
Application of early enteral nutrition nursing based on enhanced recovery after surgery theory in patients with digestive surgery
2023-10-21 01:03YanRuShaoXiaKeLiHuaLuoJinDongXuLiQianXu
Yan-Ru Shao, Xia Ke, Li-Hua Luo, Jin-Dong Xu, Li-Qian Xu
Abstract
Key Words: Enhanced recovery after surgery; Extremely early postoperative enteral nutrition nursing; Gastrointestinal surgery; Tracheal intubation under general anesthesia; Agitation during recovery; Recovery of gastrointestinal function
INTRODUCTION
Gastrointestinal tumor is a common malignant tumor, which is usually treated by surgery or radiotherapy and chemotherapy, which can effectively reduce the clinical symptoms and improve the prognosis. Relevant studies have pointed out that patients with digestive tract tumors have psychological fluctuations due to long-term illness and worry about surgical risks. In addition, preoperative fasting and water prohibition before surgery reduce the tolerance of the body, which is not conducive to the operation[1]. It has been reported that enhanced recovery after surgery (ERAS) can reduce the stress response after surgery and improve the prognosis of patients[2]. ERAS is a group of surgical models that use a variety of efficient techniques during the perioperative period to lessen the stress and trauma of surgery and hasten the postoperative rehabilitation of patients. These strategies are backed by evidence-based medical data. Early postoperative nutritional support is the core concept of ERAS. Early feeding can not only stimulate gastrointestinal peristalsis and promote the recovery of gastrointestinal function, but also nourish the intestine, maintain the integrity of intestinal mucosa structure and function, reduce the balance of intestinal flora, and thus reduce the incidence of wound infection and other complications[3]. Previous reports also pointed out that the application of ERAS in the perioperative intervention of patients undergoing surgical treatment can promote postoperative recovery[4]. Consequently, the purpose of this research is to notify clinical interventions for patients with this disease by investigating the impact of ERAS-theorized extremely early postoperative enteral nutrition nursing on post-anesthesia agitation and gastrointestinal recovery following tracheal intubation for general anesthesia.
MATERIALS AND METHODS
Clinical data
The data of 126 patients with digestive surgery from May 2019 to February 2022 were retrospectively analyzed. According to different nursing methods, they were divided into control group and observation group, with 63 cases in observation group and 63 cases in control group. As can be shown in Table 1, there was no statistically significant difference in clinical data between the two groups (P> 0.05).

Table 1 Comparison of clinical data between the two groups
Inclusion criteria
(1) Patients who fulfilled the diagnostic criteria for colorectal and gastric cancer[5]; and (2) The clinical data was complete.
Exclusion criteria
(1) Patients with contraindications to enteral nutrition; (2) Patients with cognitive dysfunction or mental illness; (3) Patients with severe cardiac, liver and renal dysfunction; (4) Survival time ≤ 3 mo; and (5) Patients with other malignant tumor diseases.
Methods
The patients in the control group underwent standard perioperative nursing care, with venous access established before surgery, vital signs monitored, and standard anesthesia and resuscitation protocols used to keep diastolic and systolic blood pressure at 60-80 mmHg and 90-100 mm Hg, respectively, throughout the procedure. Patients were given infusion of conventional fluids and a routine indwelling catheter. After operation, parenteral nutrition support was performed before anal exhaust. After exhaust, liquid food was taken and analgesic was injected. Patients were instructed to get out of bed according to their wishes.
According to relevant guidelines[6], the observation group was treated with ERAS-based extremely early postoperative enteral nutrition nursing intervention based on the control group: (1) Preoperative nutritional therapy: Patients with NRS2002 score ≥ 5 points were given nutrition treatment 7-10 d before operation. Patients without diabetes history took Ensure Nutrison (enteral nutrition powder) orally, and patients with diabetes history took Glucerna SR orally. Preoperative nutritional requirements were HGB ≥ 80g/L, albumin ≥ 32g/L, and lymphocyte count returned to normal; (2) Preoperative education: Individualized face-to-face education, lectures, wall newspapers, knowledge manuals and other ways were used to publicize ERAS and related knowledge of the perioperative period of gastric cancer, and visceral function reserve. Smokers and alcoholics should quit smoking for at least 2 wk and abstain from alcohol for 4 wk before surgery; (3) Intraoperative treatment: Thermal insulation blanket was used to maintain the patient’s central body temperature > 36℃; Restrictive rehydration and prophylactic use of antibiotics to prevent postoperative infection; The indwelling catheter and drainage tube were routinely placed and removed as soon as possible after surgery; (4) Tubes intervention: The patient was placed in an appropriate position. Before the patient was awake, the supine position was taken, the head was tilted to one side. After the patient was awake under general anesthesia and the blood pressure was stable, the patient could be changed to the semi-decumbent position. Explained again the importance of tube retention, strengthened the patrol at night, observed whether the tube was in place and unobstructed, and prevented the tube from being pulled out accidentally during sleep; Removed the gastric tube after the anus exhausts; (5) Extremely early postoperative enteral nutrition nursing: Strictly grasped the “three degree principle” of enteral nutrition, namely, temperature, speed, concentration; Followed the principle of step by step, from less to more, from slow to fast, from thin to thick; The temperature of liquid food should be controlled at 38℃-40℃ to prevent spasmodic abdominal pain and diarrhea caused by too low temperature, and damage of digestive tract mucosa caused by too high temperature. After eating, the patient was observed for abdominal distension, abdominal pain, diarrhea, nausea, vomiting and other discomfort. Aspiration pneumonia was the most serious complication in patients with enteral nutrition. Patients should be placed in the semi-decumbent position during feeding, and intestinal sounds should be observed at any time to avoid gastric retention, which was helpful for the prevention of aspiration. If the patient was found to inhale by mistake, immediately stopped feeding, quickly sucked out the liquid from the trachea, and encouraged the patient to cough hard, and if necessary, performed tracheoscopy to remove foreign matters in the trachea; (6) Postoperative treatment: Postoperative analgesia pump was given to relieve pain. From the first day after operation, massaged bilateral Zusanli acupoints twice a day, 5 min/time, preferably with local feeling of soreness, numbness and swelling, and massaged the opposite side in the same way. Get out of bed (sitting, standing, walking) one day after surgery; Gastric tube was extracted 3-4 d after surgery, catheter was extracted one day after surgery, and abdominal cavity drainage was extracted as soon as possible after surgery. Oral care was performed twice a day, instructing patients to take deep breaths to relieve nausea, vomiting and other discomfort; and (7) Postoperative follow-up: The anesthesia follow-up nurse evaluated patients’ consciousness, cognitive impairment and other complications after anesthesia at the bedside on the first day after surgery, and the ward nurse guided patients to change dressing or remove stitches and diet at the time of discharge. Within 3-10 d after discharge, a second follow-up visit was conducted by phone or WeChat, and patients were instructed to seek medical treatment in emergency department in time they felt unwell, and to be readmitted to hospital if necessary.
Observation indicators
(1) Comparing the two groups' waking times, spontaneous respiration recovery times, extubation times, postoperative eye opening times, and directional force recovery times allowed us to identify relevant indices of awakening quality; (2) Agitation: Riker's Sedation-Agitation Scale (SAS)[7] was used to assess agitation in patients, and scores ranged from 1 to 7. 7 points: Hazardous agitation, yanking the endotracheal tube, attempting to remove numerous tubes, scaling the window bar, yelling at the nurses, and wriggling in bed; 6 points: Very agitated, requiring a protective restraint and many verbal warnings to stop, and biting endotracheal intubation, 5 points: Agitation, anxiety or physical restlessness, can be quiet after being dissuaded by verbal prompts; 4 points: Quiet, easy to wake up, obey instructions; 3 points: Calm, drowsy, language stimulation or gentle shaking can wake up, and can obey simple instructions, but quickly fall asleep; 2 points: Very calm, responsive to physical stimulation, unable to communicate and obey instructions, and able to exercise independently; (3) Gastrointestinal function: The two groups' times for the first half-fluid feeding after surgery, the first postoperative exhaust time, the first postoperative defecation time, and the time for intestinal sound recovery were all compared; (4) Nutritional status: D-100TMhemoglobin detector (Bio-Rad company) was used to detect the hemoglobin A1c level on 1stand 3rdday after surgery by high pressure liquid chromatography. Beckman Coulter AU automatic biochemical analyzer and ALB detection kit were used to detect the albumin level of patients on the 1stand 3rdday after operation by bromocresol green method; Beckman Coulter AU automatic biochemical analyzer and GLUC detection kit, provided by Shanghai Kehua Bioengineering Co., LTD., were used to detect fasting blood glucose on 1stand 3rdday after surgery by hexokinase endpoint method; and (5) Adverse reactions: The incidence of anesthetic associated adverse responses such as hypoxemia and chills following surgery was recorded.
Statistical analysis
The data collected was analyzed using SPSS22.0. To facilitate comparisons across groups, theχ2test was used to convert the numerical counts to percentages. After determining that the data were normally distributed, the measurements were stated using mean ± SD, and thet-test was used to compare the groups. When comparing two groups, a value ofP< 0.05 was deemed significant.
RESULTS
Comparison of related indexes of recovery period between the two groups
When compared to the control group, the awake duration, spontaneous breathing recovery time, extubation time and postoperative eye-opening time were all considerably shorter (P< 0.05). As can be seen in Figure 1, There was no significant difference in the recovery time of orientation force between the two groups (P> 0.05).
Comparing the two groups' recovery agitation.
Figure 2 shows the statistical significance (P< 0.05) that the lower SAS score of the observation group compared to the control group.
Comparison of gastrointestinal function recovery across groups
The observation group's recovery times for intestinal soundness, first postoperative exhaustion, first postoperative defecation, and first half-fluid eating were all shorter compare to control group (P< 0.05), as indicated in Figure 3.
Postoperative nutritional status comparison between groups
On postoperative days 1 and 3, the observation group had greater albumin and hemoglobin levels, which were higher while the fasting blood glucose value was lower compare to the control group's (P< 0.05) (Figure 4).
Comparison of Anesthesia-related adverse responses in both groups
As can be shown in Table 2, there was no statistically significant difference in the occurrence of adverse responses to the anesthesia between the two groups (P> 0.05).

Table 2 Compares the incidence of adverse responses associated to anesthesia in the two groups, n (%)
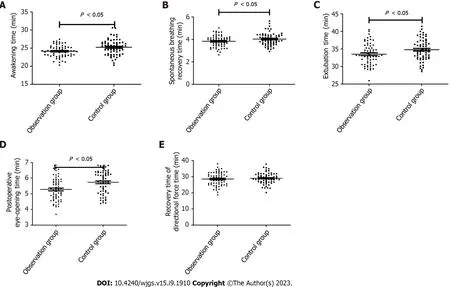
Figure 1 Comparison of relevant recovery duration indices for the two groups. A: Awakening time; B: Spontaneous breathing recovery time; C:Extubation time; D: Postoperative eye-opening time; E: Recovery time of directional force time.
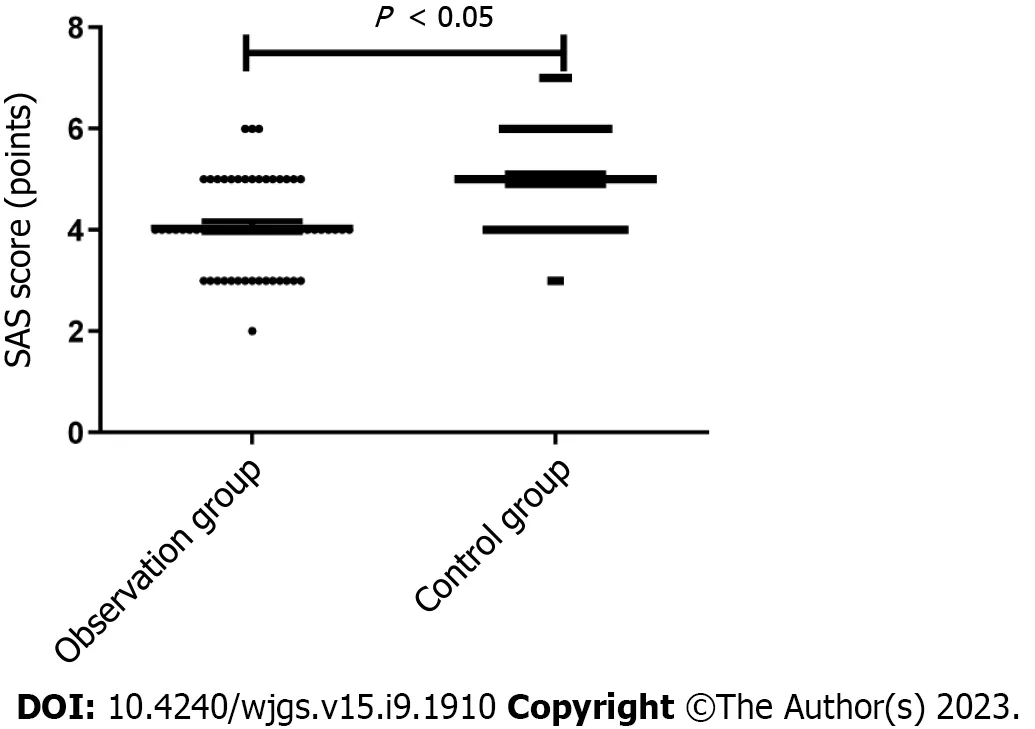
Figure 2 Incidence of agitation among these two groups throughout the recovery period. SAS: Riker's Sedation-Agitation Scale.
DISCUSSION
The surgical treatment of digestive tract tumors can bring pain and traumatic stress to patients during anesthesia, invasive operation and other processes, and the stress reaction will destroy the body immune function, increase the release of inflammatory mediators, and interfere with the balance of water and electrolyte, which can delay the recovery, increase postoperative complications, and prolong the hospital stay[8]. According to relevant research, patients' stress responses after surgery have been shown to be significantly enhanced by ERAS intervention[9,10]. Through a coordinated effort of evidence-based perioperative treatment strategies, ERAS may reduce the physiological and psychological impact of surgery on patients, allowing them to recover more quickly. The ERAS idea, according to the aforementioned research, uses multi-mode analgesia, which increases the analgesic impact, prevents the transmission of stress signals, and lessens the stress response[11,12]. This study found that the extremely early postoperative enteral nutrition intervention based on ERAS theory for patients undergoing gastrointestinal surgery can reduce the stress response, which is consistent with the above research results. The reason for this is that the perioperative stress response of patients is reduced and the rehabilitation process is shortened through the integration of nutritional support, anesthesia, and other nursing measures in the extremely early postoperative enteral nutrition intervention based on the ERAS theory[13]. Additionally, this study discovered that the SAS score was lower in the observation group than in the control group and that the awakening time, spontaneous breathing recovery time, extubation time, and postoperative eye-opening time of the observation group were significantly shorter than those of the control group. These findings suggest that the extremely early postoperative enteral nutrition intervention based on ERAS theory can reduce the level of agitation and improve the quality of awakening. This is mainly because ERAS concept, through improving perioperative nursing measures such as pain control and injury control, combines epidural block technology with general anesthesia to reduce patients’ perioperative stress response, effectively reduce patients’ myocardial oxygen consumption, and thus promote postoperative recovery.
Patients with digestive tract tumors are affected by tumor invasion and various factors secreted by tumor cells, which can affect the nutritional status of the body. In addition, the patients are in a state of high energy consumption due to surgical trauma, which is prone to the risk of malnutrition, resulting in poor prognosis[14,15]. The results of this study showed that the nutritional status of the body for patients in the recovery period after tracheal intubation under general anesthesia could be improved by the extremely early postoperative enteral nutrition intervention based on the ERAS theory, as measured by albumin and hemoglobin levels on the first and third postoperative days and by the fasting blood glucose value than those of the control group. This is mainly because enteral nutrition conforms to normal physiological characteristics and has the characteristics of high nitrogen utilization, which can maintain postoperative nitrogen balance, tissue and organ metabolism and functional integrity of intestinal mucosal barrier, promote gastrointestinal function recovery, reduce abdominal distension, and contribute to the prevention and treatment of anastomotic edema and postoperative delayed gastric functional emptying syndrome[16,17].
Relevant reports have pointed out that patients undergoing surgical treatment often have certain gastrointestinal functional problems or metabolic disorders after surgery, and the treatment of digestive tract tumors often leads to gastrointestinal sympathetic nervous system abnormalities, causing intestinal dysfunction and affecting the postoperative recovery process of patients[18]. The occurrence of this condition will lead to changes in patients’ nutritional status, reduced intestinal barrier level, and cause multiple complications. Previous reports have pointed out that surgical treatment is an important factor to aggravate the gastrointestinal dysfunction of patients, and the blood circulation status during gastrointestinal tumor surgery can affect the occurrence of early postoperative gastrointestinal dysfunction of patients[19]. Excessive intraoperative blood loss leads to unstable hemodynamics of blood circulation, and massive blood transfusion and fluid replenishment further lead to disorders of the intravascular coagulation system, affecting the blood supply of the gastrointestinal tract. Operation time makes gastrointestinal congestion time too long, further aggravates gastrointestinal function damage. Relevant research has shown that early enteral nutrition not only has the potential to provide the body with the nutrients it needs; it can also aid in the recovery of gastrointestinal peristalsis function, boost the protective function of the gastrointestinal mucosal barrier, and decrease the occurrence of bacterial flora disorders[20]. To avoid stomach mucosa atrophy and speed up the recovery of gastrointestinal function, enteral nutrition is beneficial. The findings of this research demonstrate that the use of this nursing intervention may shorten the time required for patients in the observation group to regain gastrointestinal functioni.e., to regain intestinal sound, experience their first postoperative exhaust, have their first postoperative defecation and begin receiving their first halffluid feeding after surgery. This is mainly because no drug analgesia is used in ERAS mode intervention, so the inhibition of gastrointestinal peristalsis is less, which is conducive to shortening the time of intestinal peristalsis and anal exhaust. In addition, early enteral nutrition support can promote the repair of intestinal immunity and biological barrier, blood circulation, further accelerate the recovery of gastrointestinal function, reduce complications such as infection, and shorten hospital stay[21].
CONCLUSION
In conclusion, extremely early postoperative enteral nutrition intervention based on the ERAS theory has been shown to improve patients' nutritional status during the recovery period, as well as decrease their level of agitation and enhance the reliability with which they regain gastrointestinal function after endotracheal intubation under general anesthesia in digestive surgery.

Figure 4 Comparison of postoperative nutritional condition observed among the two groups. A: Albumin; B: Hemoglobin; C: Fasting blood glucose.
ARTICLE HIGHLIGHTS
Research objectives
Comparison of nursing effects of different nursing methods, to observe the advantages of very early enteral nutrition based on enhanced recovery after surgery (ERAS) theory over conventional care. The very early enteral nutrition nursing based on ERAS theory showed better improvement in recovery quality, gastrointestinal function, enteral nutrition and immune function in digestive surgery patients with general anesthesia, which confirmed that this nursing method has a good nursing effect. The significance of realizing these objectives for future research is to provide a new reference for perioperative nursing of digestive surgery patients with general anesthesia in the future.
Research methods
Clinical data of patients were retrospectively analyzed and grouped according to nursing methods. Then, independent samplettest, paired samplettest andχ2test were used to statistically analyze the general data of the two groups, related indexes of recovery period, restiness during recovery period, gastrointestinal function recovery, postoperative nutritional status, stress indexes before and after surgery, immune function indexes before and after surgery, anesthesia-related adverse reactions. The characteristic of retrospective study is to explore the cause through the results, and case data is more easily obtained.
Research results
The routine nursing of early postoperative enteral nutrition based on ERAS theory has remarkable effects, with good improvements in wake recovery, wake agitation, gastrointestinal function recovery, postoperative nutritional status, stress, immune function and other aspects, which provides a new nursing method for postoperative nursing of patients with general anesthesia in digestive surgery and needs further prospective exploration.
Research conclusions
Post-stress will affect the length of hospital stay in gastrointestinal surgery patients with general anesthesia, so we should pay attention to the influence of nursing methods on post-operative stress. The effect of early postoperative enteral nutrition nursing based on ERAS theory is better, and the nursing plan with better effect should be preferred in clinic.
Research perspectives
Nursing can improve the physiological indicators of patients, and its influence on the psychological state of patients can be further explored.
FOOTNOTES
Author contributions:Shao YR, Ke X and Xu JD designed the research study; Luo LH, Xu JD and Xu LQ performed the research; Xue JZ, Luo LH and Ke X contributed new reagents and analytic tools; Shao YR and Xu LQ analyzed the data and wrote the manuscript; and all authors have read and approve the final manuscript.
Institutional review board statement:This study was approved by the Ethics Committee of the Guangdong Provincial People’s Hospital.
Informed consent statement:The informed consent statement was waived by the Ethics Committee.
Conflict-of-interest statement:The author declares no competing interests.
Data sharing statement:The labeled dataset used to support the findings of this study are available from the corresponding author upon request.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Li-Qian Xu 0000-0002-3867-8138.
S-Editor:Wang JL
L-Editor:A
P-Editor:Zhao S
 World Journal of Gastrointestinal Surgery2023年9期
World Journal of Gastrointestinal Surgery2023年9期
- World Journal of Gastrointestinal Surgery的其它文章
- Preoperative and postoperative complications as risk factors for delayed gastric emptying following pancreaticoduodenectomy: A single-center retrospective study
- Comparative detection of syndecan-2 methylation in preoperative and postoperative stool DNA in patients with colorectal cancer
- Preoperative prediction of microvascular invasion in hepatocellular carcinoma using ultrasound features including elasticity
- Surgical management of gallstone ileus after one anastomosis gastric bypass: A case report
- Hepatic ischemia-reperfusion syndrome and its effect on the cardiovascular system: The role of treprostinil, a synthetic prostacyclin analog
- Advances and challenges of gastrostomy insertion in children