
Cancer risk in relatives of BRCA1/2 pathogenic variant carriers in a large series of unselected patients with breast cancer
2023-03-16 08:19:54JiamingLiuLuYaoJieSunLiHuJiuanChenJuanZhangYeXuYuntaoXie
Cancer Biology & Medicine 2023年2期
Jiaming Liu, Lu Yao, Jie Sun, Li Hu, Jiuan Chen, Juan Zhang, Ye Xu, Yuntao Xie
Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Familial & Hereditary Cancer Center, Peking University Cancer Hospital & Institute, Beijing 100142, China
ABSTRACT Objective: The spectrum and risk of cancer in relatives of BRCA1/2 pathogenic variant carriers in the Chinese population have not been established.
KEYWORDS BRCA1 variant; BRCA2 variant; cancer risk in relatives; Chinese breast cancer patients; family history of cancer
Introduction
Germline pathogenic variants inBRCA1/2genes result in increased risks of various cancersviaan autosomal dominant pattern of inheritance1.A series of studies on the spectrum and risk of cancer inBRCA1/2pathogenic variant carriers (hereafter referred toBRCA1/2carriers) have been conducted2-18.It is well-known thatBRCA1andBRCA2carriers are at increased risk for breast and ovarian cancers,andBRCA2carriers are at increased risk for pancreatic and prostate cancers2,6,7,9-11,16-18.The cancer risks and spectra appear to differ betweenBRCA1andBRCA2carriers; specifically, the risk for ovarian cancer inBRCA1carriers is higher thanBRCA2carriers2,7,17, and the risks for pancreatic and prostate cancers inBRCA2carriers may be higher thanBRCA1carriers7,9-11,18.The associations betweenBRCA1/2carriers and other cancers, such as colorectal and gastric cancers, have not been established, thus warrant further investigation3-6,11-15,17,18.
Most previous studies involvingBRCA-associated cancer have focused onBRCA1/2carriers; however, a limited number of studies have examined the cancer risk and spectrum in relatives ofBRCA1/2carriers.One study reported that relatives ofBRCA1andBRCA2carriers have an increased risk for breast and ovarian cancers, and relatives ofBRCA2carriers also have an increased risk for pancreatic cancer19.
In addition, the data regarding the cancer risks in relatives ofBRCA1/2carriers are largely based on Western populations; scant data exists that pertains to Chinese populations.Chinese individuals have significantly different cancer spectra and risks compared with Western individuals, with relatively lower risks of breast and prostate cancers and relatively higher risks of gastric, esophageal, and liver cancers20,21.Moreover, the spectrum ofBRCA1/2variants in Chinese women is different from Western women, with approximately 30% of variants not present in Caucasian women22-24.Therefore, the cancer risks in relatives ofBRCA1/2carriers in Chinese women might be different from Caucasian women.In the present study we aimed to clarify and characterize the spectra and risks of cancers in relatives ofBRCA1/2carriers in a large series of unselected Chinese patients with breast cancer.
Materials and methods
Study population
Between October 2003 and May 2015, a total of 10,341 consecutive patients with breast cancer who were treated at the Breast Center of Peking University Cancer Hospital & Institute were enrolled in a breast cancer database.All patients were confirmed to have breast cancer based on preoperative biopsy or postoperative histologic examination.BRCA1/2germline variants were determined in all patients by next-generation and/or Sanger sequencing, or multiplex ligation-dependent probe amplification, as described previously25-27.All of theBRCA1/2variants have been listed in detail in previous studies25-27.TheBRCA1/2status in 438 patients could not be determined due to insufficient quantity or poor quality of genomic DNA.Therefore, 9903 patients with breast cancer were ultimately enrolled in this study.Among these patients, four carried pathogenic variants in both theBRCA1andBRCA2genes, and were consideredBRCA1carriers at the time of analysis.
Variables, including demographics, clinicopathologic characteristics, and a family history of cancers, were extracted from the breast cancer database, and uncertain family history was confirmed and supplemented through telephone calls or outpatient visits.
Written informed consent was obtained during hospitalization from all patients whose clinical information and blood samples could be used for research, including genetic testing.The study was performed in accordance with the Declaration of Helsinki.Ethical approval for this study was obtained from the Ethics Committee of Peking University Cancer Hospital &Institute (Approval No.2011KT12).
Definitions
BRCA1/2variants are considered pathogenic when classified as pathogenic or likely pathogenic.Variants with uncertain significance (VUS) or likely benign or benign are considered non-pathogenic based on current American College of Medical Genetics and Genomics guidelines.Only patients with pathogenic variants were defined as carriers; other patients were considered to be non-carriers.A family history of cancers referred to cancers that occurred in first-,second- and third-degree relatives of the participants in our study.The cancer history of the participants and further relatives were not included in the analysis.A history of cancer in any relative that corresponded to the cancer in a study participant was regarded as a positive family history.Considering data accessibility, we used the family of the participants but not individuals as the unit with which to analyze the cancer risks of relatives; thus, cancer risks in relatives were calculated based on the family history of the study participants.Of note, a very small fraction of patients may have come from the same family, and such families may have been counted more than once.For convenience, related cancers with a low incidence were merged together for the analysis.For example, lymphoma included Hodgkin’s lymphoma and non-Hodgkin’s lymphoma, and urothelial carcinoma included bladder cancer and cancers of the ureter and urethra.Furthermore, fallopian tube cancer was considered ovarian cancer.
Statistical analysis
We analyzed all types of cancer with positive family history counts equal to or greater than five amongBRCA1/2carriers, and those with counts less than five were summarized as “other cancers”.Continuous and categorical variables are described as the means ± standard deviations (SD) and frequencies with a percentage (%), respectively.Student’st-test was performed to analyze differences in continuous variables,the Wilcoxon rank-sum test was used to analyze differences in ordered categorical variables, and the Pearson chi square test or Fisher’s exact test was used to analyze differences in unordered categorical variables.In addition, we calculated relative risks (RRs) with 95% confidence intervals (CIs) for comparison of cancer risks in relatives ofBRCA1carriers,BRCA2carriers, and non-carriers.All statistical analyses were performed using StataSE 15 (StataCorp LP, College Station, TX, USA).Only two-tailedPvalues < 0.05 were considered statistically significant.
Results
Distributions of cancers in relatives of patients with breast cancer
There were 538 germlineBRCA1/2pathogenic variant carriers (209 forBRCA1and 329 forBRCA2) and 9365 non-carriers in this study.The distribution of cancers in the relatives of the patients with breast cancer are presented in Table 1.The incidences ofBRCA1andBRCA2carriers among relatives with 1, 2, and ≥3 cancer types were significantly higher than non-carriers (Table 1).Additionally, the proportion ofBRCA1andBRCA2carriers with 1, 2, and≥3 affected family members was significantly greater than non-carriers (Table 1).Differences in the number of cancer types and cancer-affected members among relatives betweenBRCA1andBRCA2carriers, however, were not significant(Table 1).
Cancer risks in female relatives of BRCA1 and BRCA2 carriers
The most common cancers in female relatives ofBRCA1carriers were breast (33.0%), ovarian (11.5%), and liver (3.8%)cancers, followed by lung and cervical cancers (2.4% each;Table 2).The risks for breast and ovarian cancers in female relatives ofBRCA1carriers were significantly higher than the risks in female relatives of non-carriers (breast cancer: RR = 4.29,95% CI = 3.50-5.27;P< 0.001 and ovarian cancer: RR = 21.95,95% = CI 13.73-35.07;P< 0.001).Furthermore, the risks for liver (RR = 3.73, 95% CI = 1.84-7.58;P= 0.002) and cervical cancers (RR = 2.99, 95% CI = 1.22-7.31;P= 0.030) in female relatives ofBRCA1carriers were significantly higher than female relatives of non-carriers.The cancer risks in female relatives ofBRCA1carriers and non-carriers were not significantly different with respect to gastric, pancreatic, and colorectal cancers(Table 2).The most frequent cancer sites in female relatives ofBRCA2carriers were the breast (32.2%), lung (3.7%), and ovary(2.4%), followed by the cervix and pancreas (1.5% each; Table 2).The risks for breast (RR = 4.19, 95% CI = 3.53-4.98;P<0.001) and ovarian cancers (RR = 4.65, 95% CI = 2.22-9.73;P= 0.001) in female relatives ofBRCA2carriers were also significantly higher than female relatives of non-carriers.Moreover,the risks for lymphoma (RR = 3.16, 95% CI = 1.13-8.83;P=0.046) and kidney cancer (RR = 4.07, 95% CI = 1.22-13.56;P=0.046) in female relatives ofBRCA2carriers were significantly higher than female relatives of non-carriers.The pancreatic cancer risk for female relatives ofBRCA2carriers was marginally but not significantly higher than female relatives of non-carriers(RR = 2.54, 95% CI = 1.02-6.30;P= 0.055).Female relatives ofBRCA1carriers had significantly higher risks for ovarian (RR =4.72, 95% CI = 2.16-10.31;P< 0.001), liver (RR = 6.30, 95% CI= 1.35-29.36;P= 0.016), and any cancers (RR = 1.22, 95% CI= 1.02-1.46;P= 0.032) than female relatives ofBRCA2carriers(Table 2).Differences in the risks for other cancers (liver, gastric,and colorectal cancers) between female relatives ofBRCA1andBRCA2carriers were not significant (Table 2).
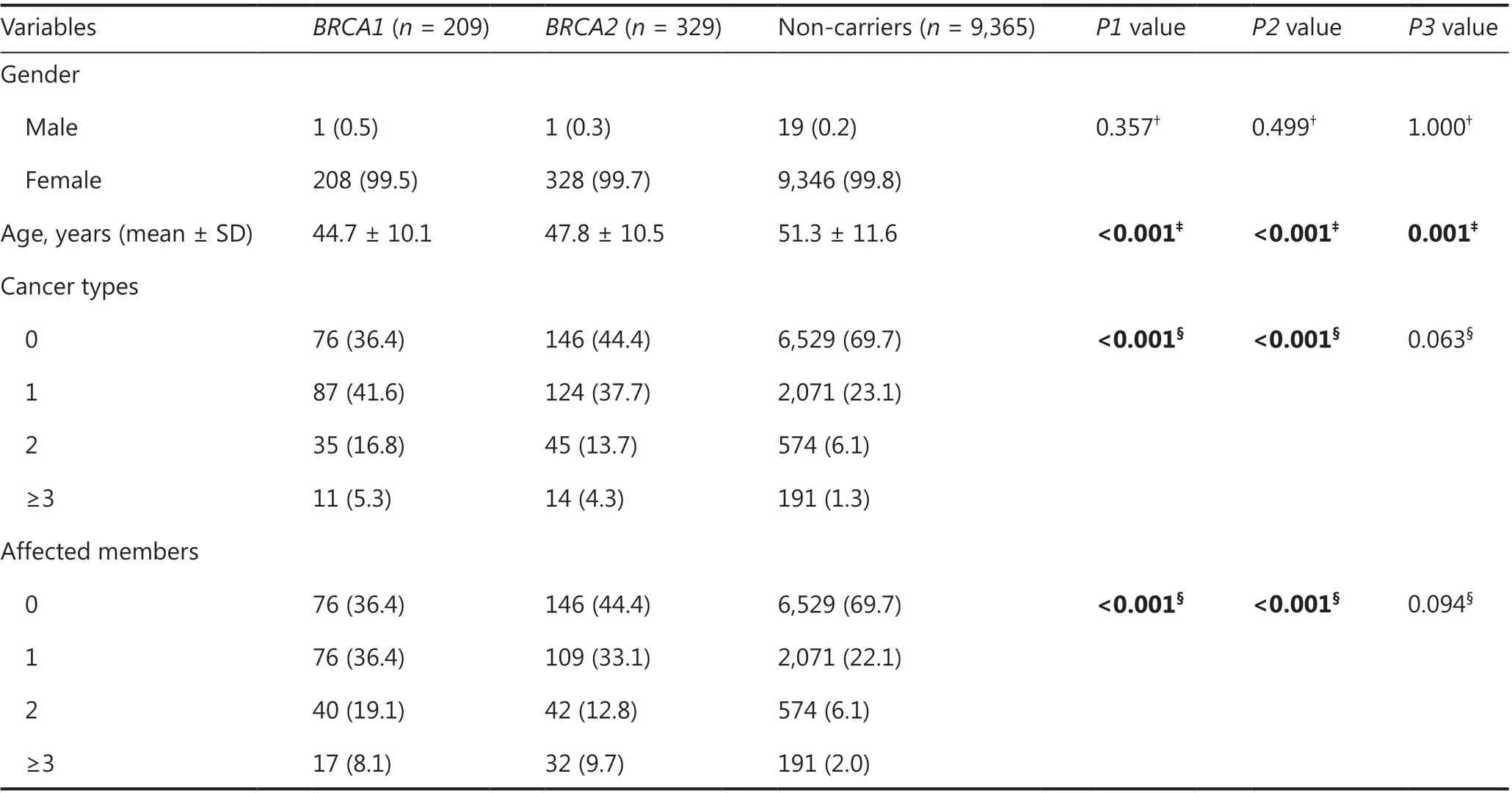
Table 1 Demographics of patients with breast cancer and distributions of cancers in their relatives according to BRCA status
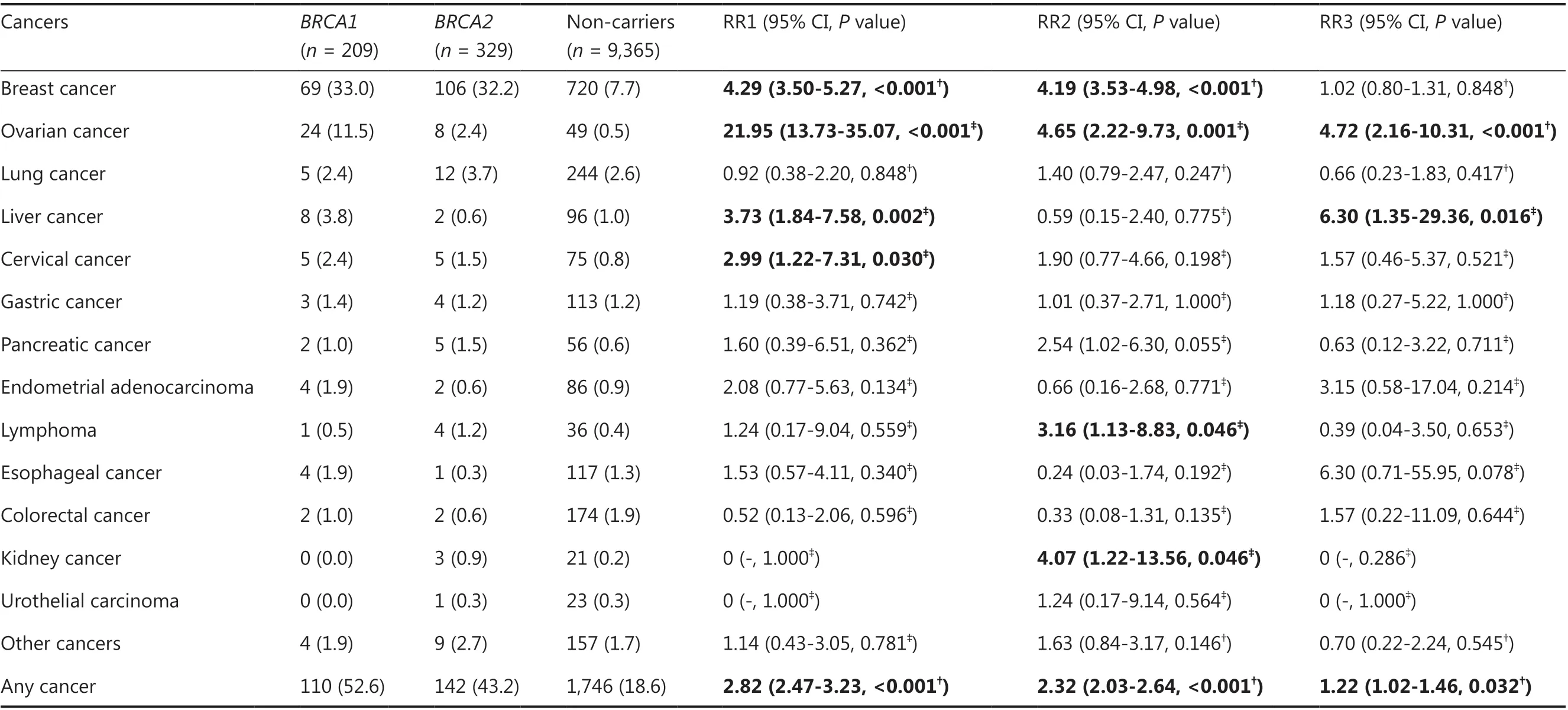
Table 2 Cancer risks in female relatives of germline BRCA1 and BRCA2 pathogenic variant carriers
Cancer risks in male relatives of BRCA1 and BRCA2 carriers
The most common cancers in male relatives ofBRCA1carriers were lung (7.2%), esophageal (6.2%), and gastric cancers(4.8%), followed by liver cancer and lymphoma (2.4% each;Table 3).Male relatives ofBRCA1carriers had significantly higher risks of esophageal cancer (RR = 2.33, 95% CI 1= 0.36-4.00;P= 0.002) and lymphoma (RR = 4.77, 95% CI =1.92-11.86;P= 0.005) than male relatives of non-carriers.No significant differences in the risks of other cancers (gastric,liver, and colorectal cancers) between male relatives ofBRCA1carriers and non-carriers were detected (Table 3).The most common cancers in male relatives ofBRCA2carriers were lung(4.9%), esophageal (4.9%), and liver cancers (4.3%), followed by gastric (2.8%) and pancreatic (2.7%) cancers (Table 3).In contrast, male relatives ofBRCA2carriers had significantly higher risks of pancreatic (RR = 4.34, 95% CI = 2.17-8.68;P=0.001) and prostate cancers (RR = 4.86, 95% CI = 2.20-10.75;P= 0.001) than male relatives of non-carriers.In addition, the risks of esophageal (RR =1.82, 95% CI = 1.11-2.98;P= 0.017),kidney (RR = 4.22, 95% CI = 1.48-11.98;P= 0.020), and breast cancers (RR = 9.49, 95% CI = 1.92-46.83;P= 0.028)in male relatives ofBRCA2carriers were significantly higher than male relatives of non-carriers.Differences in cancer risks between male relatives ofBRCA2carriers and non-carriers,however, were not significant with respect to gastric, liver, and colorectal cancers.No significant differences in any type ofcancer or overall cancer risk existed between male relatives ofBRCA1andBRCA2carriers.
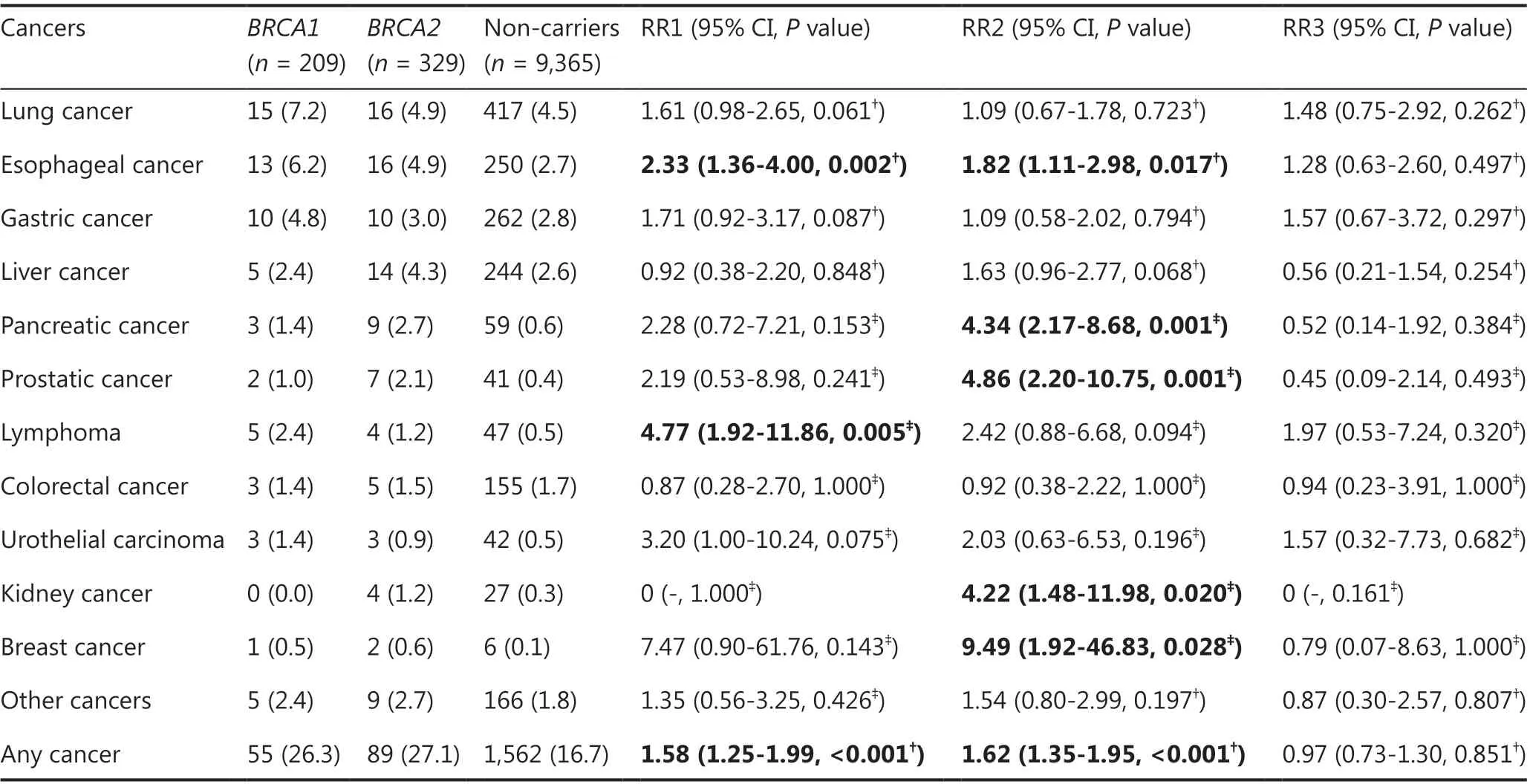
Table 3 Cancer risks in male relatives of germline BRCA1 and BRCA2 pathogenic variant carriers
Discussion
This is the first study to determine the cancer risks in relatives ofBRCA1/2carriers in the Chinese population.This study was based on a family history of cancer in 9903 unselected breast cancer patients.We found that the risks for breast and ovarian cancers in the female relatives ofBRCA1andBRCA2carriers were significantly higher than non-carriers, and the risks for pancreatic and prostate cancers in male relatives ofBRCA2carriers were also significantly increased.
In our study breast cancer was the most common cancer among female relatives of bothBRCA1andBRCA2carriers.Ovarian cancer was the second and third most common cancer among female relatives ofBRCA1(21.95-fold increased risk) andBRCA2carriers (4.65-fold increased risk), respectively.Additionally, our study demonstrated that relatives ofBRCA1carriers have a significantly higher risk for ovarian cancer (RR = 4.72) than relatives ofBRCA2carriers, suggesting that relatives ofBRCA1carriers should be more aware of ovarian cancer thanBRCA2carriers.
Pancreatic cancer is another commonBRCA-associated cancer; however, multiple studies have shown thatBRCA2, but notBRCA1, predisposes individuals to pancreatic cancer3,7,11,19.Our study findings were in agreement to these reports.Indeed,the pancreatic cancer risk was significantly increased in male relatives ofBRCA2carriers (RR = 4.34) but not relatives ofBRCA1carriers.Although pancreatic cancer risks were not shown to be significantly elevated in female relatives ofBRCA1orBRCA2carriers, a trend toward risk for pancreatic cancer was still observed for female relatives ofBRCA2carriers (RR 2.54, 95% CI 1.02-6.30;P= 0.055).Notably, an increased risk for pancreatic cancer was reported in femaleBRCA2carriers in a previous study3.Prostatic cancer is also associated withBRCA3,6-11,17,18,28,29.Similarly, we found a significantly increased risk for prostate cancer in male relatives ofBRCA2carriers (RR = 4.86;P= 0.001), but a non-significant risk in male relatives ofBRCA1carriers (RR = 2.19;P= 0.241); our finding is in agreement with previous studies3,7,9,11,17,18.
In addition, we also found that the risks for liver and cervical cancers in female relatives ofBRCA1carriers, and lymphoma and kidney cancer in female relatives ofBRCA2carriers were significantly increased compared with female relatives of non-carriers.Moreover, the risks of esophageal cancer and lymphoma were markedly elevated in male relatives ofBRCA1carriers, and the risks of esophageal, kidney, and breast cancers in male relatives ofBRCA2carriers were also increased.It should be noted that the sample size of relatives with these cancers was small, and further studies are needed.
The cancer spectrum of relatives of non-carriers was similar to the common cancer spectrum of the general Chinese population20,30, which may accurately reflect cancer risks in the Chinese population.Several common malignancies in the general population, such as gastric, colorectal, and endometrial cancers, were not significantly associated withBRCA1orBRCA2variants in our study, even though correlations between these cancers and variants have been reported4,6,7,11,13.Our study findings did not rule out the possibility of increased risks for these cancers in relatives ofBRCA1/2carriers.
Several limitations should be considered when interpreting our study.Although the study involved a large cohort of unselected patients with breast cancer, theBRCA1/2carrier sample size was not sufficiently large, and some types of cancer were rare after stratification by gender and gene type.Familial cancers were based on a family history of cancers; recall bias was inevitable, especially for the cancer histories among secondand third-degree relatives.
Conclusions
In summary, this study investigated the cancer spectrum and risk in relatives ofBRCA1/2carriers in a Chinese population.Our findings indicated that female relatives ofBRCA1andBRCA2carriers are at increased risks for breast and ovarian cancers.The risk for ovarian cancer in female relatives ofBRCA1carriers is even higher than female relatives ofBRCA2carriers.In addition, male relatives ofBRCA2carriers have increased risks for pancreatic and prostate cancers.Our study may be useful for genetic counseling and cancer risk evaluation for relatives ofBRCA1/2carriers in the Chinese population.
Grant support
This study was supported by grants from National Natural Science Foundation of China (Grant Nos.81974422, 81772824,and 81802635).
Conflict of interest statement
No potential conflicts of interest are disclosed.
Author contributions
Conceived and designed the analysis: Yuntao Xie.
Collected the data: Jiaming Liu, Lu Yao, Jie Sun, Li Hu, Jiuan Chen, Juan Zhang, and Ye Xu.
Contributed data or analysis tools: Jiaming Liu, Lu Yao, Jie Sun, and Ye Xu.
Performed the analysis: Jiaming Liu, Lu Yao, Jie Sun, Li Hu,Jiuan Chen, Juan Zhang, Ye Xu, and Yuntao Xie.Wrote the paper: Jiaming Liu and Yuntao Xie.
 Cancer Biology & Medicine2023年2期
Cancer Biology & Medicine2023年2期
- Cancer Biology & Medicine的其它文章
- Optimization of regional nodal irradiation in the era of sentinel lymph node biopsy
- Association between homologous recombination deficiency and outcomes with platinum and platinum-free chemotherapy in patients with triple-negative breast cancer
- Circular RNAs: implications of signaling pathways and bioinformatics in human cancer
- Conceptualizing the complexity of ferroptosis to treat triplenegative breast cancer: theory-to-practice
- Intercellular transmission of cGAS-STING signaling in cancer
- 2022 Chinese expert consensus and guidelines on clinical management of toxicity in anti-CD19 chimeric antigen receptor T-cell therapy for B-cell non-Hodgkin lymphoma