
A study on service capacity of primary medical and health institutions for cervical cancer screening in urban and rural areas in China
2019-11-08 01:49:50YangLiLiMaChunxiaYangZhangyaChenYuqianZhaoLeDangJingheLangYoulinQiao
Yang Li ,Li Ma ,Chunxia Yang,Zhangya Chen,Yuqian Zhao,Le Dang,Jinghe Lang,Youlin Qiao
1Department of Epidemiology,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;2Division of Health Information Dissemination,Institute of Medical Information,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100005,China;3Department of Epidemiology,Dalian Medical University,Dalian 116027,China;4Department of Epidemiology and Biostatistics,West China School of Public Health and West fourth Hospital,Sichuan University,Chengdu 610041,China;5Executive office,Taiyuan Health Supervision,Taiyuan 030001,China;6Office of Cancer Prevention and Treatment,Sichuan Cancer Hospital &Institute,Sichuan Cancer Center,School of Medicine,University of Electronic Science &Technology of China,Chengdu 610041,China;7Department of Obstetrics and Gynecology,Peking Union Medical College Hospital,Chinese Academy of Medical Sciences/Peking Union Medical College(CAMS/PUMC),Beijing 100730,China
Abstract Objective:To provide a decision-making basis for sustainable and effective development of cervical cancer screening.Methods:This cross-sectional study assesses the service capacity to conduct cervical cancer screening with a sample of 310 medical staff,medical institutions and affiliated township health centers from 20 countylevel/district-level areas in 14 Chinese provinces in 2016.Results:The county-level/district-level institutions were the main prescreening institutions for cervical cancer screening.More medical staff have become engaged in screening,with a significantly higher amounts in urban than in rural areas(P<0.05).The number of human papillomavirus(HPV)testers grew the fastest(by 225% in urban and 125% in rural areas)over the course of the project.HPV testing took less time than cytology to complete the same number of screening tasks in both urban and rural areas.The proportion of mid-level professionals was the highest among the medical staff,40.0% in urban and 44.7% in rural areas(P=0.406),and most medical staff had a Bachelor’s degree,accounting for 76.3% in urban and 52.0% in rural areas(P<0.001).In urban areas,75.0% were qualified medical staff,compared with 68.0% in rural areas,among which the lowest proportion was observed for rural cytology inspectors(22.7%).The medical equipment for cervical pathology diagnosis in urban areas was better(P<0.001).HPV testing equipment was relatively adequate(typing test equipment was 70% in urban areas,and non-typing testing equipment was 70% in rural areas).Conclusions:The service capacity of cervical cancer screening is insufficient for the health needs of the Chinese population.HPV testing might be an optimal choice to fill the needs of cervical cancer screening given current Chinese medical health service capacity.
Keywords:China;cervical cancer screening;health service capacity;appropriate technology;cytology testing;HPV testing
Introduction
Cervical cancer is a common cancer that seriously threatens the health of females worldwide.In 2018,there were approximately 570,000 new cases and 311,000 death cases from cervical cancer worldwide(1).The majority of new cases and deaths occurred in low-and middle-income countries,which accounted for 86% and 88% of the new cases and deaths in the entire world,respectively(1).In the last 20 years,the incidence and mortality of cervical cancer have been continuously increasing in China(2).In 2015,there were 98,900 new cases and 30,500 deaths of cervical cancer in China(3).From 2000 to 2014,the average annual percent change(AAPC)of age-standardized incidence rates in China was at 9.2%,and the AAPC in rural areas was relatively high(4).Females living in the Northwest China and Central China have a high risk of mortality from cervical cancer compared to the nationwide,with the rate ratio being 2.09[95% confidence interval(95% CI):1.83-2.38]and 1.26(95% CI:1.11-1.44)respectively(5).In the last 30 years,the disease burdens of cervical cancer in developed countries have been dramatically decreased through the introduction of well-planned population-based cervical cancer screening programs and preventive vaccination programs against human papillomavirus(HPV)(6,7).In May 2018,Dr.Tedros Adhanom,director-general of the World Health Organization(WHO),proposed an intermediate target to eliminate cervical cancer by 2030(8).As the largest developing country with a great disease burden of cervical cancer,China plays an important role in achieving the global elimination goal.In the last 10 years,the Chinese government has conducted a series of substantial work in cervical cancer prevention and control.In 2009,China launched a new round of medical system reforms and proposed the implementation of major national public health service projects(9).As a part of this health care reform,China’s government launched a major public health service project,namely,the National Cervical Cancer Screening Program(NCCSP)(10),which has played an important role in preventing cervical cancer and ensuring women’s health in China(11).
The WHO noted that the service capacity of medical institutions,including human resources,equipment resources and personnel capacity,has a great impact on the national prevention and control of cervical cancer;it is also an important factor to measure the sustainability of cervical cancer prevention and control policies and strategies in a country(12).At present,the main barrier of cervical cancer prevention in some countries is a lack of capacity to screen or treat cervical cancer in medical institutions.China is also faced with practical issues such as a large population base,low overall coverage rate,lack of professional personnel and training,unbalanced health service development in different economic regions and other practical problems(11).The Lancet once commented that the success of the NCCSP still requires long-term observation and scientific assessment(13).Therefore,understanding the medical and health service capacity of cervical cancer screening,including the progress of screening work,personnel service capacity,implementation conditions of the equipment,etc.,would be informative for strengthening the future implementation of cervical cancer screening in China.This study investigates the service capacity of medical and health institutions on the cervical cancer screening project developed by Peking Union Medical College Hospital and the Cancer Hospital Chinese Academy of Medical Sciences that collaborated with 21 Grade A medical institutions and universities while evaluating the real-world effectiveness of different screening techniques in large populations.Accordingly,this study aims to provide a decision-making basis for the sustainable and effective development of cervical cancer screening in China.
Materials and methods
Respondents
With a convenience sampling method,340 township health centers and 20 primary medical institutions in 20 counties or districts that conducted the NCCSP were selected from 14 provinces(Table 1),and 310 medical staff who participated in cervical cancer screening were investigated.All investigated institutions were public medical institutions.
Survey methods
Questionnaires were used to collect relevant data in this survey,which were conducted from July to October 2016.The questionnaires included items on the 1)workload,equipment and infrastructure of cervical cancer screening in medical institutions;2)implementation and management of cervical cancer screening project;and 3)background information of medical staff who participated in cervical cancer screening.The questionnaires concerning 1)and 2)were completed by managers in charge of cervical cancer screening projects in primary medical institutions,and the questionnaires regarding 3)were completed by medical staff.
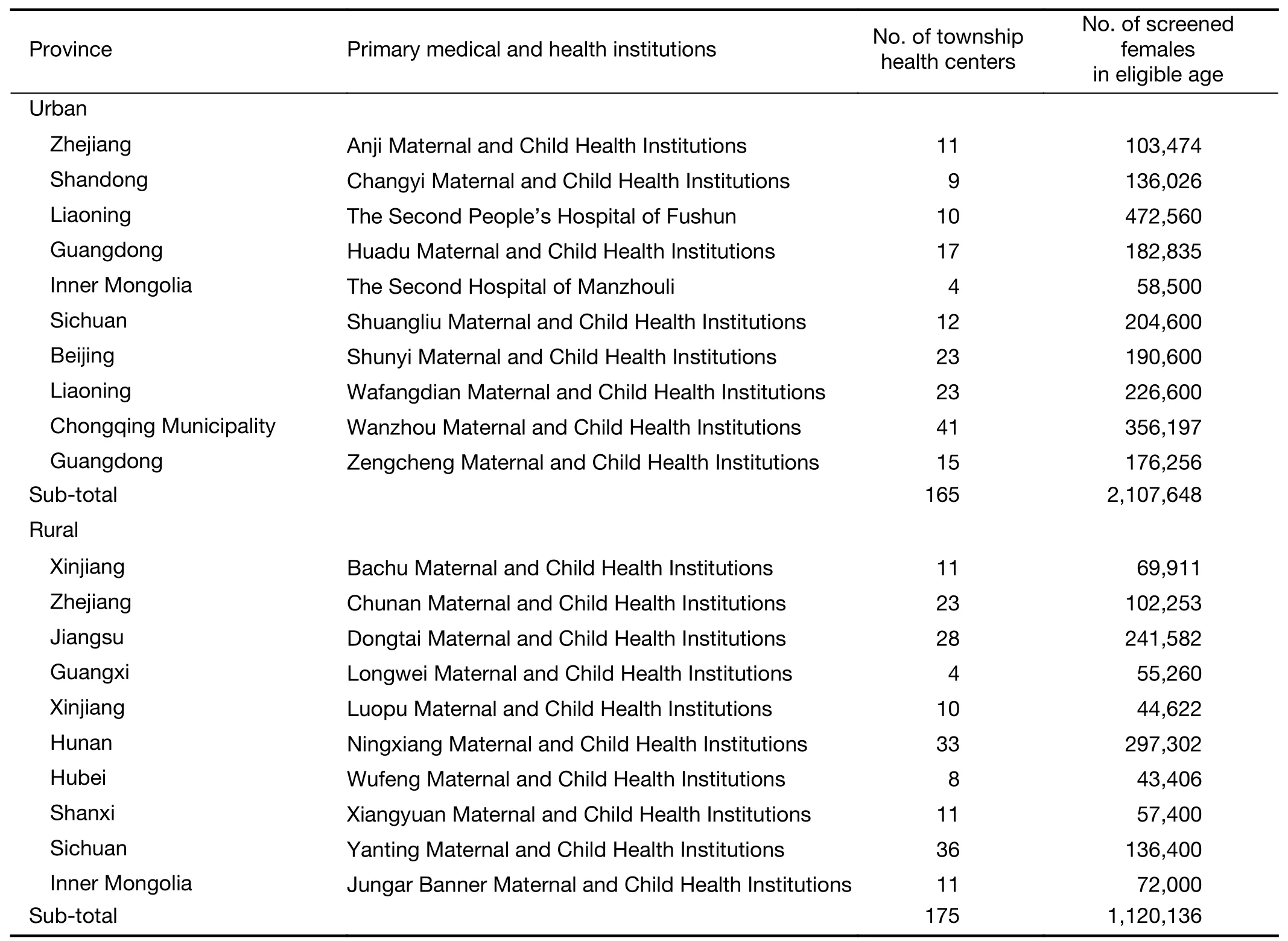
Table 1 Study sites involved NCCSP
Quality control
First,a unified proposal,questionnaire and instruction manual were designed.Second,before the formal survey began,two institutions within the scope of this survey were selected to conduct a pre-survey,and then,the questionnaire was updated according to the results of the pre-survey.Third,detailed instructions for the questionnaire were prepared,and standardized training was provided to the investigators.
Statistical analysis
EpiData3.1(EpiData Association;Odense,Denmark)was used for data entry by two researchers,and SPSS 17.0(SPSS Inc.,Chicago;IL,USA)was applied for the statistical analysis.Chi-square test was applied to compare the task and division of labor,the service capacity of medical staff,and the proportion of examination equipment and examination rooms/laboratories of medical institutions between rural and urban areas.Fisher’s exact test was applied when small sample size,i.e.less than 40,and significance level was set to 0.05.
Results
Assignment and cooperation among medical institutions participating in cervical cancer screening programs
Completion of cervical cancer screening tasks in medical institutions
An analysis showed that the county/district-level medical institutions that were the main implementer of NCCSP in urban and rural areas provided nearly all cervical cancer screening services.The results showed that the number of institutions for HPV testing with genotyping is higher in urban areas(P=0.003).All institutions could offer gynecological examinations and colposcopy examinations.Overall,90.0%,80.0%,and 50.0% of institutions in urban areas could offer HPV testing,pathology diagnosis and liquid-based/thin prep cytologic tests(TCTs),respectively;in rural areas,the proportions decreased to 70.0%,40.0%and 20.0%,respectively(Table 2).
The main roles of township-level hospitals were organizing and mobilizing females and following up on abnormal/suspicious cases;some of these township-level hospitals that have gynecology departments also undertook tasks of gynecological sample collection and visual inspection of acetic acid or lugol’s iodine(VIA/VILI).
Service capacity of medical staff
Number and growth of medical staff engaged in cervical cancer screening programs
In the 20 county-level/district-level medical institutions,35.3%(310/878)of the employed medical staff members in gynecology,laboratory,pathology and other departments related to cervical cancer screening were involved in the NCCSP program.The analysis results performed by the 310 medical staff showed that the proportion of staff who engaged in pathology diagnosis in urban areas was statistically significantly higher than that in rural areas(P=0.003).The proportion of staff engaging in a colposcopy examination was significantly lower in urban areas(P=0.002)(Table 3).
The increasing rate of the number of medical staff involved in the NCCSP was higher in urban areas than in rural areas during the course of the project(P=0.018).The growth was especially rapid for personnel working in HPV testing in both rural and urban areas.The growingproportion of medical staff for gynecological examinations and cytology testing was significantly higher in urban areas than in rural areas(P=0.015,P=0.022)(Table 4).
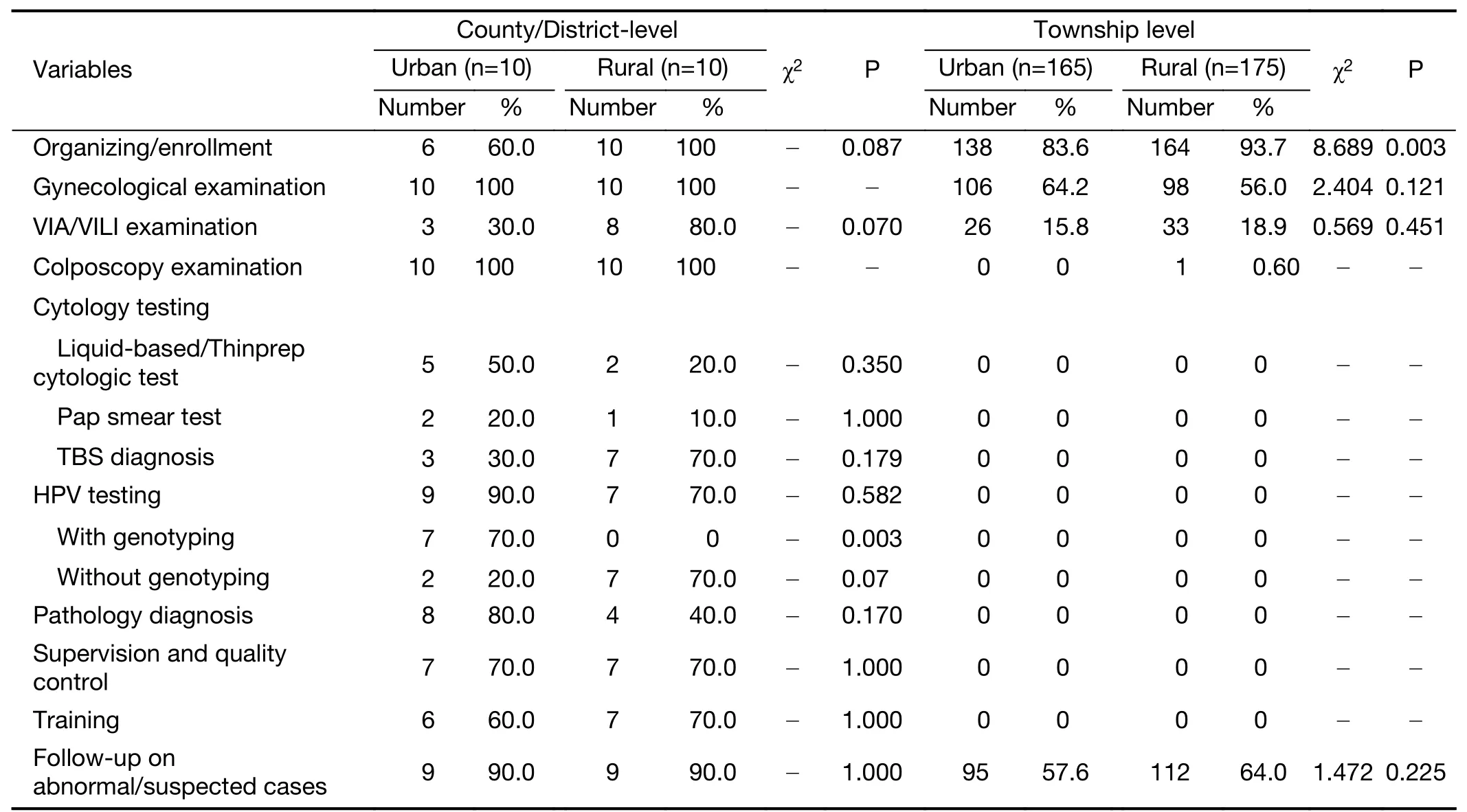
Table 2 Characteristics of screening services provided in NCCSP by level of medical institutions
The number of medical staff per 10,000 people in areas where the project was conducted was estimated by the number of medical staff engaged in cervical cancer screenings.According to the daily workload standard of cervical cancer screenings,we also estimated the working hours of completing the screening of age-appropriate females in the area.The results are shown inTable 5.We can observe that in urban and rural areas,the number of staff who provided cytology testing(0.10 person/10,000 and 0.20 person/10,000,respectively)and HPV testing(0.06 person/10,000 and 0.08 person/10,000,respectively)per 10,000 age-appropriate females was the least,and they worked the longest days,which were 1,003.64 d and 509.15 d in cytology testing,and 574.91 d and 460.96 d in HPV testing in urban and rural areas,respectively.The time taken by HPV detection is less than that taken by cytological examination in completing the same number of screening tasks.
Ability of medical staff involved in cervical cancer screening
Both urban and rural personnel had mainly mid-level and senior professional titles.The personnel with mid-level professional titles accounted for the highest proportion,specifically,40.0% and 44.7% in urban and rural areas,respectively(P=0.406).A Bachelor’s degree was the main educational background,which accounted for 76.3% of urban medical workers and 52.0% of rural medical workers(P<0.001).The vast majority of medical personnel who participated in the NCCSP were qualified as physicians(Table 6).
The ability requirements of medical staff for cervical cancer screening are outlined in the guidelines of quality assurance and control of cervical cancer screening in China(14).The service capacity of medical personnel was assessed based on the ability requirements(Table 7).The number of medical staff who met the NCCSP requirements is shown inTable 8.The results displayed the qualified staff as cytological examiners are insufficient in rural areas,only 22.7%.
Facility and equipment/lab status
As shown inTable 9,all institutions were equipped with digital colposcopy.The proportion of medical institutions equipped with HPV testing instruments was also higherand accounted for 90.0% and 70% in urban and rural areas,respectively.Fifty percent of urban institutions have TCT production machines,and only 20% of rural institutions have these machines,but there is no statistical difference.The proportion of pathological image analyzers,dehydrators,embedding machines and slicers related to pathological examination was significantly higher in urban medical institutions than in rural institutions,which was statistically significant.

Table 3 Number of medical staff involved in NCCSP
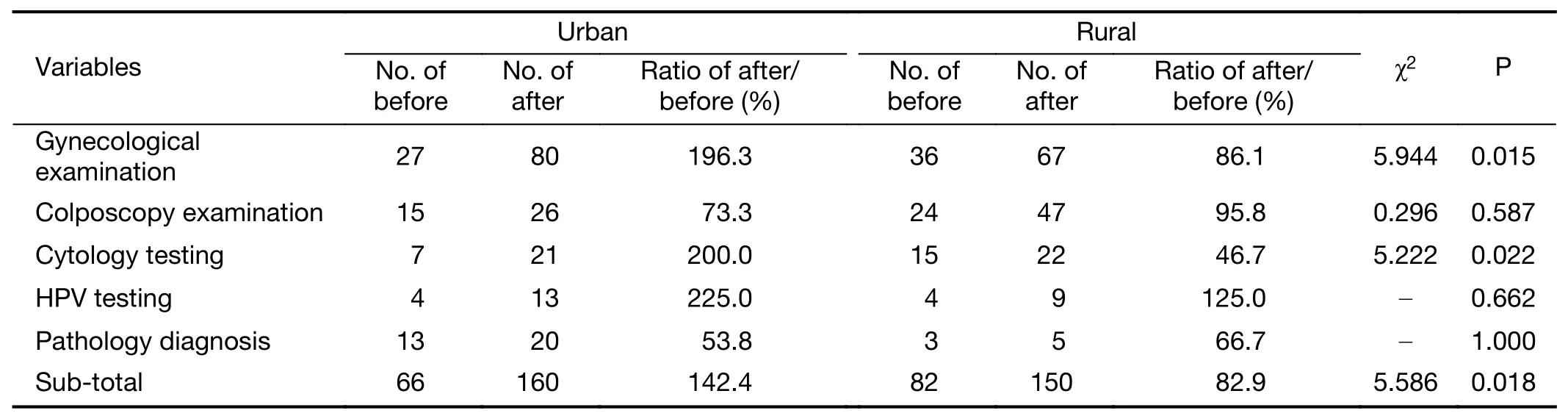
Table 4 Increasing number of medical staff involved in NCCSP before and after implementation
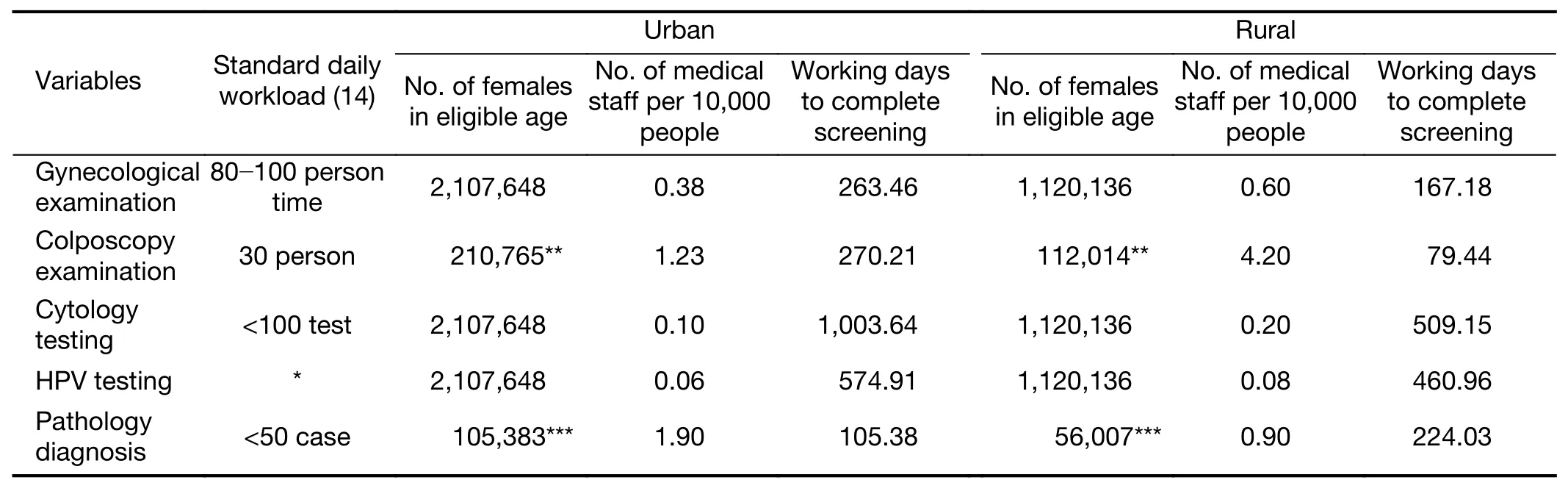
Table 5 Working time needed to complete required screening estimated according to national standard daily workload
The examination rooms/laboratories are shown inTable 10.Both urban and rural medical institutions had independent gynecological examination rooms,and only two urban medical institutions had polymerase chain reaction(PCR)laboratories,which are necessary to perform the HPV typing test.
Discussion
A good multi-sectoral collaboration mechanism has been formed and service capacity of medical institutions has been promoted during progress of NCCSP
As can be seen from the results of this survey,a screening model from the central to the local levels has gradually been established for the screening project in urban and rural areas.This screening model has a modality of multiinstitution cooperation of county-level/district-level medical institutions as the main providers of screening services and comprehensive hospitals at the county level and third-party inspection institutions that work as collaborators.Different collaborations and administration mechanisms that ensure the implementation of NCCSP were established based on the availability of medical resources in these areas.
With the implementation of the program,the number of medical staff members in primary medical institutions has continued to increase,with a particularly significant growth in the number of personnel who work in HPV testing,and most of medical staff possess a good professional foundation and professional quality.With respect to medical training,the mean number of trainings each person received was more than one,and the training rate reached 100% which promotes the improvement of the professional ability of medical staff.In terms of facilities and equipments,medical institutions in urban areas can provide better cervical cancer screening equipments in general than the institutions in rural areas.With the introduction of HPV testing in recent years,medical institutions in pilot areas have also equipped with relevant equipments,and so the equipment is relatively sufficient.
Current health service capacity is unable to completely satisfy demand of cervical cancer screening of China
First,the overall medical service capacity of township health centers is insufficient.Only few institutions can provide gynecological sampling and VIA/VILI examinations,and colposcopy,cytology and pathology diagnosis cannot be performed.
Second,there is a gap between the screening needs and the number of medical staff.Since the screening project started in China,the program has covered less than 30% of the population in China as calculated based on the population data;there are 295 million 35-64-year-old females in China according to the sixth national population census of the National Bureau of Statistics in 2010(15).The results of our survey indicate that medical workers spent at least 1,003 d in urban areas and 509 d in rural areas to complete the screening task,which took the longest screening time as of the time completing the project.Only 1.16% of Chinese females were surveyed.If this coverage rate remains unchanged,some Chinese females would never be able to receive even one screening service during their entire lives.
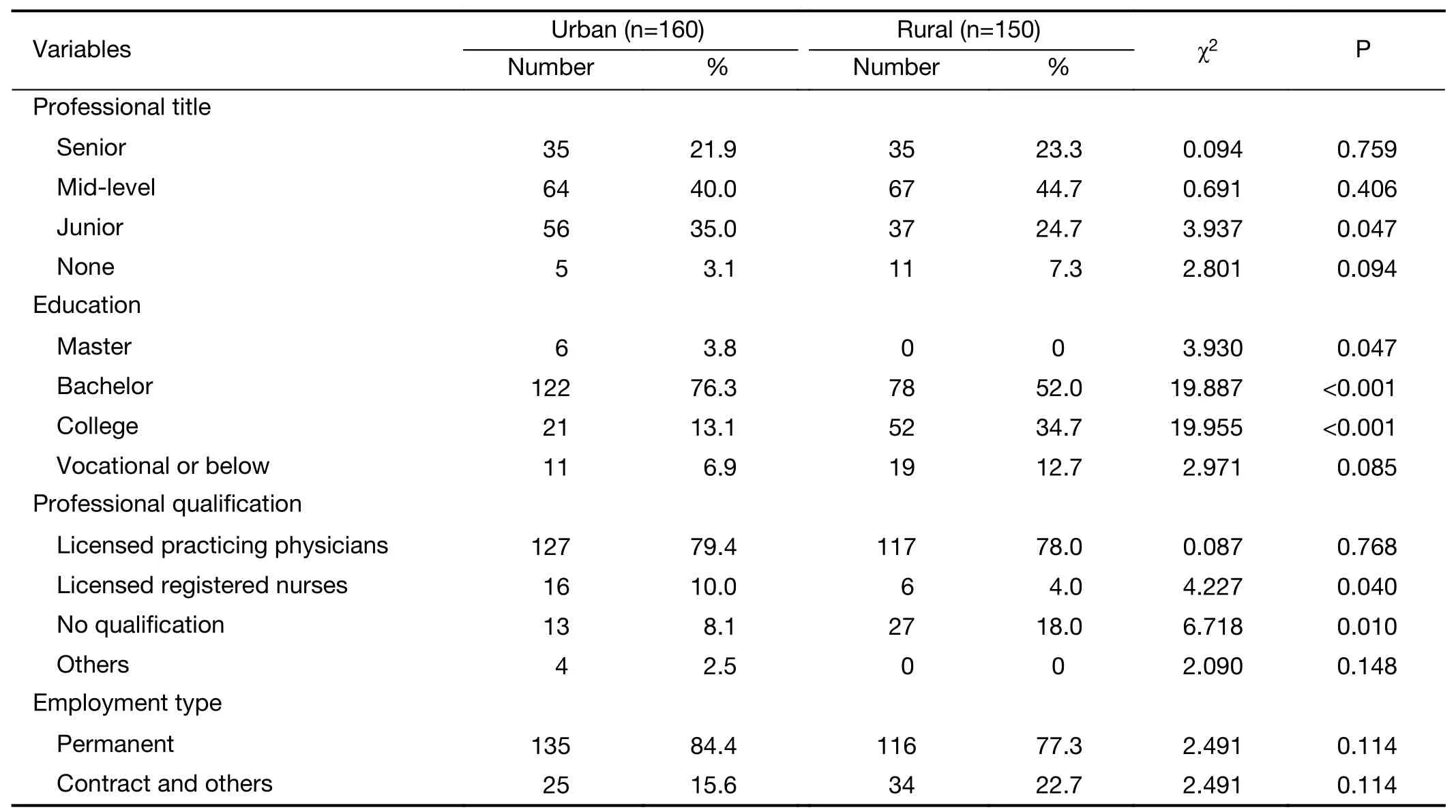
Table 6 Information of medical staff engaged in NCCSP
Third,the growth of the medical staff working in pathology was slower,and the growth of examiners conducting cytology testing was also slower in rural areas.The training of medical personnel in these two examinations was difficult and needed so much time that it was impossible to quickly replenish relevant personnel in a short time.In addition,a certain proportion of personnel were still not officially part of the staff who are responsible for conducting the screening.It is difficult to conduct a complete and systematic cultivation of such personnel because of mobility.
Fourth,the construction of PCR laboratories required by the typing HPV detection is insufficient,which affected the detection effect of typing HPV detection to some extent.
Finally,a relatively large gap still exists in the current health service capacity between urban and rural areas.Urban areas are slightly better than rural areas in terms of medical staff and facilities.
Appropriate cervical cancer screening technologies should be selected according to population demand and medical capacity of urban and rural areas in China
In China,primary screening institutions still have common problems for cervical cancer screening,such as insufficient medical human resources and poor professional quality,which are the core issues in the reform of the medical system.Accordingly,when choosing the best approach,the most suitable screening technology based on the capacity of the primary medical services and the health needs of the population must be taken into consideration.Considerable data show that establishing sustainable cytology-based cervical cancer screening systems is very difficult in developing countries,which are limited by low economic levels and health service staff shortages(16).Hence,this technique has not been successfully applied in developing countries.In recent years,in the cervical cancer screening guidelines of Europe,the United States,and other countries or regions and the WHO,it is proposed thatHPV testing and HPV detection technology can be applied to the screening of cervical cancer as an alternative to cytological screening because of the advantages of high sensitivity(at least 90%)(17,18),objectivity,repeatability and batch operation(19,20).
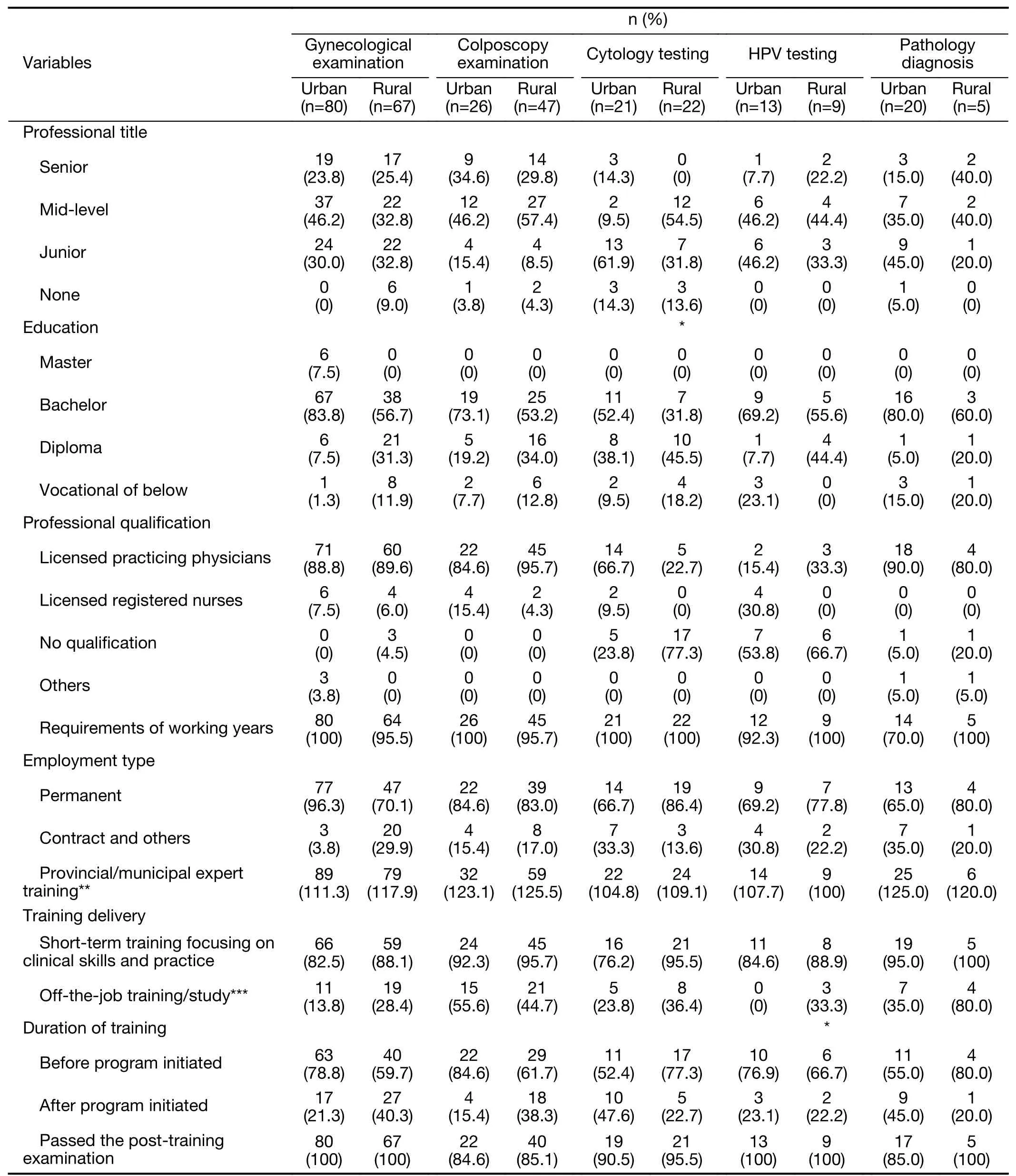
Table 7 Basic information and service capacity of medical personnel involved in NCCSP by screening/diagnosis procedure
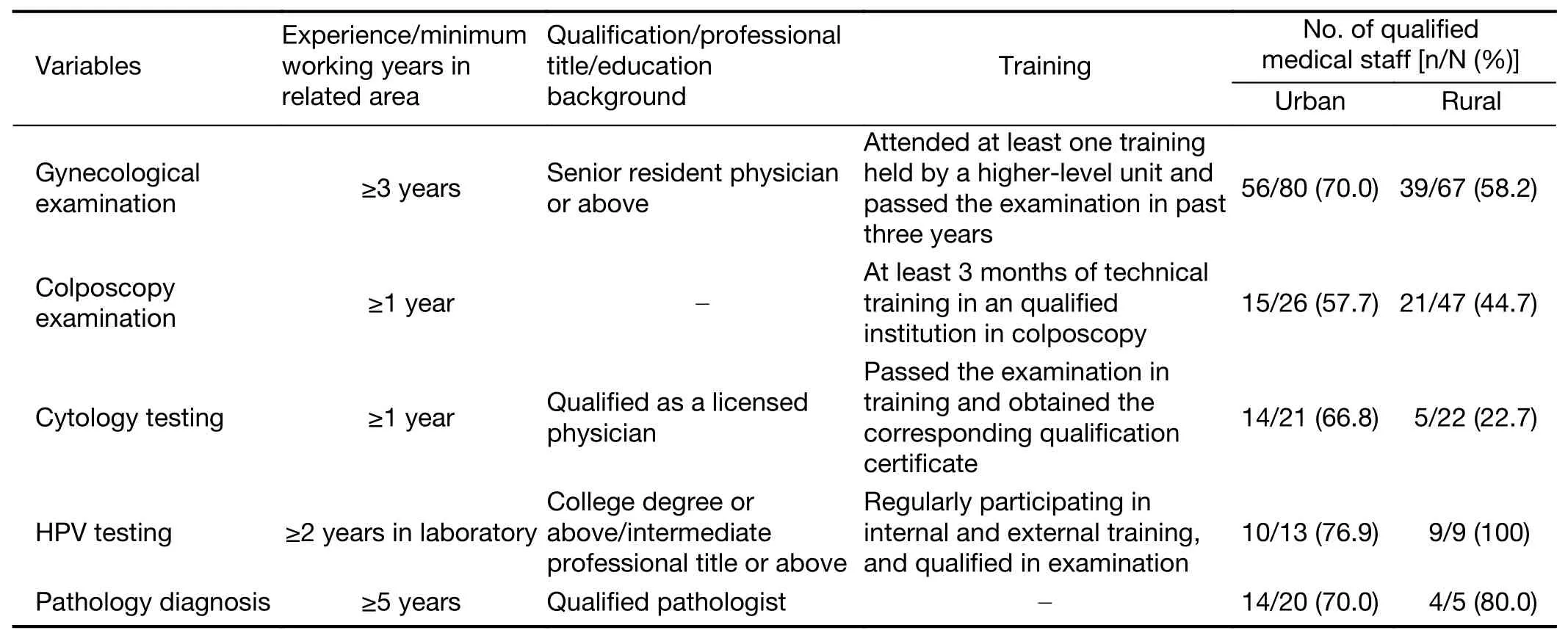
Table 8 Number of qualified medical staff meeting standards of NCCSP
This survey found that institutions that can conduct cervical cytology testing not only were rare but also had poor diagnostic techniques.HPV testing might be an option to satisfy females’demands for cervical cancer screening given the current health service capacity in China.In terms of personnel growth,the increase in the number of medical personnel engaged in HPV testing was the fastest.In terms of the quality of medical personnel,the majority of them achieved a Bachelor’s degree.HPV detection methods could be operated in batches,and less time was spent in completing the test by medical staff who used HPV detection than medical staff who used cytology testing.In addition,the HPV detection method has the advantages of objectivity,a short time to obtain results,and being easy to repeat,and it has been advancing rapidly in primary medical institutions in China with extensive application in practice.
We suggest that appropriate cervical cancer screening technologies should be selected according to the economic affordability of different regions.HPV testing with genotyping that can better distinguish between the immediate and long-term risks of HPV infection(21-23)is more suitable for urban areas with strong economic development and adequate health service capacity.In underdeveloped areas,suitable technologies for cervical cancer that are easy to operate and have relatively low requirements for operating conditions may be a better option,such as the rapid,accurate,safe and low-cost careHPV test developed by the Chinese research team(24,25).
Inadequacies of study
The data of this survey are from 2015,which only reflect the service capacity at this time.With the continuous progress of screening,the service capacity of the area is also improving,so the service capacity of primary medical institutions should be tracked.However,the results of this study show that now the critical factor of the inadequate service capacity of primary medical institutions is the quantity and quality of staff.In terms of quantity,it is difficult to solve this problem in a short time because of the limitation of the staffing of public hospitals in China.The quality problems mainly focus on the education background of personnel,which is not affected by time,and the training of personnel,which has met the national requirements.
Conclusions
The results of this study reflect the service capacity of primary medical institutions and have a certain reference significance for the sustainable development of the cervical cancer screening project.The current health service capacity has provided some support for cervical cancer screening to some extent in China,but it is still unable tocompletely satisfy the demand of cervical cancer screening in Chinese population.The key solution is to choose a suitable screening technique based on the health service capacity and population health demand of areas.HPV testing might be an optimal choice given the current health service capacity in China.
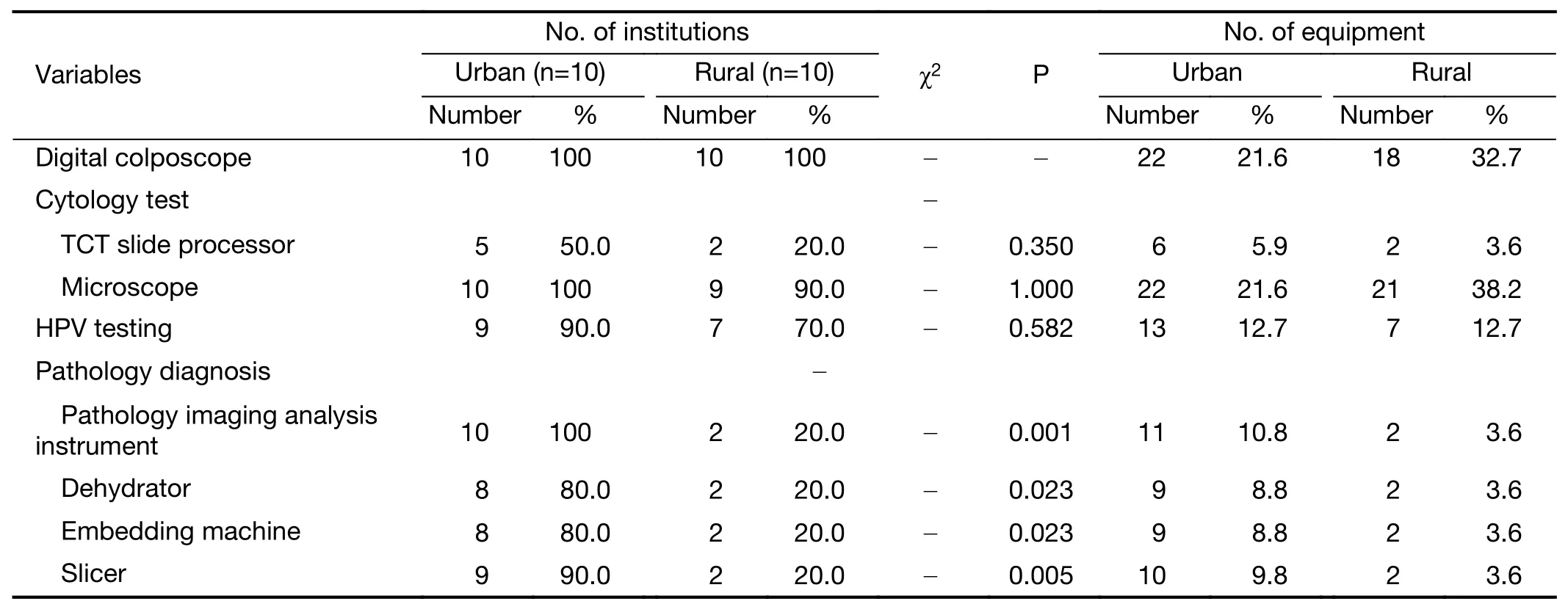
Table 9 Equipment utilization in NCCSP
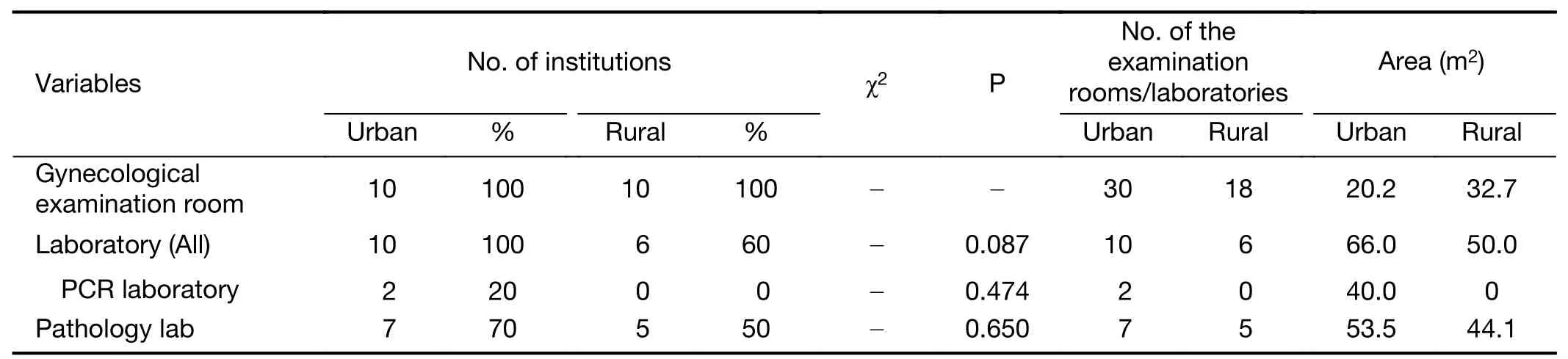
Table 10 Examination rooms/laboratories utilized in NCCSP
Acknowledgements
This study was supported by the National Health Commission of the People’s Republic of China(formerly the Health and Family Planning Commission of China)(No.201502004).
Footnote
Conflicts of Interest:The authors have no conflicts of interest to declare.
 Chinese Journal of Cancer Research2019年5期
Chinese Journal of Cancer Research2019年5期
- Chinese Journal of Cancer Research的其它文章
- Medical expenditures for colorectal cancer diagnosis and treatment:A 10-year high-level-hospital-based multicenter retrospective survey in China,2002-2011
- Surgical outcomes of hand-assisted laparoscopic liver resection vs.open liver resection:A retrospective propensity scorematched cohort study
- Texture analysis on gadoxetic acid enhanced-MRI for predicting Ki-67 status in hepatocellular carcinoma:A prospective study
- Machine-learning-assisted prediction of surgical outcomes in patients undergoing gastrectomy
- Prognostic significance of lymphovascular infiltration in overall survival of gastric cancer patients after surgery with curative intent
- Phosphoglucose isomerase gene expression as a prognostic biomarker of gastric cancer