
Short-term effects of air pollutants on hospital admissions for acute bronchitis in children: a multi-city time-series study in Southwest China
2022-06-27 11:10:32YiHeWanyanhanJiangJiaQiangLiaoLinJingJiaLiLianYang
World Journal of Pediatrics 2022年6期
Yi He .Wanyanhan Jiang .Jia-Qiang Liao .Lin Jing .Jia Li .Lian Yang
Abstract Background Few studies have investigated the effects of air pollutants on children with acute bronchitis. This study aimed to explore the acute effects of four air pollutants [fine particulate matter (PM 2.5), inhalable particulate matter (PM 10), sulfur dioxide (SO 2), and nitrogen dioxide (NO 2)] on the daily number of children admitted to the hospital for acute bronchitis in Sichuan Province, China.Methods The 49,975 records of hospitalized children with acute bronchitis from medical institutions in nine cities/prefectures, Sichuan Province, China, as well as the simultaneous meteorological data and air pollution data from 183 monitoring sites, were collected from 1 January 2017 to 31 December 2018. A generalized additive model was adopted to analyze the exposure–response and lag effects of hospitalizations of children with acute bronchitis to air pollutants. Stratified analyses were conducted based on sex, age, and season.Results The single-pollutant model showed that a 10 μg/m 3 increase at lag07 of PM 2.5, PM 10, SO 2, and NO 2corresponded to an increase of 1.23% [95% confidence interval (CI) 0.21–2.26%], 1.33% (95% CI 0.62–2.05%), 23.52% (95% CI 11.52–36.81%), and 12.47% (95% CI 8.46–16.64%) in daily hospitalizations for children with acute bronchitis, respectively. Children aged 0–2 were more prone to PM 2.5 (P< 0.05). Interestingly, the effects were stronger in the warm season than in transition seasons and the cool season for PM 2.5and PM 10(P< 0.05).Conclusion The higher daily average concentrations of four pollutants in Sichuan Province can result in an increased number of children hospitalized for acute bronchitis.
Keywords Acute bronchitis · Air pollutants · Children · Time-series study
Introduction
Rapid urbanization and industrialization, as well as the sharp increase in energy consumption in China, have brought about diverse air pollution problems. The adverse health effects of short-term exposure to ambient air pollutants have been widely studied [ 1]. Global research has found positive correlations between short-term exposure to fine particulate matter (PM 2.5 ) and inhalable particulate matter (PM 10 ), daily all-cause mortality, cardiovascular disease mortality, and respiratory disease mortality [ 2]. In 2019, environmental particulate pollution was among the three types of disease risk factors accounting for more than 1% of disabilityadjusted life years [ 3].
Air pollution is a neglected public health emergency for children worldwide [ 4]. Children are particularly susceptible to ambient air pollution due to their physiological and behavioral characteristics [ 5]. The lungs of children are not fully developed, they breathe more air per kilogram of body weight than adults, and their respiratory systems are more prone to damage, which results in a decline in their lung function [ 6]. According to World Health Organization estimates and the Global Burden of Diseases, Injuries, and Risk Factors Study, approximately 1 million children under 5 years age died of lower respiratory tract infections in 2015, partly due to exposure to air pollution, insufficient nutrition, and health care [ 7]. By 2016, 600,000 children died of acute lower respiratory infections caused by air pollution [ 4].
Studies in China have also indicated that air pollutants have adverse effects on the lower respiratory tract of children. Leung et al. in Hong Kong, China and Liang et al. in Guangzhou found that increased air pollutant concentrations were associated with increased hospital admissions for acute bronchiolitis in children [ 8, 9]. Several studies have also found that increased air pollutant concentrations are associated with increased hospital admissions for pneumonia and asthma [ 10].PM 2.5 and PM 10 are respirable particulate matter, while sulfur dioxide (SO2) and nitrogen dioxide (NO2) are gaseous substances. Different types of air pollutants have different mechanisms of damage to the respiratory system; respirable particulate matter penetrates the alveolar epithelium and triggers inflammation in the lungs, while gaseous pollutants mainly cause bronchoconstriction and breathing difficulties, such as asthma [ 11, 12]. Although an increasing number of studies have shown that air pollutant exposure is related to childhood lower respiratory tract diseases, research on the associations between air pollutant exposure and hospitalizations for acute bronchitis in childhood are still limited. Acute bronchitis, a lower respiratory tract infection characterized by coughing with or without sputum production lasting several days to several weeks, is a common disease treated in pediatrics [ 13]. From 2015 to 2019, the global incidence of acute lower respiratory infections in children aged 0–14 showed an increasing trend [ 14]. Acute lower respiratory infections, including acute bronchitis, have been the main causes of mortality in children under 5 years of age (except newborns) [ 15].
Sichuan Province, located in Southwest China with approximately 90 million residents, is roughly divided into the Sichuan Basin and the Western Sichuan Plateau in terms of topography. The degradation of pollutants is linked to geographical factors, with the basin and the surrounding plateau alpine terrain atmospheric pollutant dispersion degree causing relatively slow dispersion of atmospheric pollutants, making the region became one of China’s most polluted regions, and therefore there are large differences in concentrations of different pollutants in different cities. In addition, meteorological conditions such as temperature and humidity also vary from city to city [ 16]. However, most prior studies analyzing air pollution and health outcomes focused on the provincial capital city of Chengdu, Sichuan [ 17]. Limited studies have evaluated the overall exposure to air pollutants in multiple regions of Sichuan Province. To better evaluate the impact of air pollutant exposure in Sichuan Province on the daily hospitalizations of children with acute bronchitis, we conducted a time-series study to analyze the associations between PM 2.5 , PM 10 , SO 2 , and NO 2 and the daily number of children hospitalized for acute bronchitis.
Methods
Acute bronchitis admission data
There are 21 cities and prefectures in Sichuan Province, including 18 cities and prefectures in the Sichuan Basin and three cities and prefectures in the Western Sichuan Plateau. This research collected relevant data of hospitalized children with acute bronchitis (ICD-10 J20) including age, sex, home address, date of admission, disease diagnosis, and disease code in municipal hospitals from January 1, 2017 to December 31, 2018, in nine cities in Sichuan Province, namely, Chengdu, Guang'an, Luzhou, Liangshan Yi Autonomous Prefecture, Mianyang, Meishan, Nanchong, Yibin, and Zigong. A total of 49,975 cases were collected, excluding those with home addresses outside Sichuan Province, to analyze the association between air pollutants and hospitalization of children due to acute bronchitis. The subjects included in the study were children in Sichuan, aged 0–14 years.
Meteorological data and air pollution data
We collected daily meteorological data from the Sichuan Meteorological Bureau ( http:// www. scdata. net. cn/ ) from January 1, 2017, to December 31, 2018, which included daily average temperature and relative humidity.
Particulate matter with aerodynamic diameter ≤ 10 μm (PM10), particulate matter with aerodynamic diameter ≤ 2.5 μm (PM2.5), SO2, and NO2were selected as representatives of outdoor air pollution. These four pollutants are closely associated with respiratory diseases [ 18]. The average daily concentrations of PM 2.5 , PM 10 , SO 2 , and NO 2 were collected from the Sichuan Environmental Monitoring Station (183 air monitoring stations) from January 1, 2017 to December 31, 2018. These stations are mandated to be located away from major roads, industrial sources, buildings, and residential sources of emissions from the burning of coal, oil, or waste. This ensures that the monitoring results reflect the urban air pollution level in the city rather than local sources of traffic or industrial combustion.
Statistical analysis
Spearman’s correlation was used to analyze the correlations between air pollutants and meteorological indicators. The closer the absolute value of the correlation coefficient r is to 1, the stronger is the correlation estimated.
The time-series analysis method in the generalized additive model (GAM) has been widely used to assess the associations between air pollutants and hospitalization for respiratory diseases [ 19]. Since the daily number of children hospitalized for acute bronchitis typically followed an over-dispersed Poisson distribution, this study adopted a quasi-Poisson distribution in the GAM model. The health effects of air pollution may have a negative effect. Therefore, this study analyzed the associations between the four air pollutants (PM 2.5 , PM 10 , SO 2 , and NO 2 ) and the daily average number of children hospitalized for acute bronchitis with single-day lags from the current day (lag0) and each 1–7 days before the acute bronchitis event (lag1, lag2, lag3, lag4, lag5, lag6, and lag7) and moving average exposure of multiple days (lag01, lag02, lag03, lag04, lag05, lag06, and lag07). In addition, meteorological factors may also affect the hospitalizations of children with acute bronchitis. Hence, the average daily temperature and relative humidity were introduced into the model as control variables. The model is as follows (Eq.1):
where E(Yi) is the expected number of children hospitalized for acute bronchitis on day i; α stands for the model intercept; Zi represents the air pollutant concentration on day i (μg/m 3 ); β represents the exposure–response coefficient, which is the increase in the number of daily hospitalizations caused by the per unit increase in pollutant concentration; s is a non-smooth parameter item; and df is the degree of freedom. The time stands for a date variable with a degree of freedom of 7/year; dow is an indicator variable of “day of the week”; temperature and humidity stand for the average daily temperature and relative humidity, whose degrees of freedom are both 3.
After the exposure–response relationship coefficient, β (Eq.1) was estimated using the generalized additive model, and the relative risk increase (RRI) and the 95% confidence interval (CI) of children hospitalized for acute bronchitis were calculated for every 10 μg/m 3 increase in air pollutants (Eq.2) [ 20]:
A spline function of GAM was applied to plot the exposure and response correlation curves between air pollution and hospital admissions for acute bronchitis. Moreover, two-pollutant models were set to evaluate the robustness of our results after adjusting for other pollutants. In the subgroup analyses, stratified analyses were conducted based on sex (boys and girls), age (0–2 years old, 3–6 years old, 7–14 years old), and season (transition season: 4, 5, 9, and 10 of each year from 2017 to 2018; hot season: 6 to 7 each year; cold season: 11 to 3). We tested significant differences from stratified analyses of potential effect modifiers by calculating the 95% CI, based on the following formula (Eq.3):
where ^Q1and ^Q2are the adjusted estimates for two categories (e.g., boys and girls), S^E1and S^E2are their respective SE s [ 21].
All statistical analyses in this study were conducted using R3.4.3, and the quasi-Poisson regression model was constructed using the “mgcv” package. The statistical tests were two-sided, and associations with P < 0.05 were considered statistically significant.
Sensitivity analysis
Two types of sensitivity analyses were performed to verify the stability of the model. First, the stability of the time trend was tested, and the model was fitted by changing the degree of freedom of the time-series ( df = 5, 6 per year). Second, to confirm the robustness of the association results, a sensitivity analysis was performed by evaluating the cases within circular areas of 50 km surrounding air monitoring stations, which could deduce the potential effect of the distance between the air pollution monitoring site and the address of the patient [ 22].
Results
Data description
Table 1 provides a description of air pollution levels, meteorological variables, and the daily number of hospitalizations for acute bronchitis. During the study period, the daily average concentrations of PM 2.5 , PM 10 , SO 2 , and NO 2 were 50.17 μg/m 3 , 76.12 μg/m 3 , 12.61 μg/m 3 , and 29.66 μg/m 3 , respectively. It is worth noting that the daily average concentrations of PM2.5, PM10, SO2, and NO2did not exceed the secondary standards in the “Ambient Air Quality Standards” issued by the Chinese government (GB3095-2012) (24 hours average standards for PM2.5is 75 μg/m 3 , PM10is 150 μg/m 3 , SO2is 150 μg/m 3 , and NO2is 80 μg/m 3 ). The average daily temperature and humidity were 16.46 ℃ and 76.64%, respectively. During the study period, 49,975 children hospitalized for acute bronchitis were included in the study. The average daily number of hospitalized cases was 68, with more boys hospitalized daily than girls. The 3- to 6-year-old age group had the largest number of hospitalizations per day: 31. More children were hospitalized in cold seasons than in the other two seasons.
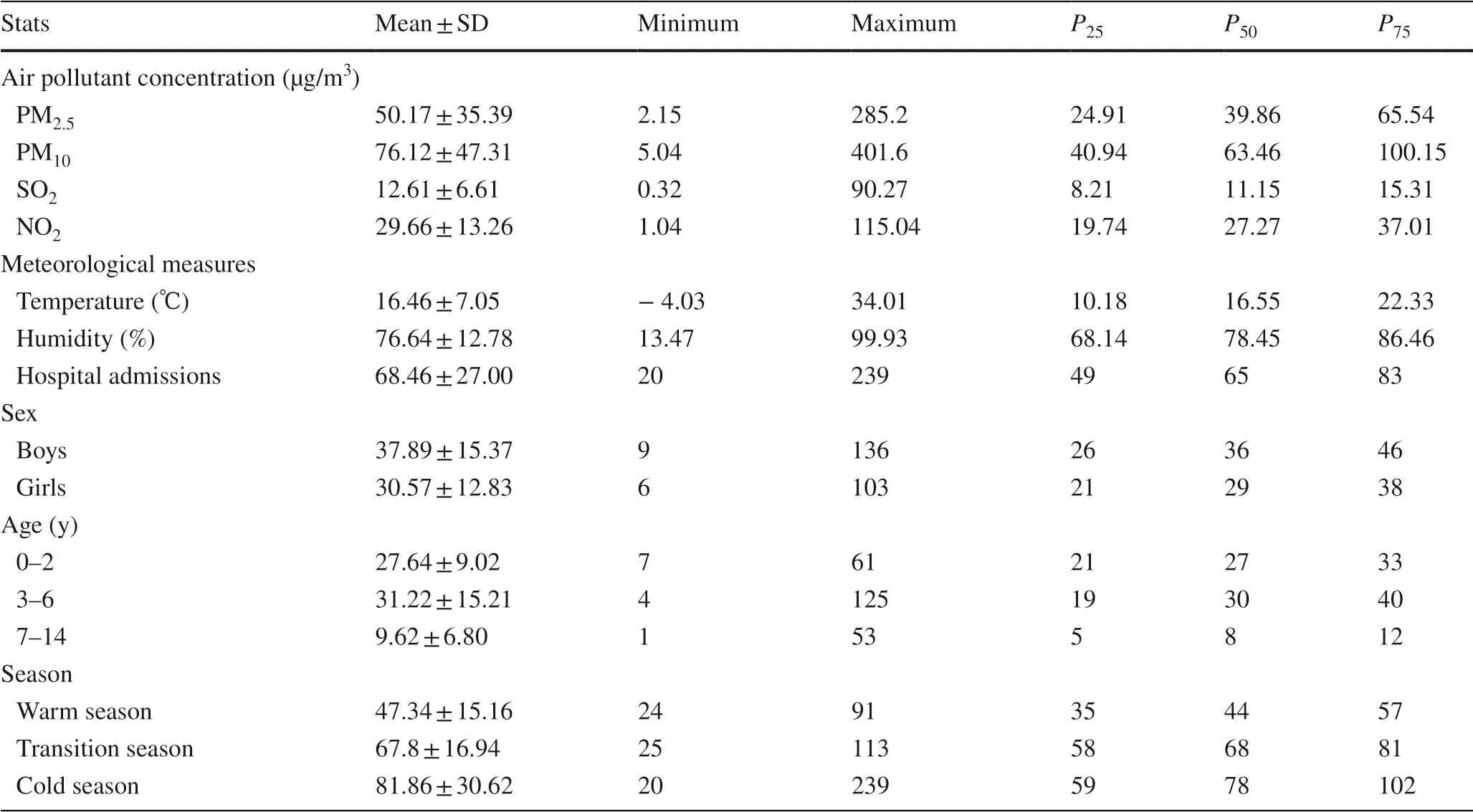
Table 1 Description of daily air pollutants, meteorological parameters, and hospitalized characteristics of children with acute bronchitis in Sichuan Province, China, during 2017–2018
Generally, we observed significant positive correlations between PM 2.5 , PM 10 , SO 2 , and NO 2 , with the correlation coefficient r being 0.2951–0.9447.PM10also showed strong correlations with SO2and NO2, with correlation coefficients of 0.2847 and 0.6429, respectively. The correlation coeffi-cient between SO2and NO2was 0.2117. There was a negative correlation between air pollutants and meteorological variables (P< 0.05) (Supplementary Table 1).
Health effects of pollutants in the overall and subgroup population
Figure 1 shows the smoothing E–R curves between air pollutants and daily total hospital admissions for acute bronchitis in Sichuan, China. In general, we observed significantly positive associations between respiratory diseases outpatient visits and the concentration of SO2and NO2. However, there is a non-linear association between particulate matter and daily total hospital admissions for acute bronchitis.
The associations between air pollutants and the number of children hospitalized for acute bronchitis were measured using the single-pollutant model, evaluating singleday lags (lag0–lag7) and moving average exposure of multiple days (lag01–lag07) of air pollutant concentrations for every 10 μg/m3increase, as well as changes in the daily number of children hospitalized for acute bronchitis. The estimated single-day effects of PM2.5, PM10, SO2, and NO 2 all reached the maximum at lag7, and the RRIs were 0.87% (95% CI 0.21–1.54%), 0.93% (95% CI 0.46–1.41%), 15.59% (95% CI 9.06–22.52%), and 5.91% (95% CI 3.62–8.25%). The estimated multi-day effects reached the maximum at lag07, and the RRI were 1.23% (95% CI 0.21–2.26%), 1.33% (95% CI 0.62–2.05%), 23.52% (95% CI 11.52–36.81%), and 12.47% (95% CI 8.46–16.64%) (Fig.2).
Figure 3 shows the impacts of PM2.5, PM10, SO2, and NO2on the health of children of different sexes and age and in different seasons when the air pollutant concentrations increased by 10 μg/m 3 . The impact of different pollutants on children of different sexes was not statistically significant ( P > 0.05); PM2.5caused more hospitalizations for acute bronchitis in children aged 0–2 than in children aged 3–6 and 7–14, and the difference was significant ( P = 0.032). Due to PM2.5and PM10exposure, more children were likely to be hospitalized for acute bronchitis in summer than in transition and cold seasons, and the difference was statistically significant (P< 0.05) (Supplementary Tables 2 and 3).
Based on the results of the lag effect analysis of the single-pollutant model, the results of the two-pollutant models at lag02 are provided in Table 2. After the introduction of the second pollutant, the impact of a single pollutant would be affected to an extent. Occasionally, the effects were enhanced. For example, the effects of NO2were strengthened after the introduction of PM2.5. At other times, the effects weakened. The effects of some pollutants weakened after the introduction of SO2and NO2. The results of the two-pollutant model analyses suggested that researchers should pay attention to the interactions among pollutants when studying the effects of air pollutants on the number of children hospitalized for acute bronchitis.
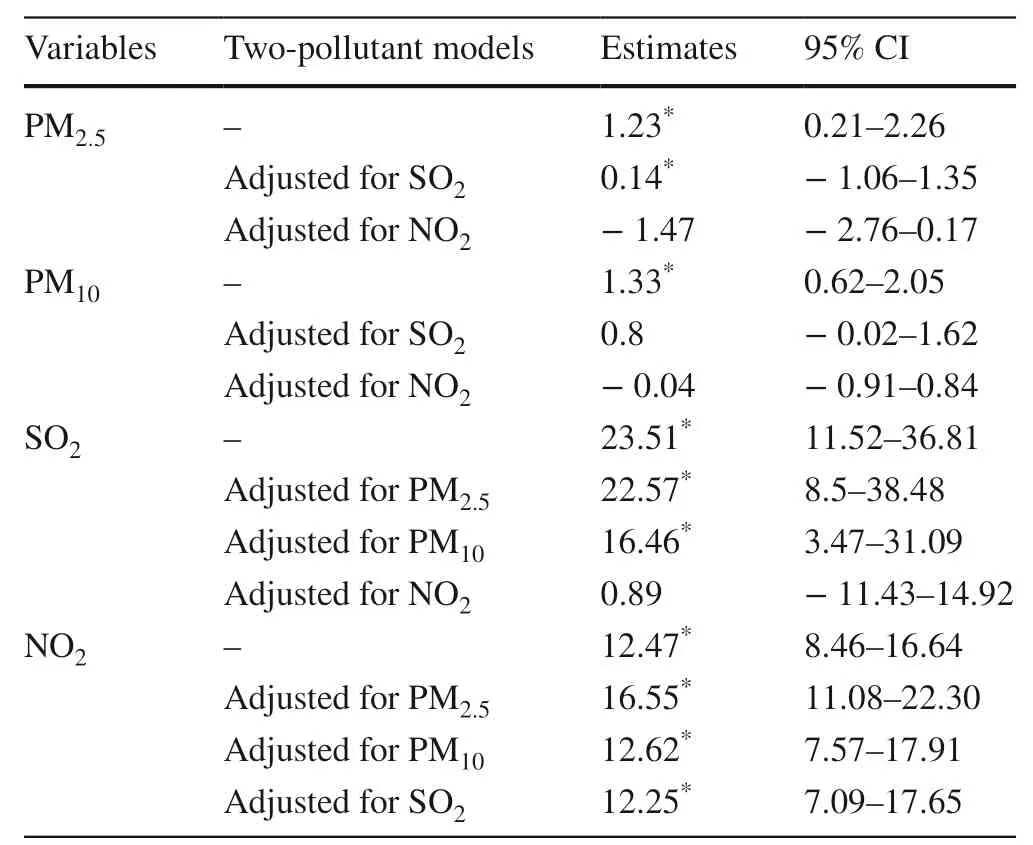
Table 2 Percentage change (95% confidence interval) of children hospital admissions per 10 μg/m 3 increase in concentrations of pollutants in the single and two-pollutant models
Sensitivity analysis
In the sensitivity analysis, the acute impact of air pollutants on the hospitalizations of children with acute bronchitis did not change substantially after replacing the annual degree of freedom of the time-series ( df) with 5 and 6 (Supplementary Table 4). Second, the home addresses of 25 patients were more than 50 km away from their nearest monitoring site. After removing these data, the estimated effects of PM2.5and PM10were still at the maximum level at lag07, which was not significantly different from the results of the original model (Supplementary Table 5).
Discussion
This study focused on the associations between exposure to air pollutants and the risk of hospitalization for children with acute bronchitis in Sichuan Province, China from 2017 to 2018. After controlling for temperature and humidity, the results showed that short-term exposure to air pollutants increased the risk of hospitalization for children with acute bronchitis. Acute bronchitis in children increases within a few days of exposure. The age and sex of patients and the season are associated with various risks. The findings enrich empirical evidence of associations between air pollutants and respiratory diseases in heavily polluted areas in developing countries.
In the single-pollutant model, when the concentrations of pollutants increased by 10 μg/m 3 , there were positive associations between PM2.5, PM10, SO2, and NO2and the hospitalizations of children with acute bronchitis, with the maximum RRI at lag07. The number of children hospitalized for acute bronchitis increased by 1.23% (95% CI 0.21–2.26%), 1.33% (95% CI 0.62–2.05%), 23.52% (95% CI 11.52–36.81%), and 12.47% (95% CI 8.46–16.64%), respectively, demonstrating a lag effect in the impact of air pollutants on acute bronchitis, which was consistent with most research results. This finding provides evidence that air pollutants are risk factors for lower respiratory diseases in children. According to Zhu et al.’s time-series study in Nanjing, China, the impact of PM10, SO2, and NO2on the lower respiratory tract of children increased significantly at lag05 [ 23]. A time-series study by Li et al. in five Chinese cities showed that both PM2.5and PM10in various cities had the greatest impact on hospital visits for respiratory disease at lag07 [ 24]. A systematic review and meta-analysis of childhood asthma found that a longer lag time resulted in a higher association between PM 10 and cough [ 18]. In addition, Halone et al. also reported that the association between air pollution and hospital visits for asthma among children lagged for 3–5 days [ 25].
The occurrence or aggravation of the adverse health consequences of the respiratory system is related to the dose of inhaled air pollutants and their deposition sites in the human body [ 26]. The adverse effects of PM2.5and PM10on children’s respiratory systems include childhood asthma, bronchitis, and other diseases [ 27]. According to the classification based on aerodynamic diameter (AD), the diameter of PM2.5is less than that of PM 10 . Studies have shown that coarse particles with an AD of less than 10 μm are mainly deposited in the airways. Interestingly, due to its small diameter, PM2.5, which is easily deposited in the bronchioles and alveoli and passes through the alveolar-capillary barrier, causing greater harm to the human body [ 12]. The components of PM2.5are complex and diverse, resulting in different effects. Toxicological studies have found the toxic effects of PM2.5, including oxidative damage, mutagenicity and carcinogenicity, immunotoxicity and inflammation, cell cycle, and changes in vitality [ 28]. The damage mechanism of PM2.5, in the respiratory system, is mainly cell-particle interaction, in which the particulate matter causes human lung epithelial A459 cells to produce excessive reactive oxygen and the loss of antioxidant enzyme activity, inducing cellular oxidative stress, which leads to the massive secretion of inflammatory cytokines and enhances the expression of inflammatory factors. Consequently, inflammatory damage to the body occurs, which results in lung and airway malfunction, which leads to systemic inflammation and aggravates acute bronchitis in patients [ 29– 31]. During the combustion and refining of sulfur-containing fuels such as coal and petroleum, SO2dissolves into water vapor to form acid and interacts with other gases and particles in the air to form sulfates and inhalable particulate matter [ 32]. Research from Harvard University also showed that SO2can be converted into sulfuric acid and then enter the small airways through inhalable particulate matter, impairing children’s lung function [ 33].SO 2 can also reduce the oscillation frequency of nasal cilia cells and thus weaken the body’s ability to remove foreign bodies and resist external harmful substances, making the body susceptible to tracheitis and bronchitis [ 34].NO2is common in both indoor and outdoor environments. The main sources of outdoor pollutants are automobile exhaust and gasoline combustion [ 35]. The free radicals of NO2can cause lipid peroxidation of the alveolar cell membrane, thereby inducing airway inflammation [ 36].
In the sex analysis, no significant difference between boys and girls was observed, which is consistent with the results of previous studies. In the age analysis, we found that children aged 0–2 were more susceptible to air pollution. For each 10 μg/m 3 increase in PM2.5, the number of children hospitalized for acute bronchitis increased by 1.08% (95% CI 0.23–2.00%), which was similar to the findings of Ningbo [ 37]. This may be explained by the fact that children in this age group have lungs not fully developed, linked with high respiration frequency, and they often are mouth-breathers [ 38]. In seasonal analysis, we found that air pollutants had a greater impact on the number of hospitalizations for acute bronchitis in the hot season. This was consistent with the research results of Hua et al. in Shanghai, in which they observed a stronger impact of PM 2.5 and PM 10 in the hot season [ 39]. Studies have shown a higher correlation between individual air pollutant exposure and ambient air pollutant concentrations in summer than in winter [ 40]. Therefore, while ambient air pollutant concentrations were higher in winter, individual exposure to air pollutants was lower. In summer, the air is usually cooler in the evenings, and children often stay outdoors with their families. In addition, air pollutant concentrations generally reach the maximum level in the evening. Consequently, the likelihood of individual exposure to air pollutants is enhanced in summer, thereby increasing the risk of hospitalization for acute bronchitis.
After the introduction of SO 2 in the two-pollutant models, the effect was enhanced in comparison with the results in models with only PM10or NO2. However, the enhancement was small but statistically significant. This suggests that PM10and NO2have significant impact on the hospitalizations of children with acute bronchitis and that the singlepollutant model is relatively stable. After the introduction of PM10, SO2, and NO2, the effects of each pollutant increased or decreased to a certain extent, and some of the differences were not statistically significant. The above results indicate that the effects of pollutants are not simply superimposed. This may be due to the collinearity effect between different pollutants, leading to a synergistic effect on the effect of acute bronchitis, which in turn affects the authenticity of the model.
This study makes several contributions. First, we explored the associations between air pollutants and hospitalizations in children with acute bronchitis. Children belong to a group susceptible to being affected by air pollutants and are prone to hospitalization for acute bronchitis. Most prior studies have linked air pollutants to hospitalizations for various respiratory diseases. This study provides empirical evidence for the association between air pollutants and acute bronchitis in children. Moreover, this study selected nine cities and prefectures in Sichuan Province, eight of which were from the Sichuan Basin and one was from the Western Sichuan Plateau, representing the overall characteristics of Sichuan Province to a certain extent. However, this study has some limitations. First, as ecological research, the research results cannot represent the real situation due to the existence of confounding factors. In addition, since only 2 years of data were used to analyze the correlation between air pollutants and the number of children hospitalized for acute bronchitis, there might be some instability in the generalized additive model.
In summary, time-series analysis was used to evaluate the short-term impact of ambient air pollutants on the number of children hospitalized for acute bronchitis from 2017 to 2018 in Sichuan Province. Involving the generalized additive model, we found that an increase in the average daily concentrations of PM2.5, PM10, SO2, and NO2could increase the hospitalizations of children with acute bronchitis and that there is a lag effect. In addition, the research results also show that particulate matter had a more significant impact on younger children and these patients were more susceptible to being affected by air pollutants in the hot season. To protect the health of children, the relevant departments of Sichuan Province should take effective measures to reduce the emissions of harmful substances into the air.
Supplementary Information The online version contains supplementary material available at https:// doi. org/ 10. 1007/ s12519- 022- 00537-1.
Author contributions YH initiated the idea for the study and was involved in writing of the original draft. WJ, YH, JLQ and JL developed the formal analysis and software. LJ was involved in data curation. LY was involved in reviewing and editing. LY was the PI for the fund and designed ideas of research. All the authors participated in revising manuscript according to the comments of reviewers and approved the final report.
Funding The authors received financial support from the National Natural Science Foundation of China (No. 72174032), and the research projects of “Xinglin Scholars” Nursery Talent in 2021 Research Plan of Chengdu University of Traditional Chinese Medicine through grants MPRC2021013.
Data availability The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethical approval All the procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki. This study was approved by the Ethics Committee of Hospital of Chengdu University of Traditional Chinese Medicine (approval no. 2020KL-001).
Conflict of interest No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article. The authors have no conflict of interest to declare.
 World Journal of Pediatrics2022年6期
World Journal of Pediatrics2022年6期
- World Journal of Pediatrics的其它文章
- Instructions for Authors
- Applications of mPCR testing reduced initial antibiotic use and duration of mechanical ventilation in virus-infected children with severe community-acquired pneumonia admitted to the PICU
- Serum homocysteine, lipid profile and BMI as atherosclerotic risk factors in children with numerical chromosomal aberrations
- Neonates are more vulnerable to symptomatic SARS-CoV-2 infection than children: a matched cohort study in Brazil
- Trichotillomania occurs during the COVID-19 pandemic in an adolescent
- Impact of rotavirus vaccine implementation on Israeli children: a comparison between pre- and post-vaccination era