
Helicobacter pylori and gastric cardia cancer:What do we know about their relationship?
2020-05-19 06:22:20JingJingYinFuJiaoDuanSailajaVatsalyaMadhurapantulaYueHuaZhangGuiHeKunYanWangXuanKeJiKaiJuanWang
World Journal of Meta-Analysis 2020年2期
Jing-Jing Yin, Fu-Jiao Duan, Sailaja Vatsalya Madhurapantula, Yue-Hua Zhang, Gui He, Kun-Yan Wang,Xuan-Ke Ji, Kai-Juan Wang
Jing-Jing Yin, Fu-Jiao Duan, Sailaja Vatsalya Madhurapantula, Yue-Hua Zhang, Gui He, Kun-Yan Wang, Xuan-Ke Ji, Kai-Juan Wang, Department of Epidemiology and Health Statistics, College of Public Health, Zhengzhou University, Zhengzhou 450001, Henan Province, China
Jing-Jing Yin, Fu-Jiao Duan, Sailaja Vatsalya Madhurapantula, Yue-Hua Zhang, Gui He, Kun-Yan Wang, Xuan-Ke Ji, Kai-Juan Wang, Key Laboratory of Tumor Epidemiology of Henan Province,Zhengzhou 450052, Henan Province, China
Abstract
Key words: Gastric cardia cancer; Helicobacter pylori; Cytotoxin-associated gene A;Relationship; Risk factors; Meta-analysis
INTRODUCTION
In modern society, cancer has become a significant cause of morbidity and mortality worldwide.At present, the incidence of gastric cardia cancer is increasing around the world[1,2].Gastric cardia cancer stands out distinctly and is different from gastric cancer and esophageal cancer[3,4].It is relatively insidious, and the degree of cancer cell differentiation is low.Gastric cardia cancer also has extensive invasion and rapid metastasis.Gastric cardia cancer has seriously endangered human health and has become a significant public health problem[5].This cancer occurs in the region of the gastric cardia, which is located at the junction of the stomach and esophagus.It is the transitional zone between the distal esophageal mucosa and the proximal gastric mucosa.Gastric cardia cancer always occurs on the lesser curvature side of the gastric cardia (~75%), followed by the posterior and anterior walls, and the greater curvature side is rarely affected.
Gastric cardia cancer is neither esophageal cancer nor gastric cancer.There are many differences among the three.Scholars have found that the incidence of esophageal cancer and gastric cardia cancer increased, while the incidence of distal gastric cancer decreased[6-8].Many epidemiological, histopathological, and molecular biological studies have showed that there are some similarities between gastric cardia cancer and distal esophageal adenocarcinoma, but gastric cardia cancer is different from distal gastric cancer and esophageal squamous cancer.Gastric cardia cancer and the other two cancers have not only different pathogenesis, but also have different prognostic factors.Besides, esophageal adenocarcinoma mainly spreads to the parastatal lymph nodes and the lower posterior mediastinum, while gastric cardia carcinoma has the characteristic of bilateral metastasis to the chest and abdominal cavity.
For the definition of gastric cardia cancer, there are few international definitions.Gastric cardia cancer is defined as cancer occurring at the anatomic site of the cardia,within 2 cm below the esophagogastric junction[9].The Siewert[3]classification is another standard classification scheme.It differentiates the following three distinct tumor entities in the area of the esophagogastric junction:Esophageal tumor (type I),true cardia tumor (type II), and subcardial gastric carcinoma (types III).The World Health Organization (WHO) classification of tumors classified gastric cardia cancer as tumors of the esophagogastric junction in 2000.The literature states that“adenocarcinomas that cross the esophagogastric junction are called adenocarcinoma of the esophagogastric junction, regardless of where the bulk of the tumor lies.”
Some scholars believe that the formation of gastric cardia cancer has undergone multi-stage pathological processes such as cardia inflammation, intestinal metaplasia,intraepithelial neoplasia, carcinomain situ, and invasive cancer[10].There are many reasons for the formation of gastric cardia cancer, and the development of gastric cardia cancer is the result of multiple factors interacting in various stages.
EPIDEMIOLOGY OF GASTRIC CARDIA CANCER
The age-standardized incidence of gastric cardia cancer (per 100000 cases) in different parts of the world was shown in the study of Colquhounet al[11].It showed that Eastern/Southeastern Asia had a higher incidence of gastric cardia cancer than other regions in the world, at 8.7 per 100000 for males and 2.4 per 100000 for females.The incidence of gastric cardia cancer in Sub-Saharan Africa was lower than that in other regions, at 0.2 per 100000 for males and 0.1 per 100000 for females.Gastric cardia cancer was more common in males than in females.
China has a higher incidence of gastric cardia cancer in the world.Epidemiological data showed that the incidence of esophageal and gastric cardia cancer was consistent.China is a high incidence area of esophageal cancer, and many studies suggested that the incidence of gastric cardia cancer is also high in this area, where esophageal cancer has a high incidence.This phenomenon has been observed in China’s Linxian (Henan Province)[12], Cixian (Hebei Province)[13], Chaoshan(Guangdong Province)[14], and other areas with a high incidence of esophageal cancer.
RELATIONSHIP BETWEEN HELICOBACTER PYLORI INFECTION AND GASTRIC CARDIA CANCER
Helicobacter pylori (H.pylori), which colonizes specifically in the human stomach, was first identified from patients with peptic ulcer disease by Barry Marshall and Robin Warren[15].The prevalence ofH.pyloriinfection in most countries in the world remains high.According to Hooiet al[16], there were 4.4 billion cases ofH.pyloriinfection worldwide in 2015.Africa had the highest percentage ofH.pyloriinfection (70.1%;95% confidence interval [CI]:62.6-77.7), while the lowest percentage was observed in Oceania (24.4%; 95%CI:18.5-30.4).Nigeria had the highestH.pyloriinfection rate of any country (87.7%; 95%CI:83.1-92.2).The prevalence ofH.pyloriin Latin America cannot be underestimated.A meta-analysis in a study by Curadoet al[17]suggested thatH.pyloriinfection rates are high in all age groups in Latin America.Differences in social and economic conditions across different countries might also affect the infection rate ofH.pylori[18].It was associated with many diseases[19-21], especially gastric cancer[22-24].
H.pyloricolonizes uniquely in the human stomach.Severe diseases caused byH.pyloriinfection are related to the host, bacteria, and environment, such as some gastrointestinal disorders[25].There is also a link between gastric cardia cancer andH.pylori.Therefore, the purpose of this paper was to find out the relationship between them through literature review and meta-analysis (Supplementary Figure 1).
Data from GLOBOCAN 2018 showed thatH.pyloriinfections account for 35.7% of cancers caused by infection-related factors worldwide, ranking first.It showed more details about the proportion of cancers caused byH.pyloriinfection in various regions of the world (Figure 1).The top three areas were:Central and Eastern Europe (49.3%),East Asia (47.6%), and West Asia (45.2%).These data showed the seriousness of the harm ofH.pylorito humans.
Relationship between H.pylori infection and gastric cardia cancer by region
Table 1 shows theH.pyloriinfection rates and age-standardized incidence of gastric cardia cancer (per 100000 cases) in different parts of the world, based on the studies of Colquhounet al[11]and Hooiet al[16].The data showed that the infection rate ofH.pyloriwas also high in several regions with a high incidence of gastric cardia cancer.However, although the infection rate ofH.pyloriwas as high as 76.9% in Africa and Western Asia, the incidence of gastric cardia cancer was relatively low.Therefore,these data revealed a correlation between gastric cardia cancer andH.pylorito some extent.
Data from some Western countries showed thatH.pyloriwas a protective factor for gastric cardia cancer, or there was no pathogenic relationship between these two.A nested case-control study of a Norwegian population by Hansenet al[26]and others found that gastric cardia cancer was negatively associated withH.pylori(odds ratio[OR] = 0.27, 95%CI:0.12-0.59).Yeet al[27]found no correlation between gastric cardia cancer andH.pyloriinfection based on the native Swedish population who were younger than 80 years.
However, studies in China, Japan, and other Asian countries have shown thatH.pyloriwas the pathogenic factor for gastric cardia cancer.A cohort study by Kamangaret al[28]on 29584 residents in Linxian (Henan Province, China) suggested thatH.pyloriinfection was a risk factor for gastric cardia cancer (hazard ratio [HR] = 1.64; 95%CI:1.26-2.14).Yasuoet al[29]also found that 75% of Japanese patients with gastric cardia cancer hadH.pyloriinfection, andH.pyloriinfection was closely associated with gastric cardia cancer.
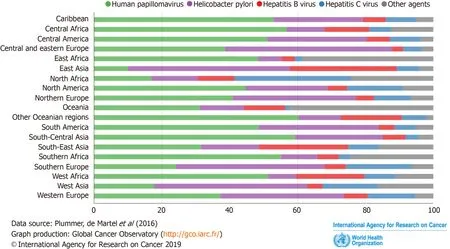
Figure 1 Proportions of cancer cases among both sexes attributable to infections in 2012 (by region).
Marlene[30]and others conducted a meta-analysis of the research on the relationship betweenH.pyloriinfection and gastric cardia cancer.The population of this study included people from all over the world.The results of the study showed that for gastric cardia cancer, the pooled relative risk (PRR) was 1.08 (95%CI:0.83-1.40;I2=52.8%), but the difference was not statistically significant.Subsequently, those authors divided the regions into high incidence areas and low incidence areas based on the incidence of gastric cancer.China, Japan, and South Korea were classified as high-risk settings, while Australia, Finland, Germany, United States,etc.were classified as lowrisk Settings.The results showed thatH.pyloriinfection was a risk factor for gastric cardia cancer in the high incidence areas of gastric cancer (RR = 0.78, 95%CI:0.63-0.97;I2= 11.6%).This result suggested that geographical factors could affect the relationship betweenH.pyloriand gastric cardia cancer.
Also, as mentioned above, although gastric cardia cancer was classified as a type of esophagogastric junction cancer by the WHO in 2000, there are still inconsistencies in the diagnostic criteria for gastric cardia cancer among many current studies.In the study of Hansenet al[26], the diagnosis of gastric cardia cancer was based on International Classification Atom of Diseases for Oncology (second edition).Inconsistencies in the diagnostic criteria for gastric cardia cancer may also lead to a wrong diagnosis, thus affecting the relationship between gastric cardia cancer andH.pyloriand leading to inconsistent research results.
Relationship between H.pylori virulence factor cagA and gastric cardia cancer:A meta-analysis
The virulence factor genes ofH.pyloriincludevacA, cagA, cagE, oipA, babA2, babB, andiceA,etc.[31,32].H.pylorivirulence factors play an important role in the progression of gastric cardia cancer.Cytotoxin-associated gene A (cagA) is a virulence factor ofH.pylorithat has been studied most in the world.CagA is located at one end of the cag-PAI (a 40-kb piece of DNA) and is likely to be incorporated into theH.pylorigenome through a horizontal transfer process[33].CagA was only found inH.pylorihighly virulent strains.H.pyloricagA protein appears as a bacterial oncoprotein[34].Leeet al[35]showed that people infected withH.pyloriwhich contains the cagA protein produce more reactive oxygen species and have an increased risk of gastric cancer.CagA protein is the only bacterial oncoprotein identified to date.CagA contains two repeatable protein-binding motifs, the Glu-Pro-Ile-Tyr-Ala (EPIYA) motif and the cagA multimerization (CM) motif.There are two major pathological and biochemical processes that contribute toH.pyloricagA-induced gastric cancer:Abnormal cancerpromoting signals caused by SHP2 imbalanceviathe EPIYA motif, and gastric epithelial destruction caused by CM-mediated PAR1 inhibition[36].EPIYA motifs are divided into four categories (EPIYA-A, -B, -C, and -D), depending on the amino acid sequence surrounding each EPIYA motif, and they have different characteristics[37].
The current research results on the relationship between cagA and gastric cardia cancer are also controversial.In the study by Limburget al[38], the adjusted OR value of cagA positive gastric cardia cancer patients compared with cagA negative patients was 1.79 (95%CI:1.05-3.06), indicating that cagA positivity was a risk factor for patients with gastric cardia cancer.Some other studies showed that there was asignificant negative correlation between cagA positivity and the development of gastric cardia cancer.Yeet al’s[27]study showed that cagA positivity was not associated with the risk for gastric cardia adenocarcinoma (OR = 1.00, 95%CI:0.70-1.60).Therefore, we performed a meta-analysis of the relationship betweenH.pyloricagA and gastric cardia cancer.
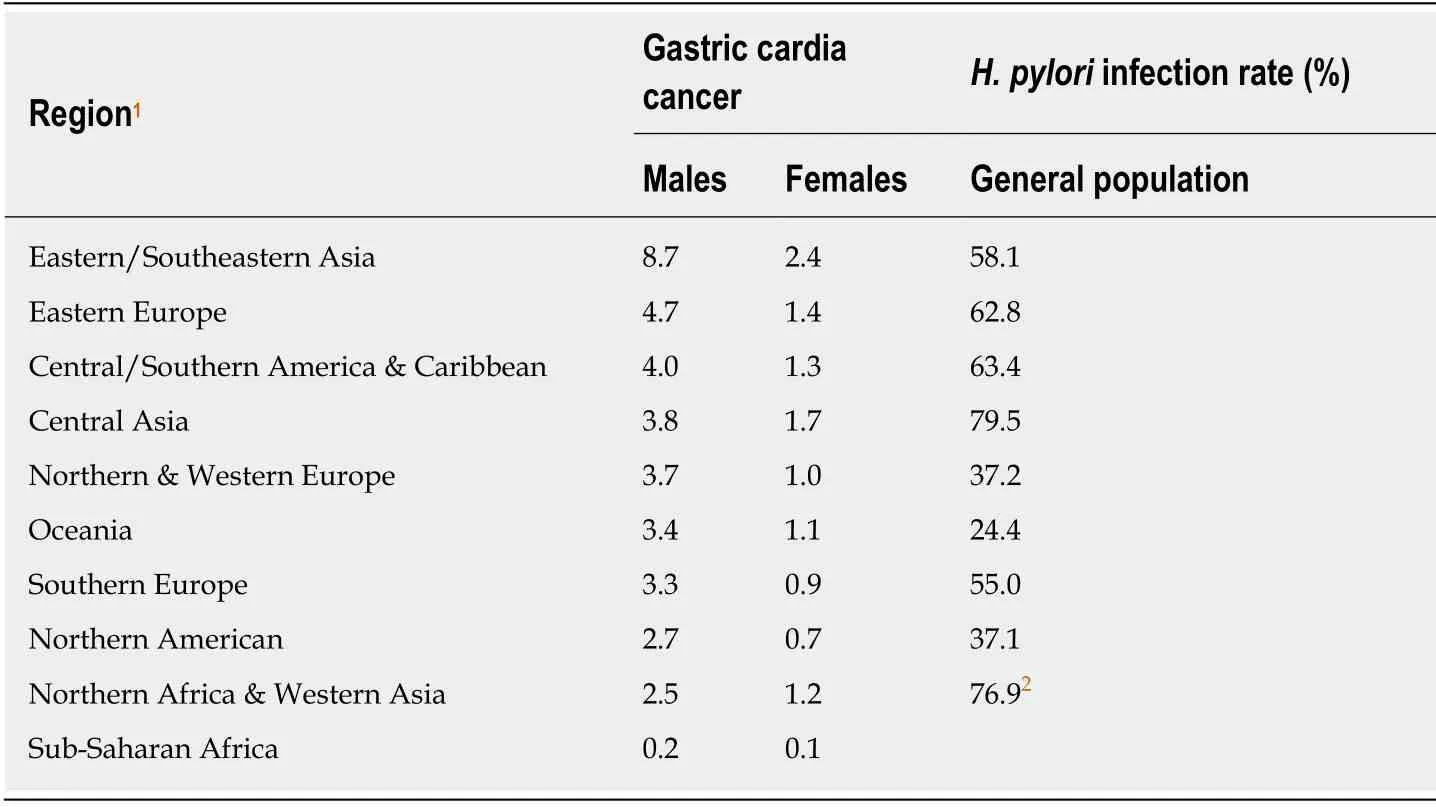
Table 1 Gastric cardia cancer age-standardized incidence rates (per 100000) and Helicobacter pylori infection rates
The study was based on the guidelines of Meta-analysis of Observational Studies in Epidemiology (MOOSE)[39]and the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA)[40].PubMed, Web of Science, Embase, Cochrane Library,Chinese National Knowledge Infrastructure (CNKI), and Wanfang (China) electronic databases were searched for relevant articles published up to December 2019.The search items were “gastric cardia cancer” and “Helicobacter pyloricagA”.
The quality of the eligible studies (Supplementary file 1) was evaluated according to the Newcastle-Ottawa Scale (NOS)[41](Supplementary Table 2), and articles with a score higher than six were considered high-quality.The STATA (Version 13.1 MP,Stata Corp, College Station, TX, United States) was used to analyze the data.P< 0.05 orI2> 50.0% was considered to have significant heterogeneity.A fixed-effects model was used when there was no significant heterogeneity, otherwise a random-effect model was used.A sensitivity analysis was performed to evaluate the stability of the pooled results.Egger’s test[42]and Begg’s test[43]were used to assess the extent of publication bias.P< 0.05 was considered statistically significant, and all statistical tests were two-sided.
After screening, a total of 12 articles were included in the study[27,38,44-53].The random-effects model (I2= 42.2%,P= 0.099) and fixed-effects smodel (I2= 42.2%,P=0.060) were used for heterogeneity testing, respectively.The results of the heterogeneity test showed no significant difference.The sensitivity analysis showed that the combined OR did not change significantly, indicating that the combined OR was fairly stable.ThePvalues of Egger’s and Begg’s tests were 0.277 and 0.244,respectively.Detailed results are shown in the Supplementary Materials.The fixedeffect model was eventually selected for use (Figure 2).The pooled OR of this study was 1.03 (95%CI:0.84-1.26).The results could not indicate thatH.pyloricagA positivity is a risk factor for gastric cardia cancer (Supplementary Figures 2-4).
Other relationships between H.pylori and gastric cardia cancer
H.pyloriinfection in different parts of the gastric cardia mucosa is different, which is consistent with the difference in the incidence of gastric cardia cancer in different regions.The distribution ofH.pyloriinfection in the cardia mucosa is characterized by the invasion of both sides of the root of mucosal fold in the cardia.The high incidence area of gastric cardia cancer overlap with the high infection area ofH.pylori.In the course of gastric cardia cancer,H.pyloriinfection in the cardia and gastric antrum mainly promotes the occurrence of the tumor.H.pyloriinfection also affects the prognosis of patients with gastric cardia cancer.H.pylorimay be related to the prediction of gastric cardia cancer, but it is not an independent factor.
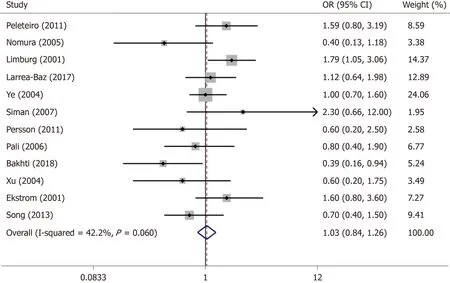
Figure 2 Forest plot of studies evaluating the odds ratios of Helicobacter pylori cagA positive expression for gastric cardia cancer.
OTHER RISK FACTORS FOR GASTRIC CARDIA CANCER
Gastric cardia cancer is a multi-factorial ailment, which is the result of the interaction of multiple factors, including genetic factors, environmental factors,etc.
Demographic characteristics such as age, gender, and ethnicity are all factors influencing gastric cardia cancer.The incidence of gastric cardia cancer increases in the elderly, and the research by Chenet al[14]showed that the population of 50-80 years had a high incidence of gastric cardia cancer.Several other studies suggested that gastric cardia cancer is more prevalent in males.Colquhoun[11]and others showed that the incidence of gastric cardia cancer was significantly higher in males than in females(male:female = 3:1).Kuboet al[54]and others, through the analysis of five groups of cancer registration data (1992-1998), also found a high incidence of gastric cardia cancer in males.
Current studies have found that many tumors have a family genetic predisposition,and studies on the relationship between gastric cardia cancer and family history have found a correlation between these two.Yanget al[55]investigated 16605 patients with gastric cardia cancer and 26053 patients with non-cardia cancer through questionnaires.And after a long period of follow-up of 2000 patients, they found that positive family history significantly increased the risk of gastric cardia cancer.
Yanget al[55]found that smoking significantly increased the risk of gastric cardia cancer (OR = 1.98, 95%CI:1.79-2.19).The results of the study by Zendehdelet al[56]also showed that compared to never-users of any tobacco, smokers had an increased risk for gastric cardia cancer (RR = 2.10, 95%CI:1.50-3.00).Obese subjects (BMI ≥ 30 kg/m2) had a higher risk of gastric cardia cancer than the average population (RR =2.73, 95%CI:1.56-4.79), according to the results of a prospective cohort study in the Netherlands[57].Also, Janssonet al's[58]study showed a correlation between covert coping strategies when maltreated at work and the risk of gastric cardia cancer.
Genetic risk factors, epigenetic risk factors, long noncoding RNAs, and microRNAs are all in the field of molecular biology.For example, a tumor suppressor protein encoded by thep53gene often mutates in many kinds of cancers and is related to cell proliferation and tumor growth[59].Shao’s[60]study showed that after Bonferroni correction, the association between TP53BP1 rs560191 G4C and gastric cardia cancer remained significant.The advent of multiple genome-wide association studies has led to the successful identification of many single nucleotide polymorphisms (SNPs),including those associated with gastric cardia cancer.Xiaoet al’s[61]study also showed that the interaction between SNPs andH.pyloriinfection is related to the increased risk of gastric cardia cancer.In Abdiet al’s[62]study, the factors of molecular biology of gastric cardia cancer were studied more specifically, including not only SNPsd but also long noncoding RNAs and microRNAs.
CONCLUSION
This article discusses the relationship betweenH.pyloriand gastric cardia cancer;however, the relationship betweenH.pyloriand gastric cardia cancer could not be analyzed generally.Accurate classification of gastric cardia cancer and patients'geographic factors can influence the relationship betweenH.pyloriand gastric cardia cancer.Also,H.pylorihas a large number of different virulence factors.In this study,only the relationship between the positive expression of cagA and gastric cardia cancer was meta-analyzed, but no correlation between these two was found.The effects of other virulence factors on gastric cardia cancer need to be further studied.BothH.pylorirelated hosts and the environment may have an impact on cardia cancer, which has not been discussed in depth in our research.In addition, the impact of family history on the relationship betweenH.pyloriand gastric cardia cancer, and even the relationship between eradication ofH.pyloriand gastric cardia cancer were not included in this study, which need further research.
 World Journal of Meta-Analysis2020年2期
World Journal of Meta-Analysis2020年2期
- World Journal of Meta-Analysis的其它文章
- Effectiveness and safety of sedation in gastrointestinal endoscopy:An opinion review
- Chinese research into ulcerative colitis from 1978 to 2017:A bibliometric analysis
- Single-balloon and spiral enteroscopy may have similar diagnostic and therapeutic yields to double-balloon enteroscopy:Results from a meta-analysis of randomized controlled trials and prospective studies
- Systematic review with meta-analysis of the epidemiological evidence relating smoking to type 2 diabetes
- Utility of gastrointestinal ultrasound in functional gastrointestinal disorders:A narrative review
- Treatment strategies and preventive methods for drug-resistant Helicobacter pylori infection