiology service and coronary intensive care unit.Based on the knowledge that the sufficient health literacy level in our country is 25%[7], the minimum sample size was calculated as 245 in 80% power and 95% confidence. Eligibility criteria required patients to have received CAD treatment excluding AF, VT, SVT, HF. Other criteria for selecting the patients were as follows: Literate, aged ≥50 years, without vision, hearing, speech and psychiatric disorders,and speaking Turkish. The study was completed with 275 voluntary CAD patients.
2.3. Data collection
The study was conducted in the form of a questionnaire, with data being gathered via face-to-face interview method (Supplementary materials). The response time of the questionnaire took an average of 30 min.
2.4. Questionnaire
The design of the questionnaires was based on the literature[12].The questionnaire has been divided into two parts.
2.4.1. First part
The first part deals with socio-demographic, clinical, behavioral,and psychosocial characteristics.
Individual-level variables covered socio-demographic characteristics, self-perception of health, self-perception of medical material skills, health system utilization, body mass index (BMI),smoking (responses were “never, quit, currently”) and alcohol consumption (responses were “never, quit, currently”) and physical activity.
Clinical characteristics including comorbidities, family history of CAD, kinds of CAD, history of angiography and by-pass surgery,and duration of hospitalization were obtained from patient files in clinics.
Psychosocial items focused on the depression symptom level. Beck Depression Inventory was adapted to Turkish in 1989 with a 0.80 Cronbach alpha coefficient[18]. It is used to determine the severity of depressive feelings in adults. The scale consists of 21 items, and each item scores between 0-3, which varies between 0-63. The calculated result points indicate the severity of depressive symptoms.
(0-9) points: Normal level
(10-18) points: Mild level depression
(19-29) points: Moderate level depression
(30-63) points: Severe depression.
In the present study, the severity of depressive symptoms was grouped into three groups as normal, mild, and moderate/severe. In this study, Cronbach's alpha coefficient was 0.82.
2.4.2. Second partThe second part was concerned with health literacy including Turkey Health Literacy Scale-32 (TSOY-32).
TSOY-32 was developed to assess health literacy among people with literate and ages>15 years. Based on the conceptual framework developed by the European Health Literacy Research Consortium[19]the scale was translated into Turkish and its validity and reliability studies were carried out by Okyay et al. (Cronbach alfa=0.927)[7].
Each item in the scale consists of 32 points in total and it consists of 4 degrees: 1=Very difficult, 2=Hard, 3=Easy, 4=Very easy. On the scale, 0 points indicates the lowest health literacy and 50 points indicates the highest[7].
Health literacy level was evaluated in four categories according to the total scores:
(0-25) points: Inadequate health literacy Percentage and mean values were used in the evaluation of research data; Chi-square test and Fisher's Exact test were used in the comparison of categorical variables. Multilevel logistic regression analysis was used to determine the effective changes in health literacy levels. Adequate health literacy level was handled as the dependent variable in logistic regression analysis. The significant level of this study was set at α=0.05.
(>25-33) points: Problematic-limited health literacy
(>33-42) points: Adequate health literacy
(>42-50) points: Excellent health literacy
In the present study, the health literacy levels of the participants were examined in two categories: Limited (0-33 points) and adequate (34-50 points). In this study, the Cronbach alpha coefficient was 0.895.
2.5. Ethical approval
The study was planned following the Helsinki Principles and Ethics Committee Approval was obtained from the Ethics Committee of Hitit University (2019-85).
2.6. Statistical analysis
The data of the study were collected using the SPSS 20.0.
3. Results
Of the study group, 59.6% were in the 50-64 age group with mean age of 61.8 years (95% CI: 50-74). Among the respondents, 81.5%were male, 68.0% had low education level (primary school and under level) and 82.9% were married. Table 1 presents the health literacy levels of the patients according to socio-demographic characteristics.
The health literacy index score was 31.7 in the whole group and the prevalence of limited and adequate health literacy was 59.3%and 40.7% respectively. Limited health literacy was more common among older participants (≥65 years old). Health literacy levels differed significantly according to age groups (χ2=53.384, P<0.001)(Table 1).
Gender was also associated with the level of health literacy. Theprevalence of adequate health literacy was 62.5% for men and 37.5% for women (χ2=44.940, P<0.001) (Table 1).
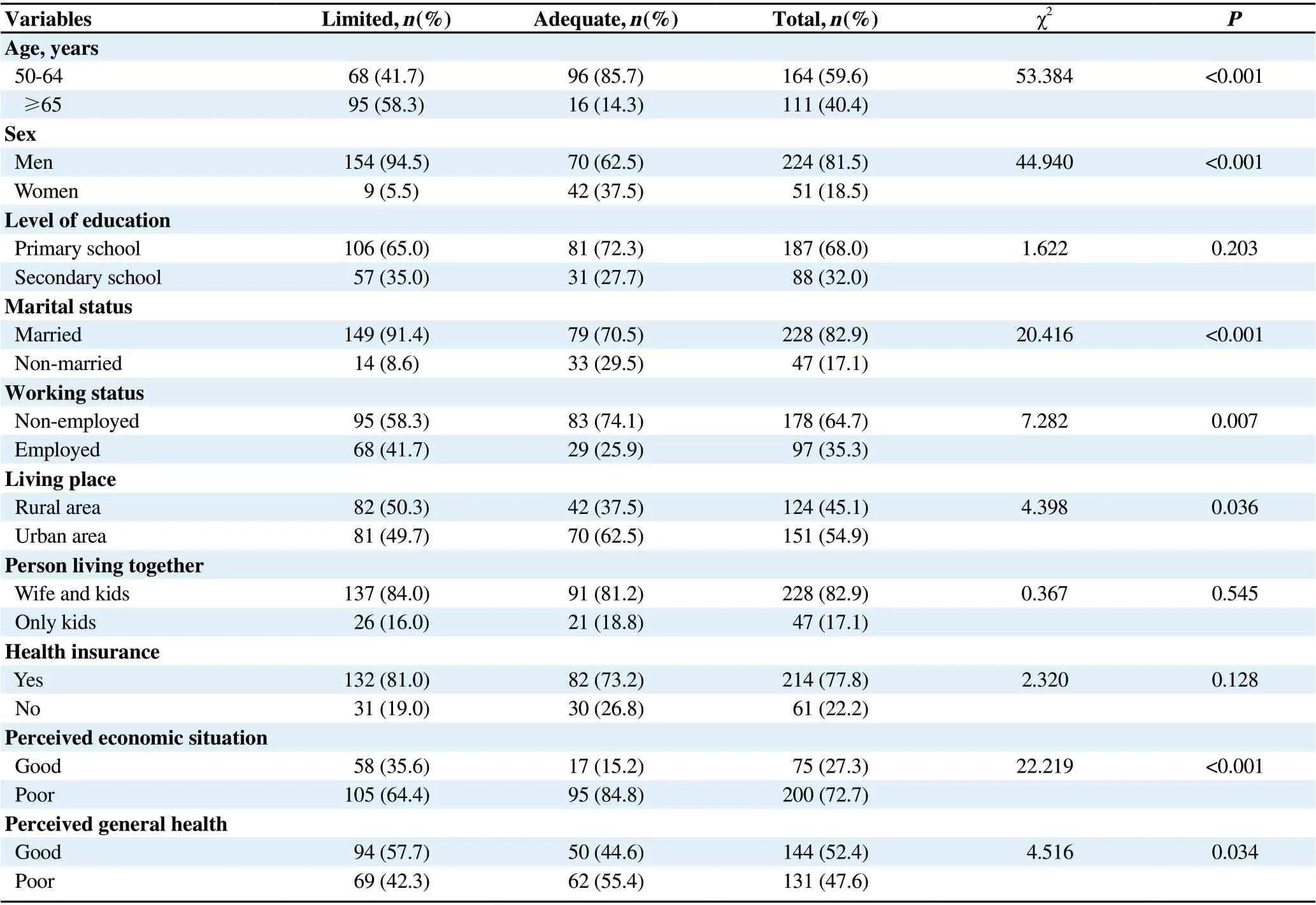
Table 1. Socio-demographic characteristics of the participants.
Among respondents who were married, non-employed, and living in rural areas adequate health literacy was significantly more often (P<0.05). Conversely, among patients with poor selfreported economic status and good self-reported health limited health literacy was more frequent (P<0.05). Education level,health insurance, and living with other people together were not associated with health literacy (P>0.05) (Table 1).
The distribution of patients' clinical characteristics based on health literacy levels is given in Table 2. Among the patients, 126 (45.8%)had a history of CAD (100 of previous angina and 26 of coronary artery bypass grafting). Major adverse cardiac events (MACEs)incidence rate for the entire population was 2.5% (7 patients).Patients with no comorbidities had higher health literacy level. Prevalence of adequate health literacy was present in 89.3% among patients without comorbidities. A significant difference was found in health literacy levels between patients with or without comorbidities (χ2=8.896, P=0.003).Nearly 44.4% of patients had a family history of CAD and the prevalence of limited health literacy was significantly more common (69.7%) among those (χ2=9.824, P<0.05).Approximately, two out of every five respondents had angiography history and limited health literacy was 68.0% among those without angiography history. Prevalence of health literacy differed significantly in terms of angiography history (χ2=4.985, P=0.025).No significant difference was found between the prevalence of health literacy in terms of kinds of CAD, history of bypass surgery, duration of hospitalization, and BMI (P>0.05) (Table 2).Health literacy was also analyzed in the context of the behavioral and psychosocial characteristics of the study population. A significantly higher prevalence of limited health literacy was found in patients with irregular health checks (χ2=12.712,P<0.001). Patients with limited health literacy were less likely to visit family medicine primarily (χ2=8.140, P<0.001). Moreover,the prevalence of limited health literacy was higher in current smokers and alcohol drinkers [(χ2=27.414, P<0.001), (χ2=17.918,P<0.001), respectively]. Nevertheless, patients with regular physical activity had a higher prevalence of limited health literacy(χ2=7.500, P<0.05). The prevalence of limited health literacy was more common among those skilled in medical material skills by themselves (χ2=8.034, P<0.001). Adequate health literacy level was (49.1%) in those with moderate/severe depressive symptoms and it was significantly higher (χ2=21.147, P<0.001) (Table 3). In the research group, the level of adequate health literacy was 66.1% for those who believe that being healthy depends on individual protective practices, and this rate was 33.9% for those who didn't believe. The level of health literacy showed a significant difference in terms of the participants' believes towards individual protective practices (χ2=45.191, P<0.001).
Logistic regression analysis of the variables affecting adequate health literacy is shown in Table 4. Table 4 lists the significant factors for the model with the estimated odds ratio (OR) and 95% confidence intervals (CI). Some variables that werenot associated with health literacy were not included in the regression analysis, including working stautus, living place,perceived general health, comorbidities, family history of CAD,angiography history, health checks, primary health system utilization, smoking status, alcohol consumption, and physical activity. The multilevel logistic model for health literacy showed that the probability of adequate health literacy was significantly higher among younger patients (OR: 2.81; 95% CI: 1.46-5.62),male gender (OR: 3.10; 95% CI: 1.46-6.58), married (OR:3.42; 95% CI: 1.39-8.44) and those with belief in individual protective practices (OR: 5.3; 95% CI: 1.93-14.96) (Table 4).

Table 2. Clinical characteristics of the participants.
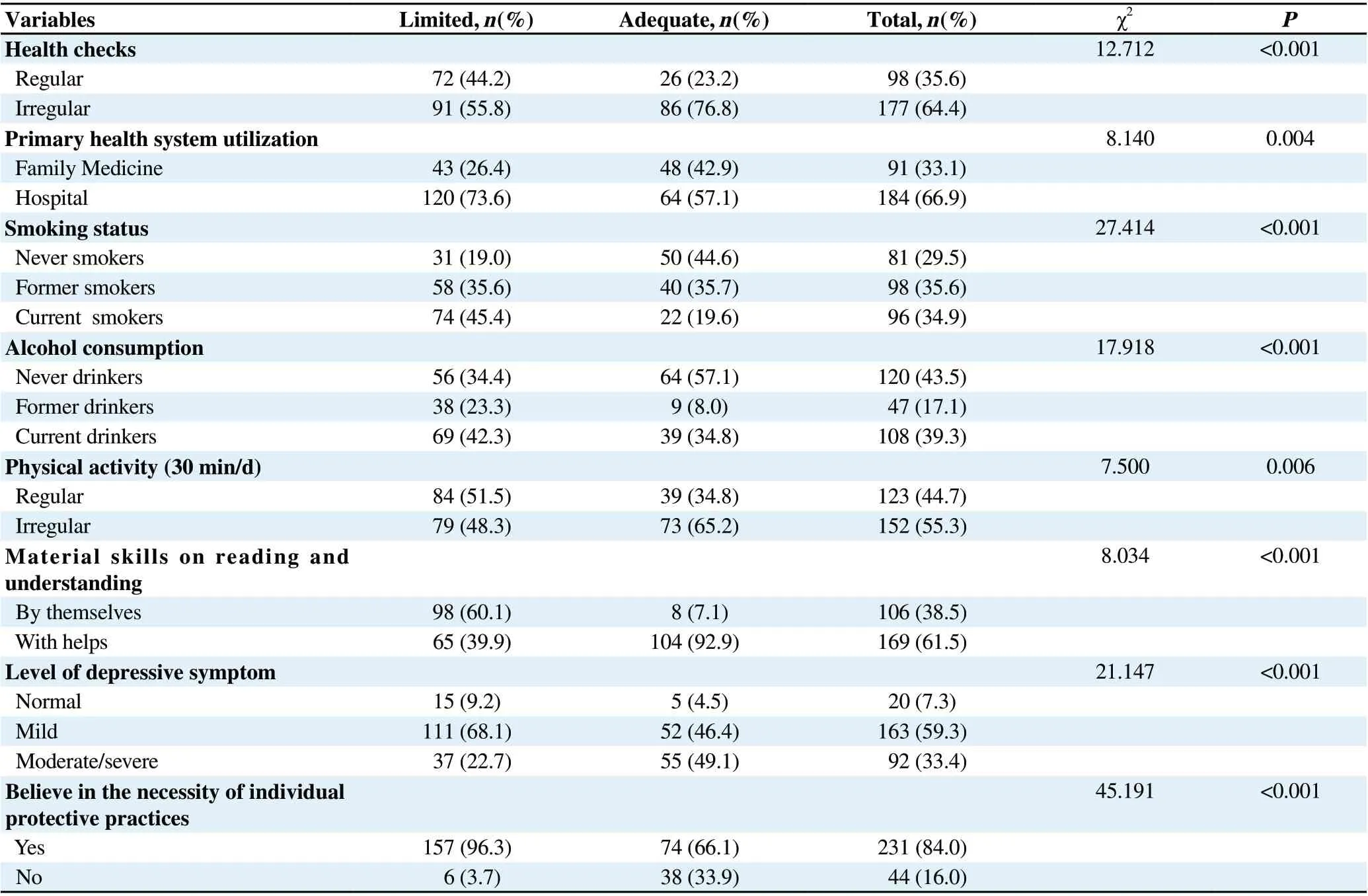
Table 3. Behavioral and psychosocial characteristics of the participants.
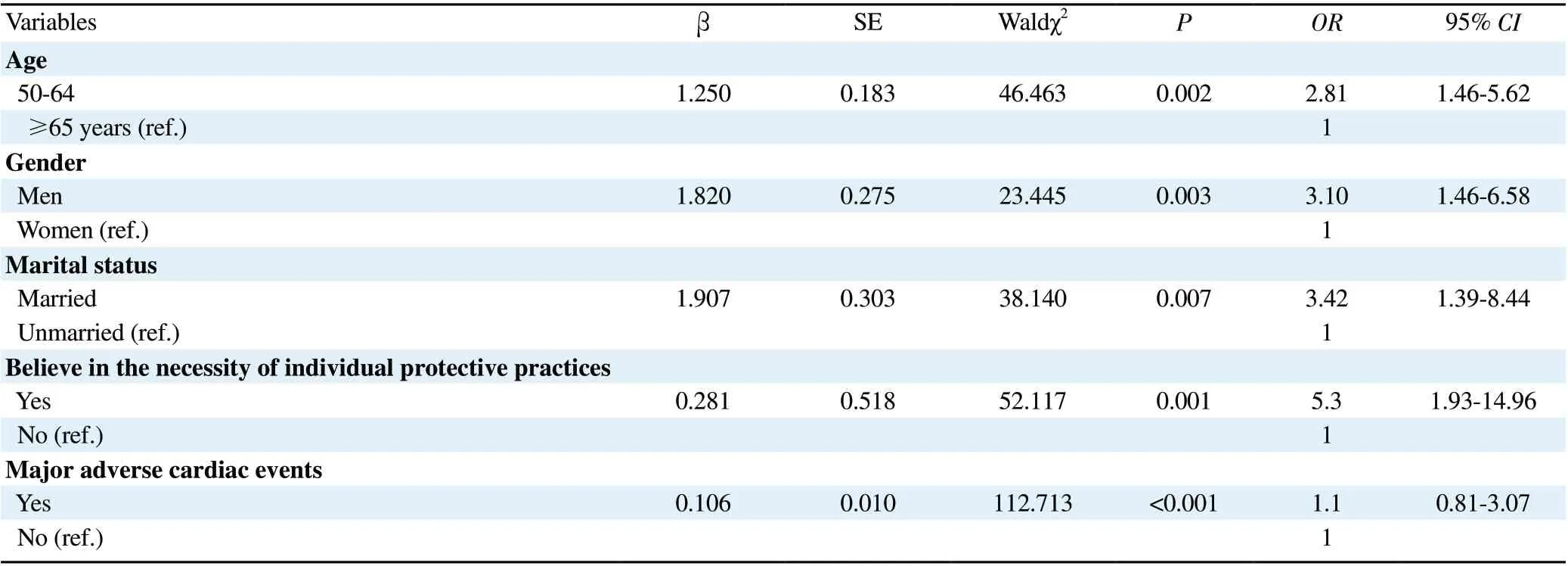
Table 4. Factors associated with adequate health literacy.
4. Discussion
The present study examined the health literacy and associated factors in CAD patients. Health literacy was found as inadequate/problematic in approximately two-thirds of the participants.Consistent with this study, international evidence also revealed that limitations in health literacy were common in such patients.Inadequate health literacy among CVD patients varied between 32%-39%[20,21] in the USA, and it was 20% in Sweden[22]. Patients with CVD had higher limited health literacy prevalence in Spain (nearly 80%)[23] and China (74.5%)[24]. Furthermore, limited health literacy prevalence was nearly 60% among patients applied to the cardiology outpatient clinic in our country[25]. It seems that CAD patients had a disadvantaged group in terms of limited health literacy.
In the present study, it was determined increased age was associated with limited health literacy (P<0.05). The level of adequate health literacy was 2.8 times higher in younger patients than older ones.Consistent with this study, in several prior pieces of evidence,inadequate health literacy was a more overemphasized challenge for elders[19,26]. The most plausible explanation for this situation is the decrease in cognitive functions with advancing age[27-29].
There is much evidence that health literacy levels also differ between genders[30-32]. While some studies showed that adequate health literacy was higher in women[29,30,32] in some studies it was higher in men[32,33]. In this study, adequate health literacy was found to be significantly lower in women than men (P<0.05).Adequate health literacy is 3.1 times higher in men than women. The differential impact of the level of health literacy on the genders may vary according to the social status attributed to the gender in society.In this study, adequate health literacy was found to be significantly lower in unmarried people compared to married ones (P<0.05).The adequate health literacy level of married people was 3.4 times higher than unmarried ones. However, some studies revealed that unmarried people had more adequate health literacy levels. In an Iranian study, the level of health literacy in married patients was found to be significantly lower than in singles[34]. Furthermore,it was observed that the health literacy level of married people was low in patients who applied to the family medicine outpatient clinic in our country[35]. Regulation of lifestyle behaviors and selfmanagement of treatment are important in the control of CAD.During this process, family members are expected to take an active role as well as the patients. The high adequate health literacy found in married individuals in this study may be due to the sharing of health messages between spouses in the management of CAD.
It was reported that the health literacy levels were affected by the employment status[36,37]. Similarly, in the present study, limited health literacy was significantly higher among those without a job(P<0.05). In parallel with our results, in our country, it had been shown that the employment status of patients in the cardiology service was affected by their health literacy level[26]. Employment status and working life may increase the interaction between individuals, and this may provide awareness and gains in terms of sharing health information. Individuals who do not have a job may experience limitations in these gains.
In a study conducted on inadequate health literacy was found to be higher in rural areas[38]. In the present study, it was observed that the health literacy level of the participants was more adequate among urban patients (P<0.05). Such a result may be explained by the fact that urban areas provide individuals with more opportunities in terms of access to health, education, transportation, and technology compared to rural areas.
In this study, another significant factor was the moderate perception of the economic situation for adequate health literacy. Study conducted in England reported that higher income is associated with higher levels of health literacy[29]. Considering the opposite, low socio-economic status is associated with limited health literacy[34].Income level interacts with welfare level and opens doors to individuals in many fields such as education and health.
The study conducted in Turkey showed that there was a positive association between health literacy and perceived health status[39].Unlike other studies, in this study, it was determined that health literacy was more adequate in those with a moderate health perception. Perception of health status in patients with CAD may be affected by many factors, and this situation may push individuals to seek more health information.
Negative reflections of limited health literacy are also seen in comorbidities[12,40] and in the present study, a similar result was observed that limited health literacy was common in comorbidities(P<0.05). The presence of multi-morbidities is an expected condition in CAD and multi-morbidities accompanying primary disease may hinder the ability to acquire and apply health-related information.
As a result of percutaneous coronary intervention due to previous stable or unstable cardiac events, it is a desired situation for patients with CAD to gain more awareness and had more health literacy.However, we found that patients without angiography history were more health literate than those with angiography history.
It was determined irregular health checks were linked to lower health literacy in the present study. Regular health checks are important in terms of the effective and appropriate use of health services and the development of health literacy as well as preventing the sequel of the disease.
In the present study, poor health literacy resulted in low primary health care utilization. Health literacy affects the use of health services, and that low health literate patients often use hospitals and emergency services instead of preventive health services[5].
Patients without smoking and alcohol intaking were more health literate in the present study (P<0.001). Similarly, smoking and alcohol consumption have been associated with inadequate health literacy in other studies[41,42]. Being aware of risk factors and improving lifestyle behaviors play an important role in the prevention and control of NCDs[3]. Adequate health literacy may be a protective barrier against risk factors for CAD.
It was stated that health literacy was positively associated with exercise[42]. In the present study, adequate health literacy was found to be higher in those without exercise regularly. This is an indication that patients are not able to turn into their knowledge to behavior adequately.
Another determinant of health literacy was believing the necessity of individual protective practice in this study (P<0.001). Avoiding and minimizing risks prevents complications and sequel, disease perception, cultural characteristics, social support mechanisms can shape beliefs about individual preventive practices and health literacy.
Health literacy is generally affected by psychosocial factors in addition to health, demographic and cultural factors[6]. Unexpectedly,adequate health literacy was more common among moderate/severe depressive symptom levels in the present study. Contrary to this study, depressive symptoms were associated with low health literacy in evidence from Spain[40]. The interesting result of this study can be explained as follows: the extreme psychological stress caused by illness can put pressure on patients and motivate them to be more health literate.
In this study, the material skills of patients didn't match with their health literacy levels. Health literacy has been found to be more inadequate in those who declared that they read and filled out health-related brochures/forms themselves (P<0.001). This result suggests that patients didn't understand and fill out health-related materials consciously. Thus, it has been determined that one-third of patients in Northern California were not sure even though they have completed medical forms[43].
This study has some limitations: (1) This study included only inpatients in the cardiology service and coronary intensive care unit of a state hospital; (2) There is no global scale to measure the level of health literacy.
In summary, limitations were common in the health literacy level of CAD patients. Depressive symptoms and negative behavioral factors were more common in limited health literacy. Older people,Females, non-married, who do not believe in the necessity of individual protective practices, and patients with MACEs were risky groups. To strengthen cardiovascular health among these patients,health literacy-based interventions should be adopted in coronary artery clinics especially for risky groups as a part of the cardiac rehabilitation programmes.
Conflict of interest statement
The authors report no conflict of interest.
Authors'contributionsA.A.: Data collection, writing, literature search; G.Y.: Study design, reviewing, language editing.
 Journal of Acute Disease2022年1期
Journal of Acute Disease2022年1期
- Journal of Acute Disease的其它文章
- Resuscitative cardiac arrest during a Caesarean section-When every second counts: A case report
- Influential factors of healthcare provider resilience in disasters: A thematic analysis
- Acute and sub-acute toxicities of hydroalcoholic extract of Allium affine aerial parts in rats
- Arrhythmia and its risk factors post myocardial infarction: A prospective study
- Incidence of adverse reactions to COVID-19 vaccination: A metaanalysis of randomized controlled trials