
Immediate Surgical Intervention for Penile Fracture:a Case Report and Literature Review
2011-11-22 02:36:04JinWenHanzhongLiZhigangJiandHongjunLi
Chinese Medical Sciences Journal 2011年2期
Jin Wen,Han-zhong Li*,Zhi-gang Ji,and Hong-jun Li
Department of Urology,Peking Union Medical College Hospital,Chinese Academy of Medical Sciences &Peking Union Medical College,Beijing 100730,China
PENILE fracture is a critical urological emergency,which is caused by the rupture of the tunica albuginea of the corpus cavernosum following blunt trauma to the erect penis.Traumatic injuries of the penis often occur in the erected state.1Due to the possible embarrassment,this condition has been underreported.Typically,the patient reports a snap or cracking sound accompanied by sharp pain and rapid penile detumescence,followed by immediate development of swelling and angulation.2The common causes include direct injuries,forceful masturbation,or vigorous sexual intercourse.3Most injuries to the penis need immediate surgical treatment.Here we report a case of penile fracture caused by traumatic injury.
CASE DESCRIPTION
A 37-year-old man was presented to the Emergency Room of Peking Union Medical College Hospital with acute painful swelling of the penis for 9 hours.The patient reported that he was having sexual intercourse with his girlfriend with the superior position when his penis inadvertently slipped from the vagina and was forcefully thrust against his partner’s perineum,but he declined to reveal more detail about the occurrence of the injury.Upon injury,he experienced a sharp pain.The erect penis immediately became flaccid and a hematoma formed.The penis began to swell and marked bruises developed along the shaft within about five minutes.Fortunately,urination was not impeded and urine was normal.
The patient’s height was 1.63 m,body weight 65 kg,and blood pressure 120/75 mmHg.Physical examination found the penis swollen and ecchymotic.A careful palpation located a gap in the penile shaft underneath the overlying clot.There was severe tenderness at the left side of the penis and the shaft was deviated rightward and upward (Fig.1).The bladder was impalpable.Urine analysis was performed to rule out microscopic hematuria.Ultrasonography showed penile fracture at the left shaft of the penis.
We performed urgent surgical exploration under continuous epidural anesthesia based on the clinical diagnosis.A subcoronal hemi-circumferential incision was made.Buck’s fascia was exposed over the area showing maximal hematoma,through which a 1.5-cm tear was revealed in the tunica albuginea enveloping the left corpus cavernosum.There was no tear in the right corpus cavernosum and corpus spongiosum.Following debridement,the corporal lacerations were repaired with 4/0 absorbable sutures after placing a 16 F silicone Foley’s catheter.An artificial erection demonstrated no penile deviation.The fascial and wound edges were reopposed.The patient made an uneventful recovery and the urethral catheter was removed after 72 hours.The patient reported good erections and normal erectile function.No penile deviation was reported,with a normal urinary stream 6 weeks after the surgery (Fig.2).
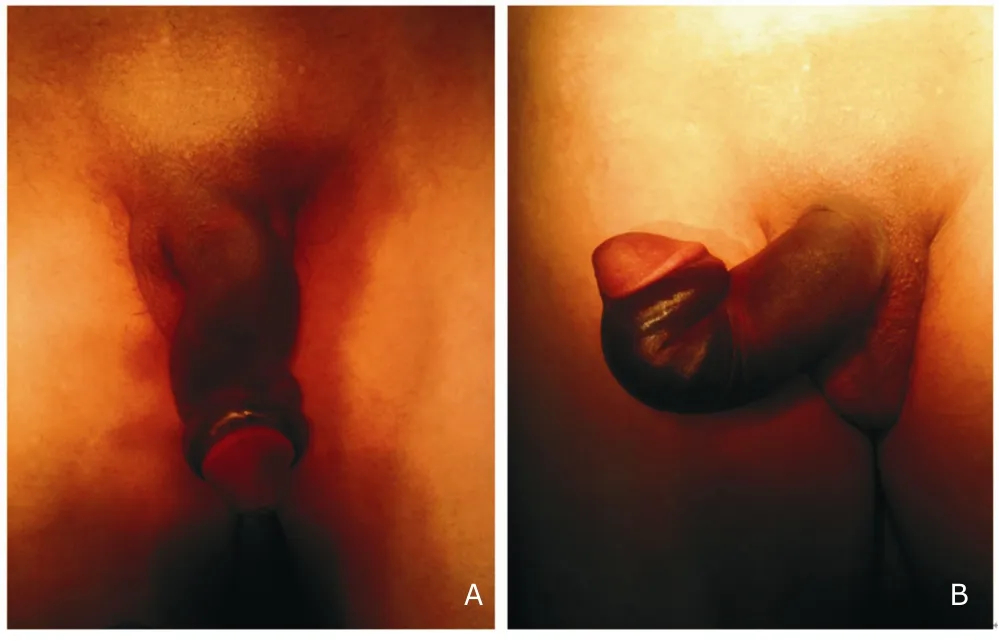
Figure 1.The shaft of the fractured penis was deviated rightward (A) and upward (B).
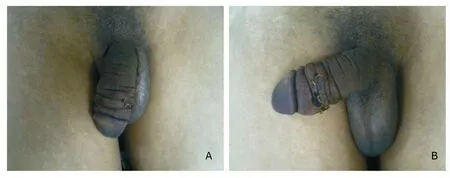
Figure 2.The rightward deviation (A) and upward deviation (B) were corrected by immediate surgical repair.
DISCUSSION
Penile fracture generally occurs during an erection as a result of direct blunt trauma that bends the erect penis in an unphysiological manner.The diagnoses of penile fracture are usually fairly straightforward because of their clinical presentation.1It has been reported that its annual incidence is 0.29 to 1.36 per 100 000.2The right side is more often involved than the left with an incidence as high as 75% in all the penile fracture cases.3Bilateral injuries are reported in 4-10% of the cases.4Concomitant tearing of the corpus spongiosum and urethra may occur.The patient typically reports hearing a“pop”or cracking sound at the time of the injury,followed by pain and immediate detumescence.5The penis may take on a bizarre shape,with deviation of the penile shaft,usually opposite to the tear site secondary to the mass effect of the hematoma.“Rolling sign”may be illustrated if Buck’s fascia is intact,in which the clot within the torn tunica overlying the fracture site can be palpated as a discrete tender swelling over which the skin can be gently rolled.When Buck’s fascia is violated,the blood extravasates around Colles’ fascia,forming ecchymosis in the perineum,scrotum,and lower abdominal wall.The presence of bloodstained urethral meatus,gross hematuria,or inability to urinate should alert doctors to the possibility of concomitant urethral injury,but their absence does not exclude such an injury because the blood may leak out of the urethra.6
In most cases,the diagnosis can be made clinically with no need of any diagnostic tools.When the history or physical examination findings are equivocal,further testing may be warranted.Urine analysis is required to rule out microscopic hematuria,which can be indicative of an inapparent urethral injury.Other available imaging modalities can be helpful,but should not replace clinical assessment and delay exploration in the urgent setting.Ultrasonography can identify large disruptions of the tunica albuginea and hematomas with a detection rate of 86%,6but this imaging modality is dependent on the proficiency of the operator and lacks tissue contrast.Magnetic resonance imaging has been proposed to be the most accurate method for evaluating patients with acute penile trauma,but the application of this technique is restricted by its high cost and limited availability.Angiography is not recommended in the case of acute penile fracture.7
Until the early 1980s,the management of fractured penis had been highly controversial.Many conservative treatments have been employed,such as pressure dressing,cold compress,Foley catheterization,anti-inflammatory drugs,antibiotics,antiandrogens,or sedatives.The drawbacks of conservative treatments include expanded pulsatile hematoma,infected hematoma,abscess formation,severe penile angulation,arteriovenous fistulas,and impotence.6In comparison,conservative treatment may be substantially more invasive than surgical treatment.
Immediate surgical repair is now the standard care with fewer complications,shorter hospital stays,better outcome,and increased patient satisfaction compared with other therapies.It can avoid infections from short-term as well as long-term complications such as urethral stricture.Management of associated urethral injuries has been variable in the literature.In cases of total rupture,anastomosis should be performed with a suprapubic cystostomy.Long-term complications following penile fracture repair may be painful erection,painful intercourse,skin necrosis,sensory loss,penile deviation,urethral stricture,and priapism.8
There are also“false”penile fractures,which are usually characterized by gradual detumescence and absence of the cracking sound typically in penile fractures.Rupture of the dorsal vein or dorsal artery is the most commonly reported cause,and the consequent condition is indistinguishable from true corporal fracture except by cavernosography.Ruptured dorsal vein should be ligated when encountered during operation but can also be managed conservatively if diagnosed clinically.9
We recommend urethral catheterization after anesthetization.The Foley’s catheter facilitates orientation of the penis during surgery.It also allows identification of the urethra and thus prevents inadvertent injury while dissecting the corpus cavernosum,as well as allowing the repair of any associated urethral injury.Nevertheless,catheterization should be cautiously assessed to reduce the risk of infection and further trauma to the urethra.8We made a hemi-circumferential subcoronal incision to locate and repair the fracture in the present case.It allows an evaluation of all three cavernous bodies and repair of injuries along the course of the shaft.We made the closure transversely across the shaft to avoid narrowing of penis or uretha.After surgical repair,intracavernous saline injection and simulated erection were applied to localize inapparent tunica albuginae laceration.
In conclusion,penile fracture could be clinically diagnosed based on reported history and physical examination.One or both sides of the corpus cavernosa may be involved,possibly with concomitant injury to the penile urethra.Appropriate imaging might be necessary if urethral injury is suspected.Prompt surgical exploration and repair is advocated for its high efficiency in treating this emergency.
1.Ghanem AN.Penile fracture in Kermanshah,Iran:the long-term results of surgical treatment.BJU Int 2003;91:301-2.
2.Chung CH,Szeto YK,Lai KK.“Fracture”of the penis:a case series.Hong Kong Med J 2006;12:197-200.
3.Jack GS,Garraway I,Reznichek R,et al.Current treatment options for penile fractures.Rev Urol 2004;6:114-20.
4.Koifman L,Cavalcanti AG,Manes CH,et al.Penile fracture–experience in 56 cases.Int Braz J Urol 2003;29:35-9.
5.Derouiche A,Belhaj K,Hentati H,et al.Management of penile fractures complicated by urethral rupture.Int J Impot Res 2008;20:111-4.
6.Masarani M,Dinneen M.Penile fracture:diagnosis and management.Trends Urol Gynaecol Sex Health 2007;12:20-4.
7.Eke N.Fracture of the penis.Br J Surg 2002;89:555-65.
8.Muentener M,Suter S,Hauri D,et al.Long-term experience with surgical and conservative treatment of penile fracture.J Urol 2004;172:576-9.
9.Feki W,Derouiche A,Belhaj K,et al.False penile fracture:report of 16 cases.Int J Impot Res 2007;19:471-3.
 Chinese Medical Sciences Journal2011年2期
Chinese Medical Sciences Journal2011年2期
- Chinese Medical Sciences Journal的其它文章
- Risk Factors Analysis on Traumatic Brain Injury Prognosis
- Erythropoietin Receptor Positive Circulating Progenitor Cells and Endothelial Progenitor Cells in Patients with Different Stages of Diabetic Retinopathy△
- Inhibition of SIRT1 Increases EZH2 Protein Level and Enhances the Repression of EZH2 on Target Gene Expression△
- Clinical Treatment and Anatomy Study of Maxillary First Molars with Five Root Canals
- Magnetic Resonance Urography and X-ray Urography Findings of Congenital Megaureter
- Changes of Nerve Growth Factor in Amniotic Fluid and Correlation with Ventriculomegaly△