
Multifactor analysis of the technique in total laparoscopic gastric cancer
2023-10-21 01:05JiaKunShiBoWangXinShengZhangPinLvYunLongChenShuangYiRen
Jia-Kun Shi, Bo Wang, Xin-Sheng Zhang, Pin Lv, Yun-Long Chen, Shuang-Yi Ren
Abstract
Key Words: Esophagogastric anastomotic muscle flap reconstruction technique; Total abdominal radical gastrectomy for gastric cancer; Gastric cancer; Perioperative indicators; Prognosis; Pathological parameters
INTRODUCTION
Gastric cancer is one of the most common tumors of the digestive system worldwide. Although gastric cancer may not have significant manifestations in the early stage, as the disease progresses, systemic symptoms such as emaciation, anemia, and gastric perforation are observed[1]. Surgery is the main treatment strategy for gastric cancer. With recent advances in total laparoscopy, total laparoscopic radical resection has gradually become an important treatment strategy for gastric cancer. Conventional laparoscopic surgery may require at least 5-6 incisions, whereas total laparoscopic surgery requires only 3-4 small incisions, decreasing surgical trauma and postoperative pain[2]. Furthermore, because total laparoscopic surgery is less invasive than conventional laparoscopic surgery, patients can generally return to normal living and working conditions more quickly[3]. Moreover, total laparoscopic surgery does not leave obvious surgical scars; therefore, it is advantageous for patients who pay attention to appearance[4]. Esophagogastrostomy is a method used to repair gastrointestinal anastomosis, called the “double muscle valve”. This technique requires folding the fundus of the stomach, followed by sealing it with two layers of tissue, forming a structure similar to a valve. The application of esophagogastrostomy to total laparoscopic radical resection for gastric cancer can effectively decrease the incidence of complications such as anastomotic incontinence and bile reflux and improve the surgical cure rate and postoperative quality of life, which is a recent topic of interest for surgeons. At present, systematic multivariate analyses of the application effects of esophagogastrostomy in total laparoscopic surgery for gastric cancer and their effects on prognosis remain scarce[5]. In the present study, we conducted surgery and postoperative follow-up of patients with gastric cancer and collected relevant clinical data for esophagogastric anastomosis during postoperative resection for gastric cancer to provide a reference for the clinical improvement of surgical effects, treatment levels, and postoperative rehabilitation efficiency.
MATERIALS AND METHODS
General information
To obtain a definite diagnosis, the study subjects were 60 patients with gastric cancer who were admitted to our hospital from October 2018 to January 2022. The inclusion criteria were as follows: (1) Patients with gastric cancer; (2) Patients whose preoperative pathology was adenocarcinoma; (3) Preoperative computed tomography, ultrasound, and magnetic resonance imaging confirmed tumor presence without distant organ metastasis; (4) Patients who underwent total laparoscopic esophageal plasty; (5) Patients with no history of abdominal surgery; and (6) Patients with complete clinical data. The exclusion criteria were as follows: (1) Tumor involving the dentate line and lower esophageal segment; (2) Patients who did not undergo surgery; (3) Patients who received preoperative radiotherapy, chemotherapy, or targeted therapy; (4) Patients with severe disease and dysfunction; (5) Patients with other or tumor history; (6) Patients with missing follow-up data; and (7) Patients with mental and psychological illnesses.
Surgical procedure
For all patients with intravenous inhalation compound anesthesia, supine position, according to the laparoscopic radical gastric cancer conventional 5-hole placement Trocar, laparoscopic conventional exploration, along the lower edge of the liver ligament, lower separation to the right cardia, cut the right diaphragm, suspension liver, complete lymph node dissection, laparoscopic linear cutter from the esophagus, stomach, specimen in specimen bag, close pneumoperitoneum, all around the umbilical mouth (3.5 cm) specimen, confirm the tumor far and near. The pneumoperitoneum was rebuilt to maintain a pressure of 10-12 mmHg and the “H” shape was labeled at the tip of the remnant stomach, with a width of approximately 2.5 cm and a spacing of 3.5 cm up and down. The plasma muscle layer and middle muscle layer were prepared and incised to prepare the cytoplasmic muscle flap of the anterior gastric wall. Next, the mucosal layer was incised under the H-shaped transverse flap to prepare for subsequent esophageal anastomosis. The posterior wall of the esophagus was pulled 4 cm from the broken end of the esophagus and the plasma muscle layer was continuously stitched on the gastric wall using barbed threads. The broken end and remnant stomach were fixed, the closed section of the esophagus was incised, and the broken end and remnant stomach were anatomized. The whole layer of the posterior wall of the broken end and the mucosal layer and submucosa of the remnant stomach was closed. A barbed thread was used to continuously suture the full layer of the anterior wall of the broken end and the H shape of the remnant stomach. The anterior gastric wall was sutured using a Y-shaped intermittent suture to realize wrapping around the anastomosis. During surgery, a gastroscope was used to check the esophagus and residual gastric anastomosis, including whether the ana-stomosis was intact and whether there was bleeding. After hemostasis of the surgical wound surface, the abdominal cavity was washed with distilled water, and a single drainage tube was placed after the anastomosis of the esophagus and stomach.
Observed indicators
Perioperative index: The perioperative index was observed, and the operating room nurse recorded the operation time, shaping time of esophagogastric double muscle flap anastomosis, number of lymph node dissections, incision length, and intraoperative bleeding volume (calculated using the sterile gauze weighing method). On the other hand, the inpatient nurse recorded postoperative first anal exhaust time, first feeding time, hospitalization time, treatment cost, and the probability of complications during postoperative hospitalization. Information on sex, age, Borrmann classification, histological type, tumor size, tumor-node-metastasis (TNM) stage, vascular invasion, postoperative adjuvant chemoradiotherapy, and lymph node metastasis was collected by inquiring or consulting medical records. Among them, the Borrmann classification can be divided into types I-IV, which refer to mushroom umbrella-type nodules (tumor nodules, polyp shape, ulcer, and ulcer surface can be shallow), local ulcer-type nodules (ulcer degree, edge, and tumor limitation), infiltration ulcer-type nodules (ulcer chassis, unclear edge, and deep infiltration), and diffuse infiltration-type nodules (infiltration of cancer tissue in the stomach wall), respectively. The follow-up records of the patients within 1 year postoperatively were analyzed and patients were grouped based on whether they survived or died. The clinicopathological characteristics of the two patient groups were observed. Statistically significant indicators were included in the Cox regression model, and the relevant factors affecting patient prognosis were analyzed.
Statistical methods
SPSS27.0 was used for data processing, with (n, %), and crossχ2test. Measurement data showing normal distribution are expressed as (mean ± SD), using the independent samplet-test. Relevant factors that affected prognosis were analyzed by Cox regression analysis. Values atP< 0.05 were considered statistically significant.
RESULTS
Perioperative indicators of the patients
The following perioperative indicators were observed: Operation time (318 ± 43 min); time of esophageal anastomosis double muscle valve forming (110 ± 13 min); number of lymph node dissection (26 ± 6); incision length (3.4 ± 0.6 cm); intraoperative bleeding volume (48 ± 15 mL); anal first vent time (5.3 ± 1.8 d); first feeding time (6.0 ± 1.6 d); hospitalization time (11.8 ± 2.5); and treatment cost (5.8 ± 0.7 ten thousand yuan). The specific bar chart ratio is shown in Figure 1. The patients suffered from three postoperative complications, two pulmonary infection-related and one respiratory discomfort-related complication. The number of complications in Figure 2.
Univariate analysis of patients with different prognoses
The univariate analysis showed histological type, tumor size, TNM stage, vascular invasion, and postoperative adjuvant chemoradiotherapy as the main factors affecting the prognosis (P< 0.05). Details are presented in Table 1.
Impact factors affecting patient prognosis
The data were assessed before performing Cox regression analysis. Patient survival was a dependent variable, whereas other statistical differences were independent variables. Details are shown in Table 2. The Cox regression analysis showed that postoperative adjuvant chemoradiotherapy was the main factor affecting the prognosis of patients (P< 0.05). Details are shown in Table 3. The patient survival function plot is shown in Figure 3. The survival time of the subsisting group (10.78 ± 1.52 mo) was significantly higher than that of the death group (7.40 ± 1.51 mo), and the difference was statistically significant (t= 6.444,P< 0.001) (Figure 3).
DISCUSSION
Gastric cancer is a malignant tumor occurring in gastric epithelial tissues. The cause of its occurrence has not been thoroughly studied. However, most scholars believe that factors such as curing, smoking, high salt consumption, high-fat consumption, drinking, and eating stale food increase the risk of gastric cancer (history of benign gastric diseases)[6]. Furthermore, chronic atrophic gastritis, gastric polyps, andHelicobacter pyloriinfection may also increase the probability of gastric cancer occurrence. According to statistics, gastric cancer is one of the most common cancers worldwide; however, its incidence in developed countries has decreased significantly. Conversely, its incidence in Asian countries, such as China, South Korea, and Japan, is still high, which can be attributed to the long-term use of high salt and pickled food[7]. Surgery is a common way to treat gastric cancer. With the development of laparoscopic technology and improvement in medical sciences, the total laparoscopic radical resection of gastric cancer has gradually become the mainstream operation of gastric cancer[8]. Esophagogastric anastomoplasty is a technique in which the esophagus and gastric resection are connected by surgery to restore the gastrointestinal digestive function of patients. Combining it with the total laparoscopic radical resection of gastric cancer can further restore the gastrointestinal function of patients, and such a combination has been applied in treating diseases including esophageal and cardiac cancers[9,10].
The perioperative indicators showed in this study, such as operation time (318 ± 43 min), esophageal anastomosis time (110 ± 13 min), lymph node dissection (26 ± 6), incision length (3.4 ± 0.6 cm), intraoperative bleeding (48 ± 15 mL), anal first discharge time (5.3 ± 1.8 d), first feeding time (6.0 ± 1.6 d), hospitalization time (11.8 ± 2.5), treatment cost (5.8 ± 0.7 thousand yuan), and a poor prognosis ratio of about 16.67%, were consistent with the results of Tianet al[11]. The results of the present study indicate that the double muscle valve plasty of esophagogastric stomosis can indeed be combined with the total laparoscopic radical surgery of gastric cancer to achieve a good curative effect in the near future. Laparoscopic surgery combined with gastric anastomosis double muscle valve plasty can retain the function of the upper stomach and lower esophagus and reduce the effect of surgery on the digestive function of the patient. Furthermore, the double muscle valve structure can avoid gastric content reflux into the esophagus and improve surgical safety. Additionally, autologous tissue repair can avoid the risk of foreign body infection. Simultaneously, as the entire operation was performed using full laparoscopic technology, the operation site was visible, which aided in the accuracy of the operation so as to better protect the nerve and vascular tissues, avoid surgical injury, and improve the efficiency of postoperative rehabilitation to some extent. To summarize, considering patient efficacy, total laparoscopic gastric cancer radical resection with esophagogastric stomosis exhibits remarkable advantages such as high surgical accuracy, high resection rate, low postoperative pain, quick recovery, and digestive function retention.
Statistical data show that the one-year survival rate of patients with gastric cancer treated with radical surgery is about 70%-90%[12]. In the present study, after the one-year follow-up of the 60 patients, their one-year survival rate was 83.33%, consistent with the epidemiological statistics. The univariate analysis showed differences in histological type, tumor size, TNM stage, vascular invasion, and postoperative adjuvant chemoradiation between the surviving and dying patients. This is similar to the conclusion of the Tougeronet al[13]. The histological types of gastric cancer usually include adenocarcinoma, papillary adeno-carcinoma, and mucinous adenocarcinoma, and some differences occur in the prognosis of these different histological types. A study has shown that patients with mucinous adenocarcinoma usually exhibit a higher survival rate compared with patients with the other types[13]. Tumor size is another important factor affecting the prognosis of patients with gastric cancer. Generally, the smaller the tumor, the better the prognosis. Clinically, the tumor size is usually graded according to the diameter, and patients with tumors of 5 cm or less usually exhibit a high survival rate[14]. TNM stage is an important indicator to examine the prognosis of patients with gastric cancer, which can be divided into four stages: Stage I (localized gastric cancer), stage II (locally spread gastric cancer), stage III (lymph node metastasis gastric cancer), and stage IV (distant organ metastasis gastric cancer). Most studies have shown that the higher the grade of the stage, the lower the survival proportion[15]. Vascular invasion is another important indicator associated with the survival rate of patients with gastric cancer, and its survival proportion is usually lower for patients whose tumor has invaded lymphatic or blood vessels[16]. This suggests a possible connection between the histological type, tumor size, TNM stage, vascular invasion, postoperative adjuvant chemoradiotherapy, and prognosis of patients with gastric cancer undergoing esophagogastric anastomosis valvuloplasty combined with total laparoscopic gastrectomy. The Cox regression analysis showed that postoperative adjuvant chemoradiotherapy was the main factor affecting the prognosis of patients, and patients who did not receive postoperative adjuvant chemoradiotherapy had a higher risk of a poor prognosis. The reason may be that postoperative adjuvant chemoradiotherapy removes the residual cancer cells after surgery and reduces the risk of tumor recurrence and metastasis by eliminating the small metastatic focus, thus improving the survival rate of patients[17-19].
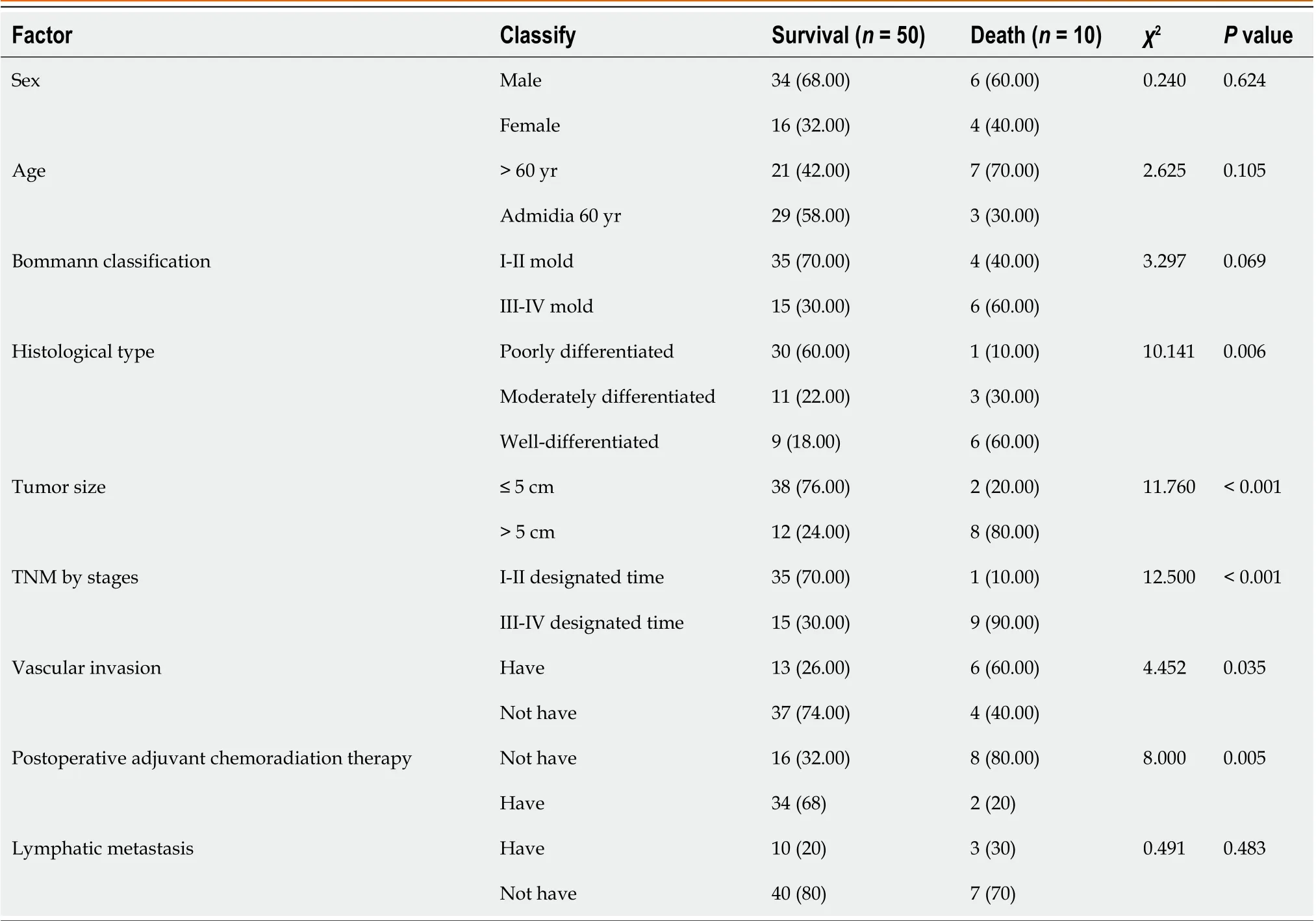
Table 1 Univariate analysis of the patients with different prognoses

Table 2 Assignment of the regression analysis
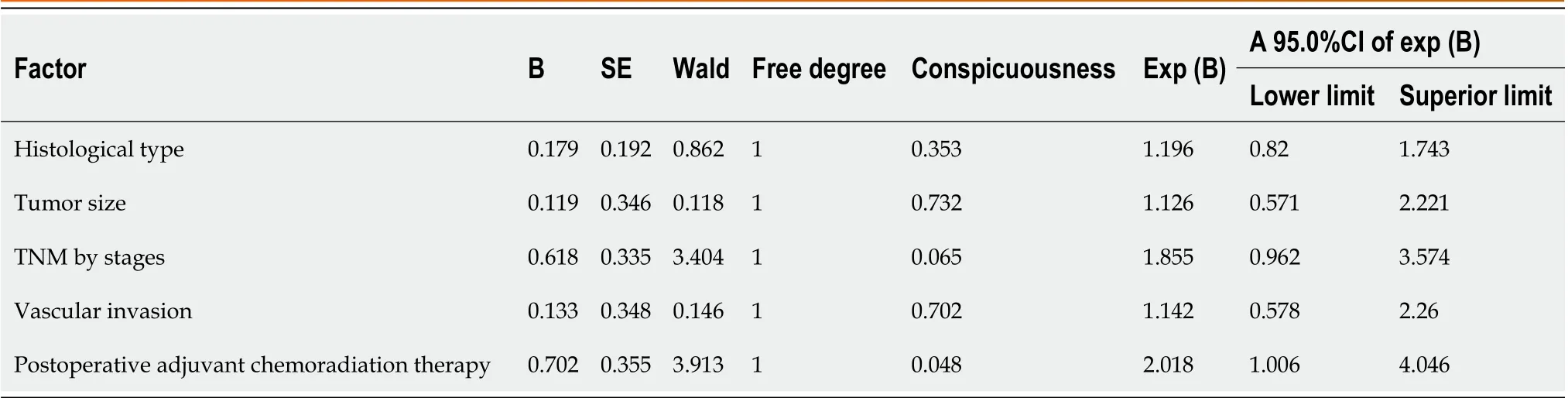
Table 3 Factors influencing the patient outcomes
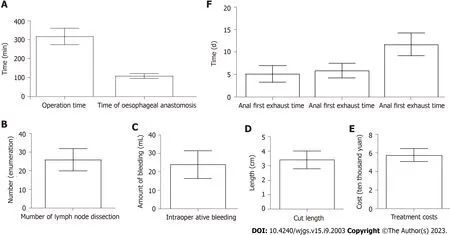
Figure 1 The specific bar chart ratio. A: Bar chart depicting the patient’s operation time and the time of esophageal anastomosis; B-E: Histogram depicting the numbers of lymph node dissection (B), intraoperative blood loss (C), the incision length (D) and the treatment cost (E); F: Bar chartdepicting time of first anal exhaust,time of first food intake and length of hospitalization.
CONCLUSION
In conclusion, esophagogastric-stapled muscle valvuloplasty showed good results in total abdominal gastric cancer. Postoperative adjuvant chemoradiotherapy was the main factor affecting the prognosis of patients. However, the study has the following limitations: The small number of samples, the single source, and the lack of analysis of the long-term efficacy of patients. Thus, large-sample, multi-center, and long-term studies are needed in the future to confirm the present results.
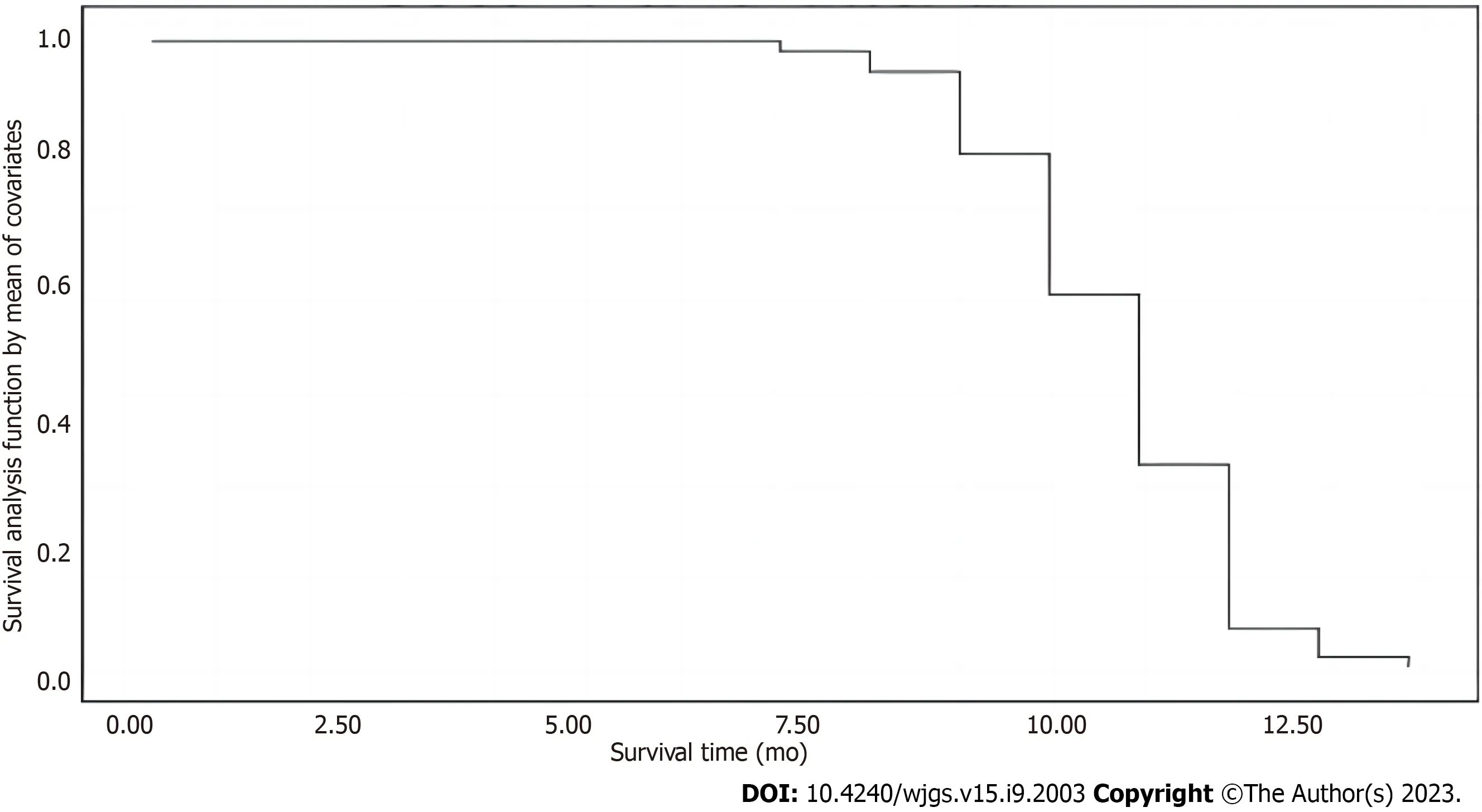
Figure 2 The patient survival function plots.

Figure 3 Bar graph depicting the survival time of patients who survived and died.
ARTICLE HIGHLIGHTS


Research motivation
Gastric cancer is a significant health concern, and total gastrectomy is a common surgical treatment for this condition. However, traditional esophagogastric anastomosis techniques have limitations, leading to complications and suboptimal patient outcomes. The emergence of muscle flap reconstruction technique provides a potential solution to overcome these challenges. By transplanting muscle tissue, the technique improves the stability and blood supply of the anastomosis site, promoting healing and recovery.
Research objectives
The objective of this study was to evaluate the effect of esophagogastrostomy with muscle flap reconstruction technique on the prognosis of patients undergoing total gastrectomy for gastric cancer.
Research methods
This study included 60 patients with gastric cancer who underwent total abdominal gastrectomy with esophagogastric anastomosis using double muscle flap reconstruction technique. Perioperative indicators, such as operation time, formation time of esophageal double muscle flap anastomosis, number of lymph node dissections, incision length, intraoperative bleeding volume, were recorded. Patients were followed up for one year to observe outcomes and classify patients based on different outcomes. Clinicopathological parameters were analyzed to identify factors affecting patient prognosis.
Research results
The study involved 60 patients with gastric cancer who underwent total abdominal gastrectomy with esophagogastric anastomosis using double muscle flap reconstruction technique. The operation time averaged (318 ± 43 min), formation time of esophageal double muscle flap anastomosis was (110 ± 13 min), and other perioperative indicators were measured. Three postoperative complications were recorded: 2 cases of pulmonary infection and 1 case of respiratory discomfort. During the one-year follow-up, 50 patients survived while 10 died. Univariate analysis identified histological types, tumor size, tumor-node-metastasis staging, vascular invasion, and postoperative adjuvant radiotherapy and chemotherapy as the main factors affecting prognosis in surviving patients. Cox regression analysis confirmed the significance of postoperative adjuvant therapy on patient prognosis. The survival time of the survival group was significantly higher than that of the death group (P< 0.05).
Research conclusions
The study concludes that esophagogastric anastomosis with muscle flap reconstruction is effective for patients undergoing total abdominal gastrectomy for gastric cancer. The technique improves the stability of the anastomosis site and enhances blood supply, promoting healing and recovery. Esophagogastric anastomosis with muscle flap reconstruction technique shows positive outcomes in patients undergoing total abdominal gastrectomy for gastric cancer, and postoperative adjuvant therapy plays a vital role in improving patient prognosis.
Research perspectives
Future research can focus on optimizing the muscle flap reconstruction technique to further enhance surgical outcomes and minimize complications. Additionally, investigating the long-term effects of postoperative adjuvant radiotherapy and chemotherapy on patient prognosis would provide valuable insights. Furthermore, evaluating the cost-effectiveness of this technique and comparing it with other surgical methods will help guide decision-making in clinical practice.
ACKNOWLEDGEMENTS
I would like to express my sincere thanks to all those who participated in the manuscript.
FOOTNOTES
Author contributions:Shi JK and Wang B proposed the concepts for this study; Zhang XS and Lv P collected the data; Shi JK, Chen LY, and Ren SY contributed to formal analysis; Ren SY and Shi JK contributed to the investigation; Shi JK, Chen LY, and Ren SY contributed to the methodology; Wang B supervised the research; Shi JK validated this study; Shi JK and Ren SY contributed to the visualization of research; Shi JK, Wang B, Zhang XS, Lv P, Chen LY, and Ren SY reviewed and edited the manuscript.
Institutional review board statement:The study was reviewed and approved by the institutional review board of Dalian Friendship Hospital.
Informed consent statement:This study has obtained informed consent from patients.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Jia-Kun Shi 0009-0001-5943-5055; Xin-Sheng Zhang 0000-0002-1915-3205; Shuang-Yi Ren 0009-0000-7056-2963.
S-Editor:Wang JJ
L-Editor:A
P-Editor:Wang JJ
 World Journal of Gastrointestinal Surgery2023年9期
World Journal of Gastrointestinal Surgery2023年9期
- World Journal of Gastrointestinal Surgery的其它文章
- Preoperative and postoperative complications as risk factors for delayed gastric emptying following pancreaticoduodenectomy: A single-center retrospective study
- Comparative detection of syndecan-2 methylation in preoperative and postoperative stool DNA in patients with colorectal cancer
- Preoperative prediction of microvascular invasion in hepatocellular carcinoma using ultrasound features including elasticity
- Surgical management of gallstone ileus after one anastomosis gastric bypass: A case report
- Hepatic ischemia-reperfusion syndrome and its effect on the cardiovascular system: The role of treprostinil, a synthetic prostacyclin analog
- Advances and challenges of gastrostomy insertion in children