
Observation on the efficacy of traditional Qigong exercise combined with Tuina manipulations in treating lower cervical disc herniation
2023-06-19 02:32YANGXiaowei楊曉偉SHENGFeng盛鋒WANGSaina王賽娜WANGZhichao王志超CHENGLei成磊GONGChen龔辰WUYi吳藝
YANG Xiaowei (楊曉偉), SHENG Feng (盛鋒), WANG Saina (王賽娜), WANG Zhichao (王志超), CHENG Lei (成磊),GONG Chen (龔辰), WU Yi (吳藝)
Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai 200032, China
Abstract
Keywords: Tuina; Massage; Qigong; Manual Therapies; Cervical Vertebrae; Intervertebral Disc Displacement; Biomechanics;Neck Muscles
Cervical disc herniation (CDH) refers to degenerative changes in the cervical discs, and alternatively, it may occur when external force acts on the neck, causing the annulus fibrosus to rupture and the nucleus pulposus to protrude.This can stimulate or compress the nerve root or spinal cord, leading to symptoms mainly characterized by neck soreness, limited mobility, pain in the shoulders and back, as well as numbness and distending pain in the upper limbs.In modern society,with the acceleration of the pace of life, the incidence of cervical spondylosis has significantly increased and is showing a trend toward younger age groups[1].In the clinical setting, approximately 85% of CDH patients can alleviate symptoms and restore cervical functions through conservative treatments.Recent studies show that intervertebral disc tissue can self-absorb within a certain period.For most patients, after conservative treatments, the symptoms can be significantly relieved,thus avoiding surgery[2].Therefore, conservative treatment is a focus of attention among scholars.Adopting conservative treatments to deal with CDH shows clear efficacy, but the disease is prone to recurrence.This study targeted the biomechanical characteristics of the neck to explore a conservative treatment with clear efficacy and a low recurrence rate for treating CDH.In addition, there is a higher rate of CDH in the C5-C6and C6-C7, collectively referred to as the lower CDH.Hence, the selected cases in this study all suffered from CDH at these two levels.
1 Clinical Materials
1.1 Diagnostic criteria
The diagnostic criteria for CDH referred to theTuina Therapeutics[3].The disease can be diagnosed based on the patient’s medical history, symptoms, physical signs,and cervical MRI examination.
1.2 Inclusion criteria
The patients who met the diagnostic criteria for CDH;aged between 30 and 65 years old, of any gender;agreed not to receive other relevant treatments(including medication) during the treatment period;signed the informed consent form.
1.3 Exclusion criteria
The patients with indications for surgery due to spinal cord compression; with severe diseases of internal medicine; with congenital anomalies of the cervical spine joints.
1.4 Dropout criteria
The patients who could not undergo the required examinations; could not adhere to the treatment plan;withdrew from the study midway; experienced severe adverse reactions; received alternative treatments on their own.
1.5 Statistical methods
The SPSS version 22.0 software was used for data analysis.The measurement data that conformed to normal distribution and homogeneity of variance were expressed as mean ± standard deviation, andt-test was used.Chi-square test was used for nonranked data, and rank-sum test was used for ranked data.P<0.05 indicated statistical significance.
1.6 General data
This study was approved by the Ethics Committee of Longhua Hospital, Shanghai University of Traditional Chinese Medicine, with approval number (2019)LUNSHEN No.28.This study included a total of 120 CDH cases who were treated in the Tuina Department of Longhua Hospital, Shanghai University of Traditional Chinese Medicine between July 2020 and October 2021.They were divided into an observation group and a control group using a random number table method in the order of their visits, with 60 cases in each group.There was no statistical significance in comparing the general data between the two groups (P>0.05),indicating comparability between the two groups(Table 1).The flow chart of this study is shown in Figure 1.

Table 1 Comparison of the general data between the two groups
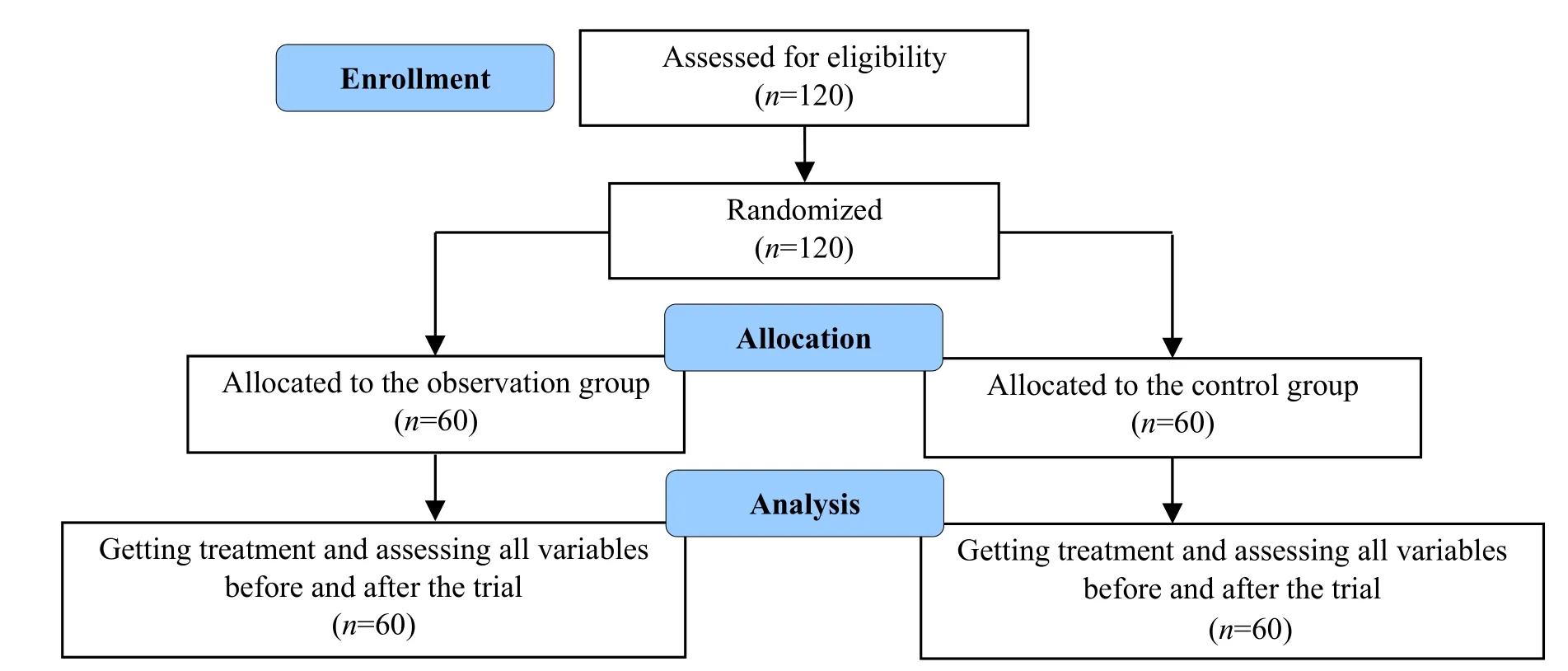
Figure 1 Flow chart of the study
2 Methods
Patients in both groups were given the same Tuina(Chinese therapeutic massage) manipulation treatment.
Relax the neck muscles: The patient took a prone position.The doctor first adopted rolling manipulation to relax the muscles of the patient’s neck and back;then adopted Yi Zhi Chan pushing to knead and relax the trapezius, supraspinatus, infraspinatus, rhomboids,and levator scapulae; and performed kneading and plucking manipulations on the muscles on both sides of the cervical vertebrae to relax the suboccipital muscles.
Manipulation adjustment: Take CDH on the left side as an example.The patient took a supine position, and naturally rotated the cervical spine to the left.The doctor supported the patient’s cheek with the left hand,and palpated along the transverse process of the right side with the right hand to check for any bulging or tender points.Then the doctor opened the right hand,placed the thumb on the patient’s posterior occipital region, and the other four fingers on the patient’s mandibular region; slowly rotated the cervical vertebra of the patient to the left to achieve maximum mobility.When the cervical spine was in a slightly flexing state,the doctor made a sudden but controlled pull with the right hand, which was tilted toward the patient’s nose tip, and usually, a sound of repositioning the cervical spine joint would present.If the patient’s cervical spine is injured, the strength of the doctor’s manipulation and the angle of rotation of the cervical spine should be within the patient’s tolerance.Avoid brute force.
The treatment was given twice a week for a total of 8 weeks.
2.1 Observation group
Additionally, patients in the observation group did traditional Qigong exercise.
Based on literature research, a Qigong exercise was devised to enhance neck mobility and regulate the whole body.We selected the movements from Yi Jin Jing (Sinew-transforming Exercise), Shaolin Neigong(Shaolin Internal Exercise), and Ba Duan Jin (Eightsection Exercise).After consulting experts, we finally included the following eight movements as the intervention plan for this study: supporting the sky with the palms, nine demons drawing their swords, bowing down in salutation and beating a drum, the overlord lifting the ancient cooking vessel, phoenix worshipping the sun, holding the heaven with two hands, turning head to gaze backward, and swinging head to twist the back side to side[4].These eight movements can strengthen the strength of such neck muscles as splenius cervicis, semispinalis muscle, levator scapulae,sternocleidomastoid, scalene muscle, and suboccipital muscle groups (rectus capitis anterior, rectus capitis lateralis, rectus capitis posterior major, rectus capitis posterior minor, obliquus capitis inferior, and obliquus capitis superior muscle) to maintain the stability of the cervical spine.The patients exercised once a day, 20 min each time, for a total of 8 weeks.
2.2 Control group
Patients in the control group did conventional neck exercises in all directions once a day, 20 min each time,for a total of 8 weeks.
3 Observation of Efficacy
3.1 Observation items
3.1.1 Main clinical symptom scores
Visual analog scale (VAS) score: 0-10 points.The higher the score, the severer the pain.
Neck disability index (NDI) score: 0-50 points.The higher the score, the severer the cervical dysfunction.
Neck pain and disability scale (NPAD) score:0-100 points.The higher the score, the more obvious the limited cervical function.
3.1.2 Characteristics of neck muscle groups
As for the transverse section of the cervical spine,which was shown as a segment of CDH on MRI, we used T2-weighed images (Figure 2).The transverse section mainly included four muscles: sternocleidomastoid,semispinalis muscle, splenius capitis muscle, and levator scapulae.To reduce the differences in paraspinal muscle groups caused by individual differences, we used the muscles vertebra ratio (MVr) as an indicator.We performed the semi-quantitative analysis of the fat content at the corresponding level of the paraspinal muscles, which was generally divided into four grades(0-3).Grade 3 indicated severe fatty infiltration with an infiltration rate of ≥50%; grade 2 indicated moderate fatty infiltration with an infiltration rate of ≥25% but<50%; grade 1 indicated mild fatty infiltration with an infiltration rate of ≥10% but <25%; grade 0 indicated normal fatty infiltration with an infiltration rate of<10%[5].
3.2 Efficacy criteria
The efficacy criteria for this study were formulated according to theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[6].
Cured: The symptoms and signs disappeared.
Improved: The symptoms and signs were not obvious,but some accompanying symptoms and signs still presented.
Effective: The symptoms were relieved, and the accompanying symptoms and signs were improved.
Invalid: No improvements in symptoms and signs.
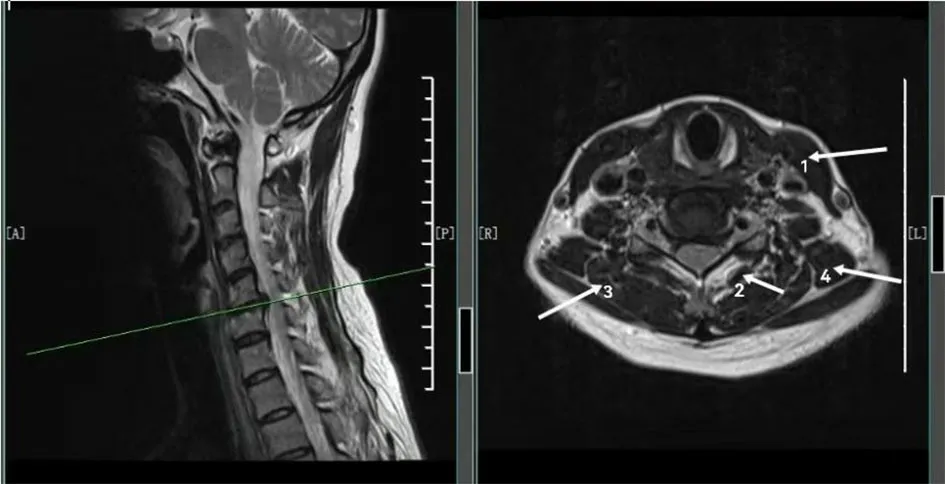
Figure 2 Muscle measurement at the corresponding segment of cervical disc herniation
3.3 Results
3.3.1 Comparison of the clinical efficacy and recurrence rate
After treatment, the total effective rate of the observation group was 95.0%, with a recurrence rate of 8.3%; the total effective rate of the control group was 91.7%, with a recurrence rate of 28.3%.There was no statistical significance in comparing the total effective rate between the two groups (P>0.05), but the recurrence rate in the observation group was lower than that in the control group (P<0.05).Check Table 2 for details.
3.3.2 Comparison of the pain and functional scores
Before treatment, there was no statistical significance in comparing the VAS, NDI, and NPAD scores between the two groups (P>0.05), indicating comparability.After treatment, the VAS, NDI, and NPAD scores of both groups were significantly reduced (P<0.05), and the NDI and NPAD scores of the observation group were significantly lower than those of the control group(P<0.05).Check Table 3 for details.
3.3.3 Comparison of the muscle group characteristics
Before treatment, there was no statistical significance in comparing the MVr between the two groups (P>0.05),indicating comparability.After treatment, the MVr of the sternocleidomastoid, semispinalis muscle, and splenius capitis muscle in the observation group was significantly higher than that before treatment,indicating intra-group statistical significance (P<0.05).There was statistical significance in comparing the MVr of the semispinalis muscle between the two groups(P<0.05).Check Table 4 for details.
Before treatment, there was no statistical significance in comparing the muscle fatty infiltration grading between the two groups (P>0.05), indicating comparability.After treatment, the muscle fatty infiltration grading of the semispinalis muscle and splenius capitis muscle in the observation group decreased (P<0.05), and there was statistical significance in comparing the muscle fatty infiltration grading of the semispinalis capitis between the two groups (P<0.05).Check Table 5 and Table 6 for details.

Table 2 Comparison of the clinical efficacy and recurrence rate between the two groups/case
Table 3 Comparison of the main clinical symptom scores between the two groupsUnit: point

Table 3 Comparison of the main clinical symptom scores between the two groupsUnit: point
Note: VAS=Visual analog scale; NDI=Neck disability index; NPAD=Neck pain and disability scale; compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05.
Group n Time VAS NDI NPAD Observation 60 Before treatment 5.48±0.78 35.80±5.12 51.82±17.33 After treatment 2.71±0.811)12.39±1.291)2)20.34±4.251)2)Control 60 Before treatment 5.52±0.70 36.11±4.58 50.89±18.67 After treatment 3.14±0.741)18.20±1.341)35.62±18.141)
Table 4 Comparison of the MVr between the two groups

Table 4 Comparison of the MVr between the two groups
Note: MVr=Muscles vertebra ratio; compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05.
Group n Time Sternocleidomastoid Semispinalis muscle Splenius capitis muscle Levator scapulae Observation 60 Before treatment 1.03±0.36 0.90±0.23 0.42±0.08 0.37±0.05 After treatment 1.11±0.441)1.04±0.261)2)0.49±0.101)0.40±0.07 Control 60 Before treatment 1.07±0.39 0.88±0.19 0.40±0.07 0.35±0.04 After treatment 1.14±0.52 0.91±0.21 0.39±0.05 0.39±0.05

Table 5 Comparison of the fatty infiltration grading of the sternocleidomastoid and semispinalis muscle between the two groups Unit: case

Table 6 Comparison of the fatty infiltration grading of the splenius capitis muscle and levator scapulae between the two groups Unit: case
4 Discussion
The biomechanical stability of the neck can be divided into endogenous stability and exogenous stability.The former is composed of intervertebral discs,facet joints, and surrounding ligaments, while the latter is composed of the muscles surrounding the spine.As age increases, the ability of intervertebral discs to resist compression gradually decreases.Due to dehydration,the nucleus pulposus becomes less rich and loses its ability to distribute axial pressure to the inner layer of the annulus fibrosus.As a result, most of the load is directly borne by the annulus fibrosus, which can easily cause it to bulge.In addition, the height of the intervertebral disc decreases, and the ligaments become lax, resulting in a decrease in endogenous stability.It is generally believed that the exogenous stability of the spine is more important than the endogenous stability.Losing endogenous stability leads to slower changes in the spine, while losing exogenous stability may result in the inability of the spine to maintain its normal functions.Therefore, the decrease in exogenous stability is considered to be the main basis for the occurrence of CDH[7].The lower part of the cervical spine is in a forward physiological curvature.It joins the backward physiological curvature of the thoracic spine, and bears the maximum load stress.The range of motion for flexion-extension and rotation of the cervical vertebrae is the greatest between C4and C6,gradually decreasing downward.The axis of motion is located at the anterior portion of the lower vertebra.However, the range of motion in the semi-flexedneutral-semi-extended range is significantly greater for C5-C7than for C3-C5.Since this range of motion happens to be the most commonly used in daily life, C5-C6and C6-C7degenerative changes occur earliest and present the most severe clinical manifestations[8].
This study finds that the pain of the patients in both groups is significantly relieved, but in terms of the recovery of cervical function, traditional Qigong exercise shows significant strengths.CDH is mainly caused by the following three factors.The first factor is the reduction of muscle mass, decreased muscle strength, and fatty infiltration in the neck muscles.Cervical muscle atrophy and degeneration are positively correlated with the clinical symptoms of CDH.The shortened length or decreased tension of muscle fibers around the cervical spine makes it difficult for the paraspinal muscles to withstand the load of the cervical spine, leading to cervical instability and clinical symptoms.Among these symptoms, the most common ones are related to the sternocleidomastoid, cervical multifidus muscle,semispinalis capitis muscle, and splenius capitis muscle.Second, increased muscle fatty infiltration leads to a decrease in muscle strength and control over the cervical spine, resulting in cervical pain[9].Third,hypofunction of the paraspinal muscles changes the original biomechanical relationship, leading to increased or uneven loading on such structures as joint capsules, articular cartilage, and intervertebral discs,which in turn causes disc degeneration.The decrease in paraspinal muscles is significantly related to the degeneration of the intervertebral disc, and they are mutually causal and promote each other.The reduction of paraspinal muscles may cause joint instability and changes in spinal curvature as well as spinal sagittal subtype.This condition may alter the stress characteristics of the spine and increase the load on intervertebral discs, which are often concurrent and share risk factors[10].Regular traditional Qigong exercise can increase skeletal muscle strength, increase muscle content, reduce fatty infiltration, and restore the original biomechanical relationship of the cervical spine[11].
Tendon-regulating manipulations are safe and effective for intervertebral disc lesions[12].However,reduction manipulations carry certain risks and thus should be used with caution or avoided, especially for patients with spinal cord compression.Some scholars have conducted relevant clinical research[13]and biomechanical research[14], by which they clearly define the limits of manipulations and suggest that safety should be the top priority when using manipulations,and brute manipulations should be avoided.The therapeutic effect of manipulations is mainly dependent on the following three aspects.Firstly, by adjusting the imbalance of the bony structure and the static stability system of the cervical spine, it can relieve disorders of small joints of cervical vertebrae, release synovial incarceration, increase the pain threshold of muscle trigger points, and thus relieve pain; it can reduce the creep rate and stress relaxation rate of intervertebral discs from a mechanical perspective, thereby changing the stress distribution and viscoelasticity of the intervertebral discs, and improving the stability of the vertebral body[15].Secondly, by improving the contraction strength, work efficiency, and coordination ability of the cervical muscle groups, it can restore the mechanical properties of cervical muscle groups,thereby expanding the effective space of the spinal cord and achieving clinical efficacy[16].Thirdly, the therapeutic effect of tendon-regulating manipulation lies in the process of converting mechanical energy into heat energy, which can increase the blood flow velocity of cervical blood vessels, improve microcirculation, and promote the clearance of metabolic waste and absorption of inflammation, thus accelerating the repair of injuries and achieving the therapeutic goals[17].The effects of manipulation on intervertebral discs are reflected in reducing intervertebral disc creep rate and stress relaxation rate[18], alleviating intervertebral disc pressure[19], altering blood flow dynamics, thus enhancing vertebral stability, and improving intervertebral disc nutrition.Tuina manipulation boasts rapid effectiveness and shortens the treatment course for CDH[20].However, the primary issue currently in clinical settings is that although manipulation therapy has an immediate therapeutic effect, its sustained effectiveness is relatively poor.Doing traditional Qigong exercise allows muscles to undergo static contraction,which is beneficial to restoring the tension and toughness of muscle fibers, increasing arm strength,and enhancing the flexibility and stability of the neck and shoulders, thus effectively reducing the recurrence rate of cervical spondylosis[21]and alleviating the pain caused by excessive muscle load.According to a study by some researchers[22], exercise for cervical vertebrae can enlarge the intervertebral foramen and improve the relative position relationship between the nerve root and the intervertebral disc.Through static muscle strength training, the stability and coordination of the neck muscle groups can be improved, which can prevent cervical joint inflammatory reactions caused by some unstable factors and thus reduce muscle strain and joint tissue damage caused by cervical internal and external dynamic balance disorders, achieving the therapeutic and preventive effect for CDH[23-24].
The combination of traditional Qigong exercise and Tuina manipulations for the treatment of CDH aims to restore the dynamic and static balance of the neck,thereby restoring the normal physiological state of cervical vertebrae.Traditional Qigong exercise is simple and easy to learn and can be done conveniently in multiple dimensions and angles to exercise the muscles of the neck, back, and upper limbs, which is beneficial to the overall functional recovery of the spine muscles and joints.The results of this study indicate that the combination of Tuina manipulations and traditional Qigong exercise can significantly relieve the clinical symptoms of CDH and improve the cervical range of motion.This comprehensive therapy shows better efficacy than single Tuina manipulations.It also helps to strengthen joint stability and reduce recurrence, which and thus worth promoting.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by the Specialty Construction Project in Weak Areas of Traditional Chinese Medicine in Shanghai (上海市中醫(yī)薄弱領(lǐng)域?qū)?平ㄔO(shè)項目,No.BRZK2016001).
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 30 May 2022/Accepted: 22 August 2022
猜你喜歡
環(huán)境保護與循環(huán)經(jīng)濟(2021年7期)2021-11-02
中小學(xué)校長(2021年7期)2021-08-21
中國畢業(yè)后醫(yī)學(xué)教育(2020年5期)2020-12-06
學(xué)生導(dǎo)報·初中版(2020年1期)2020-05-03
中華建設(shè)(2019年7期)2019-08-27
車迷(2017年12期)2018-01-18
中國衛(wèi)生(2016年3期)2016-11-12
制冷技術(shù)(2016年6期)2016-03-08
天津護理(2015年4期)2015-11-10
 Journal of Acupuncture and Tuina Science2023年3期
Journal of Acupuncture and Tuina Science2023年3期
- Journal of Acupuncture and Tuina Science的其它文章
- Electroacupuncture stimulation attenuates corpus striatum white matter injury in rats with cerebral ischemia by inhibition of Nogo-A/NgR pathway
- Study on the antipyretic mechanism of large pushing Tianheshui for young rabbits with endotoxin-induced fever
- Effects of different moxibustion time on knee cartilage morphology and the expression of TNF-α and IL-10 in rats with knee osteoarthritis
- Effects of horse-riding squat exercise plus Governor Vessel-regulating Tuina therapy on static balance function in patients with stroke
- Clinical study of treating somatoform pain disorder with the combination of electroacupuncture and duloxetine
- Clinical observation of Tuina combined with Bu Zhong Yi Qi Tang in the treatment of rectocele