
Conventional treatment options and herbal remedies for male infertility: An overview
2022-09-06 02:35:06AnkitaWalPranayWalAshutoshPandeyHimangiVigRohiniKarunakaranBiswajitDash
Ankita Wal, Pranay Wal, Ashutosh Pandey, Himangi Vig, Rohini Karunakaran, Biswajit Dash
1Pranveer Singh Institute of Technology Pharmacy Kanpur, 209305 Uttar Pradesh, India
2Unit of Biochemistry, Faculty of Medicine, Centre of Excellence for Biomaterial Science, AIMST University, 08100 Semeling, Kedah, Malaysia
3Department of Computational Biology, Institute of Bioinformatics, Saveetha School of Engineering, SIMATS, Chennai, Tamil Nadu, 602105, India
4NEPEDS College of Pharmaceutical Sciences, Guhawati Assam, 781028, India
ABSTRACT Male infertility is responsible for an estimated 50% of all cases of infertility. Treatments for male infertility include surgery, invitro fertilization, hormone therapy, and herbal remedies. Assisted reproductive technologies and methods have made it possible to identify and treat previously untreatable causes of male infertility.Currently available treatments for male infertility are prohibitively expensive, difficult to obtain, necessitate a lengthy course of treatment, and have a host of side effects. Herbal therapy offers male infertility treatment that is less expensive and has fewer side effects than other treatments. The current review focuses on the various treatment options for male infertility.
KEYWORDS: Male infertility; Ayurveda; Antifertility herbs;Hormonal therapy; Epididymovasostomy; In-vitro fertilization;Human chorionic gonadotropin; Intracytoplasmic sperm injection
1. Introduction
Infertility is defined by the World Health Organization (WHO)as the inability to bear children following at least 12 months of constant, unprotected sexual intercourse[1]. Infertility is a significant health issue that affects 8%-12% of couples around the world,with masculine factors being a significant or fundamental aspect in around 50% of cases. Infertility causes a lot of mental and social stress, and it costs both the patient and the health care system a lot of money[2]. Male subfertility can be caused by hereditary, acquired or pathological conditions that interfere with sperm production[3,4].Many genes and environmental variables have been linked to male infertility, yet approximately 30% of instances are still considered idiopathic. One percent of males are azoospermic[5], which means they do not have any sperm in their ejaculate. Azoospermia can be caused by a blockage in the genital tract, giving obstructed azoospermia, or by basic testicular insufficiency, leading to spermatogenesis failure, resulting in non-obstructive azoospermia.Low sperm count and/or poor sperm morphology are common symptoms of these issues. Hormonal fluctuations, oligospermia,decreased sperm motility, prostatitis, varicocele, and other conditions are examples. Intracytoplasmic sperm injection (ICSI)is the most common treatment for infertile men nowadays. Because sperm is obtained via arousal, this method is painless for the male partner. But, the female partner must undergo several invasive tests to achieve ICSI, involving blood testing, hormone treatments,operative ova retrieval, and embryo transfer. Some of these techniques are unpleasant and have short-and long-term medical risks, such as ovarian hyperstimulation and subsequent pregnancy.Many infertile couples are unable to afford assisted reproductive technologies, including in-vitro fertilization (IVF), zygote intrafallopian transfer, and ICSI[6]. Different infertility treatments and assisted reproductive procedures are costly. Due to the limitations of assisted reproduction techniques, patients with male infertility frequently turn to alternative treatments, such as herbal treatment[7].Across most developing nations, infertile couples are treated with both natural treatments and modern therapies. Due to restricted access to orthodox treatments, conventional medicine is generally the initial therapeutic option for infertile couples in impoverished and underdeveloped nations. Experiments are being done with crude extracts, decoctions, and partially purified parts of medicinal herbs to treat problems with infertility, impotence, ejaculatory problems,and faulty spermatogenesis. They are all treated with these herbal therapies. The goal of this review article is to highlight the numerous male infertility treatment options available, such as hormone therapy, surgery, and ICSI, among others. It also discusses what orthodox medicine cannot accomplish and what herbal remedies can accomplish more effectively.
2. Male infertility prevalence
The estimated incidence of male infertility, as well as the exact necessity of male infertility medical services, is unknown. No registration system gathers data about male sexual wellness in a methodical and particular manner. Infertility affects 60-80 million couples globally, according to the WHO[8]. It varies by area and is expected to impact 8%-12% of couples worldwide[9]. In India, 12-18 million couples are diagnosed with infertility each year. Male infertility accounts for roughly 40%-50% of all infertility cases,with just as many as 2% of all males having insufficient sperm parameters. Low sperm volume, sperm motility, or morphological abnormalities are all possibilities. According to the WHO, the prevalence rate of main infertility is between 3.9% and 16.8%[10]. In India, the number of people who are unable to have children ranges from 3.7% in Uttar Pradesh[11], Himachal Pradesh, and Maharashtra to 5.0% in Andhra Pradesh and 15.0% in Kashmir[12,13].
Women were responsible for 40% of fertility problems, men for 40%, and both sexes were responsible for 20%[14]. As shown in a WHO multicentric dataset, male variables were responsible for 20%of cases and female variables for 38%[15]. For around 23% of Indian spouses taking medication, the male element is to blame[16]. A recent analysis of infertility in India found that about half of all cases of infertility are caused by problems with men[17].
3. Pharmacological treatment approaches
3.1. Hormonal therapies
Gonadotropins, selective oestrogen receptor modulators, and aromatase inhibitors are by far the most regularly used hormonal drugs. Their impact on operative sperm retrieval and subsequent conception rates has been studied, with mixed results. Exogenous testosterone is not used to treat men who want to have offspring because it stops the pituitary gland from making luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which stops spermatogenesis.
Exogenous gonadotropins like FSH and human chorionic gonadotropin (hCG) are designed to mimic the therapeutic properties of FSH and LH, respectively. To increase sperm characteristics and the conception rate, gonadotropin-releasing hormone copies were investigated in individuals with idiopathic infertility[18]. Male infertility caused by hypogonadotropic hypogonadism is now treated with gonadotropins. But over the years, researchers have looked into how well they work in treating idiopathic male impotence.
3.1.1. FSH
FSH is a hormone generated by the anterior pituitary gland that governs reproductive function both in men and women in conjunction with LH. FSH stimulates Sertoli cellular proliferation,causes spermatogonia mitosis, and promotes cellular differentiation up to the round spermatid phase in the testis[19]. Moreover, FSH and testosterone appear to stimulate spermiogenesis by modulating round spermatid adherence to Sertoli cells[20]. Since gonadotropins are a proven treatment for hypogonadotropic hypogonadism[21], human FSH therapy has been tried on people with idiopathic infertility who have normal levels of gonadotropin plasma in the hopes of increasing the number of sperm, the number of spermatogonial cells,and the number of times they get pregnant.
3.1.2. hCG
Spermatogenesis includes sufficient intratubular testosterone quantities[22]. Testosterone causes Sertoli cell development, which leads to a decrease in anti-mullerian hormone expression and the initiation of germ cell meiosis. The impact of hCG is similar to that of LH, resulting in a higher intratesticular testosterone content than in peripheral circulation[23]. hCG is now being used in conjunction with FSH in men with hypogonadotropic hypogonadism and a desire for reproduction. Due to the obvious intratesticular testosterone deficit, FSH on its own is unsuccessful in the beginning and/or maintaining sperm production in such patients[24]. On the other hand, it was found that a single dose of hCG was enough to restore intratesticular testosterone levels and start the process of spermatogenesis[25].
3.2. Microsurgery/epididymovasostomy
This procedure must only be conducted by endocrinologists with competence in microsurgery. Due to its small effect on fertility rates(20%-30%), it is recommended to combine epididymovasostomy with microsurgical epididymal sperm aspiration (MESA).
Cryopreservation of recovered spermatozoa for ICSI[26] is also an option. In the case of normal spermatogenesis[27],epididymovasostomy (testicular biopsy) is done when the epididymis is blocked, either from birth or over time. If ICSI is impossible or ineffective, MESA in conjunction with ICSI is recommended.Another approach is the percutaneous aspiration of sperm from the caput epididymis (PESA)[28]. If a MESA or PESA surgery does not produce spermatozoa, a testicular biopsy with testicular sperm extraction produces just a few motile spermatozoa. It can be done and utilised for ICSI. Ejaculatory ducts or midline prostatic cysts are incised via the urethra[29].
3.3. ICSI and traditional IVF
Whenever the semen quality was significantly below the WHO fourth revision seminal characteristic standards and the fertility rate in prior rounds was lower, regular IVF was generally less efficient[30]. ICSI, a procedure that involves mechanically injecting a single spermatozoon into an egg in vitro to promote fertilization,was established in 1992[31]. While complete fertilization failures have been documented in up to 50% of traditional IVF treatments in partners with intermediate male infertility, it has only been observed in 3% of ICSI couples[32,33]. As a result, ICSI is now used to treat acute male infertility all over the world[34,35]. There are many issues with the rising use of ICSI because it is time-consuming, costly,and entails unsettled problems about gamete damage and progeny health[36,37]. Several studies have found that routine ICSI treatment for sterility that is not caused by the male factor does not improve clinical outcomes[38,39].
4. Barriers to male infertility clinical treatments
There is currently insufficient data on male infertility, as well as impediments to diagnosis and treatment. Infertility care is facilitated by closeness to local and regional assisted reproductive technology centers, as well as, ideally, male and female fertility doctors. In terms of population density, the distribution of assisted reproductive technology centres for males and females of reproductive age varies greatly[40]. In these situations, general urologists may be the only alternative, as they lack expertise in or interest in male reproduction.This, in turn, alters the interplay among male and female reproductive specialists, potentially affecting assisted reproductive technology outcomes. These restrictions not only decrease healthcare coverage for men who have been diagnosed with infertility but also reduce the likelihood of a diagnosis of subfertility in men who have not been actively pursuing assisted reproductive technology services.The lack of compulsory health insurance for the diagnosis and therapy of male infertility is among the most significant problems in evaluating health care services for male infertility. The financial cost of diagnosing and treating male infertility is substantial.In addition to limiting access to infertility care for a substantial proportion of patients, the lack of insurance coverage also makes it difficult to track the usage and results of fertility services[41].Couples battling with infertility face a significant obstacle due to a lack of health insurance coverage for infertility care and prognosis.It is, unfortunately, not the only impediment. Education, income level, societal practices, religious beliefs, geographic region, and the accessibility of specialty-trained fertility urologists are all crucial factors in influencing how easily patients can access and acquire infertility treatment. There is a huge opportunity for advancement in male infertility health services research.
5. Herbal approaches for the treatment of male infertility
India has a vast array of medicinal herbs that have been used since ancient times. Naturopathy, an Indian system of medicine, is a complete technique utilised in the subcontinent of India. It uses food and herbal remedies to repair the body and promote natural protection in the face of health problems. Indian traditional medicine uses a wide range of plants, plant products, and plant extracts to treat several ailments, including high blood pressure, diabetes, and gastritis, including sexual reproductive health issues[42,43]. The extracts extracted from various parts of these plants aid in improving spermatogenesis and are referred to as aphrodisiacs[44], some of which have been described below. Several herbal supplements were included in the combination, some of which had been demonstrated to have antioxidant action[45]. More research is needed to figure out if herbal supplements should be used in assisted reproduction and to find out more about how the molecules in the supplements work[46].
5.1. Withania (W.) somnifera
W. somnifera is cultivated as a medical crop, with the whole plant or various sections used for therapeutic reasons. The roots of W.somnifera are often used as an aphrodisiac[47]. Multiple studies have demonstrated that it has antioxidant properties and suppresses lipid peroxidation in sperm cells[48], which is thought to be a major contributor to idiopathic male infertility. Furthermore, W. somnifera has indeed been linked to the restoration of sex hormones in infertile men who are under mental, physiologic, or even both types of stress, indicating that it possesses adaptogenic properties[49]. So, W.somnifera can help men who are having trouble getting pregnant by taking care of multiple problems at once.
5.2. Mucuna (M.) pruriens
Ten distinct types of research looked at the effect of M. pruriens on sperm parameters in people who had idiopathic infertility in vitro. The findings of the investigations revealed that consuming M. pruriens greatly enhances sperm count, whereas thioacetamide medication significantly decreases it. Sperm count and motility are two factors to consider. According to research, M. pruriens can correct morphological flaws in sperm to some extent, and none of the investigations found any negative effects. Seeds of M. pruriens have been proven to enhance semen quality, boost serum dopamine,adrenaline, noradrenaline, testosterone, and LH levels, and correct disturbed seminal plasma amounts of alanine, citrate, glyceryl phosphorylcholine, histidine, and phenylalanine in infertile men[50].
5.3. Tribulus (T.) terrestris
The Zygophyllaceae family's T. terrestris has been used to treat sexual dysfunction with considerable success. In human and animal studies, T. terrestris extract has been demonstrated to improve libido and spermatogenesis. T. terrestris enhances various sex hormones due to the presence of protodioscin in the extract[51]. Through 5 alphareductase activity, protodioscin in T. terrestris turns testosterone into dihydrotestosterone, which activates Sertoli cells and stimulates the growth of germ cells and the development of seminiferous tubules.This is why T. terrestris is used as a fertility-boosting drug for men[52].
5.4. Emblica officials
According to several studies, antioxidants, flavonoids, and steroids are found in Emblica officinalis Garten, aiding in the prevention of oxidative stress and inflammation, as well as the repair of testicular tissue injury. Antioxidants present in Emblica officials can help prevent the formation of oxidative distress in the testis tissue.Antioxidants, like vitamin E and vitamin C, help to reduce the damage done by free radicals and make all of these factors stronger.They are also good at preventing male infertility[53].
5.5. Eurycoma (E.) longifolia
E. longifolia Jack, also known as 'Tongkat Ali," yields a herbal concoction that is widely used to improve sexual activity and conception[54]. Numerous animal research studies[55] back up the aphrodisiac and testosterone-boosting characteristics of E. longifolia root extract. Clinical tests have also shown that E. longifolia can raise the amount of testosterone in the blood, treat erectile dysfunction,and help treat diseases caused by not having enough androgen[56].
5.6. Glycyrrhiza glabra
Glycyrrhiza glabra root extract can also help with male infertility by promoting spermatogenesis, because it raises testosterone levels,which causes sperm production. Erectile dysfunction is treated with Glycyrrhiza glabra roots[57].
5.7. Other herbs
Apart from the herbs described above, there is a long list of herbs that can aid with male infertility, some of which are summarised in Table 1.
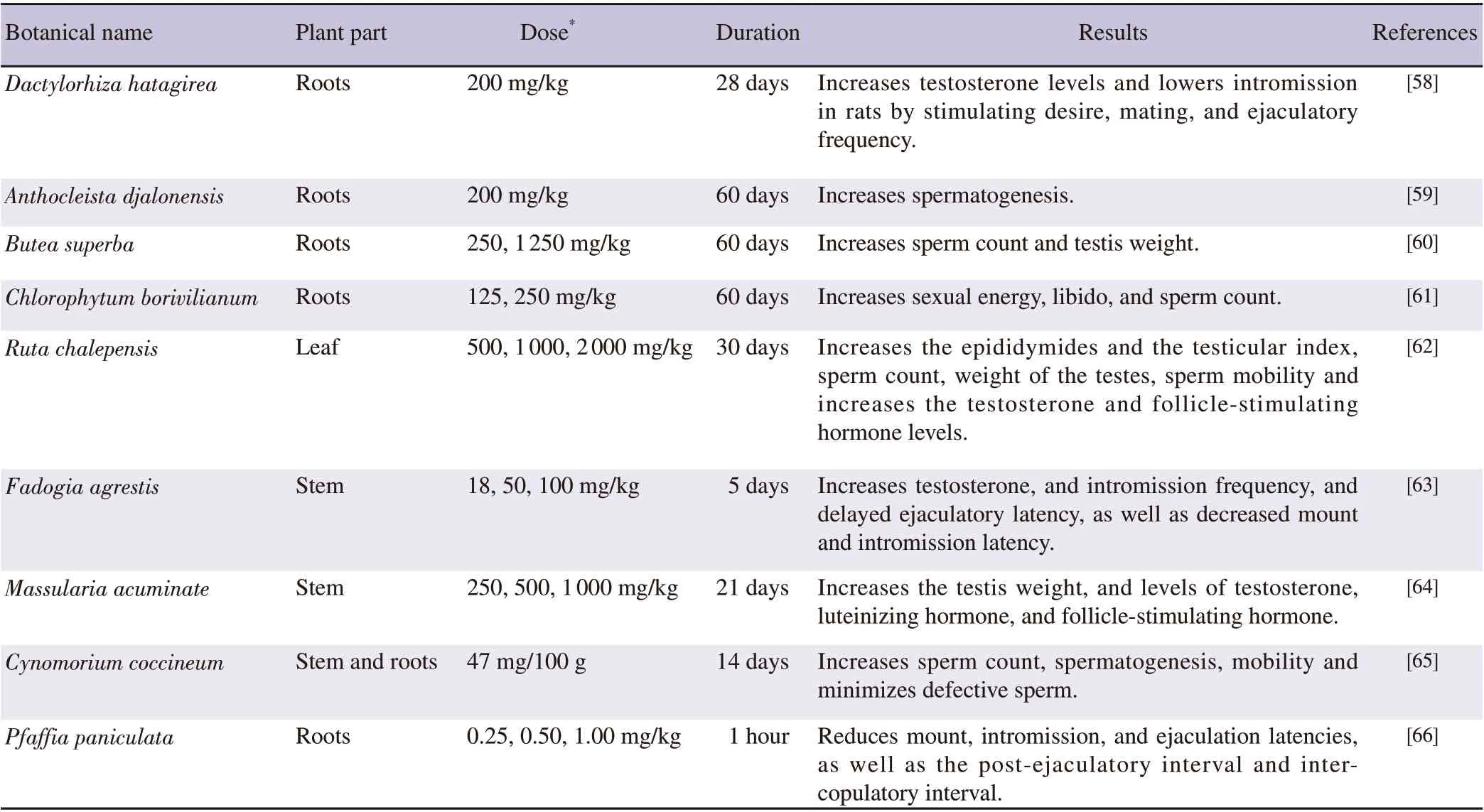
Table 1. Summary of other different herbs, including which parts are used, how much, how long, and how they affect male infertility.
6. Conclusions
Infertility is a common problem that affects more than 70 million people worldwide. The illness has been linked to several lifestyle decisions and hereditary concerns. While poor general health has been linked to infertility, it has also been shown that infertility is linked to an increased risk of several cancers. Due to the health risks,current infertility has minimal power and comes at great expense to treatments. To make headway in this area, after a sequence of standardised safety experiments in animal models, the viability of the plant extract and/or its medication formulation must be studied in people. Given the enormous population of infertile people who aspire to have their genetic offspring, the reward to society will be promising. The expensive expense of synthetic drugs for treating various forms of testicular dysfunction, such as reduced sexual functioning and desire, inadequate sperm function and generation,as well as germ cell growth, has necessitated this paradigm change.Organic, naturally occurring substances are becoming more popular again and having changes in sexual behavior, vitality, neuroendocrine control, functional or structural characteristics of various hormones,as well as qualitative and quantitative improvements in semen and sperm shape and motility have a long-term influence on male reproductive health. The biomedical study should delve further to uncover additional secret processes, through which a plethora of herbs may be used to fight male infertility, which is becoming a huge threat to future generations.
Conflict of interest statement
The authors declare that there is no conflict of interest.
AcknowledgementsWe are grateful for the Pharmacy Department at Pranveer Singh Institute of Technology that helped us in writing this review article.
Funding
The study received no extramural funding.
Authors’contributions
The data was acquired, and the document was designed by Dr.Pranay Wal, and Dr. Ankita Wal. The manuscript was written by Himangi Vig and Ashutosh Pandey. The work was read, edited, and rewritten by Rohini Karunakaran and Biswajit Dash.
 Asian Pacific Journal of Reproduction2022年4期
Asian Pacific Journal of Reproduction2022年4期
- Asian Pacific Journal of Reproduction的其它文章
- Reproductive health and rights in the COVID-19 era: Why and how are rights and choices still the answer?
- Assisted reproduction in the COVID-19 era: Dilemmas and conundrums
- Testicular vascularization at two locations in relation to hormonal levels, and pixel echotexture in bulls at different ages
- Season modulates endocrinological profiles and sex behavioural characteristics in indigenous male goats under tropical humid island ecosystem
- Impact of geographical and seasonal temperature on sperm parameters in Indian men who were partners in subfertile couples - A retrospective analysis
- Iron supplementation for non-anaemic pregnant women and the incidence of hypertensive disorders in pregnancy: A systematic review and meta-analysis