
Utility of gastrointestinal ultrasound in functional gastrointestinal disorders:A narrative review
2020-05-19 06:22:22AndrewMingLiangOng
World Journal of Meta-Analysis 2020年2期
Andrew Ming-Liang Ong
Andrew Ming-Liang Ong, Department of Gastroenterology and Hepatology, Singapore General Hospital, Singapore 169856, Singapore
Andrew Ming-Liang Ong, Duke-NUS Medical School, Singapore 169857, Singapore
Abstract
Key words: Ultrasound; Functional gastrointestinal disorders; Irritable bowel syndrome;Functional dyspepsia; Constipation
INTRODUCTION
Gastrointestinal (GI) ultrasound (GIUS) is increasingly recognised as a valuable tool in the evaluation of GI disease[1], especially in inflammatory bowel disease (IBD)where it has a similar diagnostic yield to endoscopy and cross-sectional imaging[2].
Functional GI disorders (FGIDs) are disorders of gut-brain interaction related to mechanisms such as motility disturbances, visceral hypersensitivity and altered central nervous system processing[3].Their diagnoses rest on symptom-based criterias and exclusion of organic diseases.Although it is suggested that physicians make a positive diagnosis of FGID and minimize investigations[4], many perform a limited set of tests, with normal endoscopies often being the “confirmation” of a FGID[5].GIUS have been recommended by some society guidelines to rule out organic diseases before diagnosing a FGID[6,7].As such, the primary goal of this review is to discuss the current and potential utility of GIUS in the evaluation of FGID, focusing on common FGIDs such as IBS and functional dyspepsia (FD).As part of the review, we will discuss how clinicians can take advantage of the unique nature of GIUS to evaluate upper and lower GI physiology, exclude organic disease, guide treatment decisions and build rapport with patients.
A literature search was conducted using Medline (1946 to February 2019), EMBASE(1947 to February 2019) and Google Scholar databases using a combination of MESH and keyword search terms:“ultrasound”, “functional GI disorders”, “irritable bowel syndrome”, “functional dyspepsia”, “intestinal ultrasound”, “point of care ultrasonography”, “transabdominal sonography”, “motility”, “faecal loading” and“constipation”.Papers not written in English were excluded.
EVALUATING GI PHYSIOLOGY
The GI tract is a unique system, with many organs performing multiple different functions.Thus, it is challenging to thoroughly assess GI function using currently available imaging techniques, which mainly evaluate anatomical structures.GIUS allows real-time evaluation of organ function, in addition to structure, and can provide a wide array of information on physiology such as motility, biomechanics,flow, and organ filling/emptying[8].
For example, GIUS allows real-time dynamic assessment of intestinal peristalsis to narrow down possible differential diagnoses as diminished peristalsis can indicate an unhealthy bowel seen in small bowel inflammation, obstruction, ischemia, and infiltrative processes[9].If a transition point with a collapsed distal bowel is also seen,this may suggest mechanical obstruction[10].Certain patterns can be seen in malabsorptive conditions like coeliac disease, where small bowel wall thickening is seen with hyperperistalsis causing a constant to-and-fro movement of luminal content[11].
FD is a common FGID with many putative pathophysiological mechanisms including antral hypomotility, antroduodenal dyscoordination, impaired accommodation, delayed gastric emptying and gastric hypersensitivity, each of which could contribute to the various subtypes[12,13].It is important to consider the contributing pathophysiology to symptoms in each patient[13]as newer treatment options are available to target specific pathophysiological disturbances[12].GIUS offers the benefit of evaluating more than one mechanism in a single test.
GIUS has been used to evaluate gastric emptying for more than 30 years[14]and has been shown to have good correlation to the “gold standard”[15]of gastric emptying measurement:Scintigraphy, with the benefit of no exposure to ionising radiation.GIUS has shown good reliability and interobserver agreement in the measurement of gastric emptying rates[16], and is cheaper and more easily repeatable compared to other modalities such as wireless motility capsules, gastric emptying breath tests and MRI[17].This process of gastric emptying is complex and affected by many factors such as antral contractions, antroduodenal coordination, proximal gastric relaxation and pyloric tone[18], but most investigational modalities look at only a single aspect of gastric emptying[19].GIUS overcomes this by providing real-time information on multiple parts of gastric physiology[20].For example, GIUS can demonstrate gastric contractions and measure the frequency and amplitude of these contractions[21,22], thus investigators can visualise whether delayed gastric emptying is due to an abnormally intense pyloric contractility or antral hypomotility[23], as treatment options may differ depending on the finding[24].GIUS can also assess the stomach’s ability to accommodate after meals[25], which is another mechanism contributing to FD symptoms, with dyspeptic patients showing smaller proximal stomach volumes after meals[26,27].
CLINICAL UTILITY IN EXCLUDING ORGANIC DISEASES
Differentiating between FGID and organic diseases can sometimes be difficult.One of the competing diagnoses for IBS is IBD which may also affect a similar demographic profile of patients[28].It is particularly important for a timely diagnosis of IBD to be made, as delay in treatment can result in the development of complications.Laboratory markers such as C-reactive protein and faecal calprotectin are not always accurate predictors of inflammation[29,30].Colonoscopy and cross-sectional imaging modalities have been longstanding stalwarts of the diagnostic armamentarium for IBD.However, colonoscopy is invasive and requires bowel preparation and sedation,CT imaging has the risks of ionising radiation, and MRI is costly and time-consuming.
GIUS has the benefit of being less costly, non-invasive and widely available,making it particularly useful in areas where healthcare resources are limited.It obviates the need for sedation, fasting or bowel preparation, making it ideal for repeated real-time use in clinics.GIUS also allows the managing clinician to perform the targeted examination, so decisions on therapy can be made in the right clinical context.
A prospective, real-world study[31]on consecutive patients presenting to a gastroenterology unit with symptoms suggestive of bowel disease, showed that the overall sensitivity and specificity of GIUS compared to radiological and endoscopic studies for bowel disorders was 85.4% and 95.4%, respectively.Another study[32]looked at 58 consecutive symptomatic patients presenting to a gastroenterology clinic and found GIUS to have an overall sensitivity and specificity of 80% and 97.8%respectively compared to endoscopy in identifying inflammatory causes of their symptoms.GIUS could differentiate IBS and IBD patients in a consecutive series of 313 patients[33]admitted to an outpatient clinic with non-specific chronic abdominal pain and bowel dysfunction with GIUS having 74% sensitivity and 98% specificity in detecting IBD compared to radiological and endoscopic studies.These studies suggest that GIUS can serve as a useful tool in differentiating IBD from FGID.Furthermore,GIUS can be used to triage patients and decide the urgency of investigations.GIUS can help support timing and urgency of endoscopy, as a negative GIUS together with a normal CRP and faecal calprotectin makes IBD very unlikely and therefore further investigations unnecessary[32,33].Furthermore, the cases missed by GIUS were mild endoscopically, and often did not need urgent treatment[32,33].In addition, they could be followed with serial GIUS scans to determine when treatment was warranted.
FGIDs also commonly result in severe abdominal pain requiring hospital admission, and emergency physicians not familiar with the patient’s background may subject them to excessive investigations.GIUS scans have been suggested as first-line imaging tools in patients with an acute abdomen[34], and have been shown to be comparable to CT scans in the diagnosis of appendicitis[35], diverticulitis[34]and intestinal obstruction[10].The ability of GIUS to evaluate both upper and lower GI tracts, as well as intestinal and extra-intestinal features makes it a valuable initial tool when the cause of patient’s symptoms is not entirely clear.Furthermore, GIUS is able to visualise splanchnic vessels, mesentery, omentum and lymph nodes, and abnormalities in these areas lend weight to certain diagnoses[36].GIUS can also be extended to evaluate other organs to include differentials such as ascites, ruptured ectopic pregnancies[37], nephrolithiasis[38]and gallstones[39].
ASSESSING SEVERITY AND SUBTYPING IN IBS
The diagnosis of FGID is centred solely on the patient history, but there are disparities between patient reported bowel habits and objective features of constipation or diarrhoea[40,41].GIUS can objectively demonstrate constipation can help subtype IBS and educate patients, while the visualisation of the location of the faecal retention can aid the physician in choosing the appropriate treatment (Figure 1).Scoring systems[42]have been developed to report the severity of faecal loading on radiological images,by looking at the degree of faecal retention and bowel dilatation.Since GIUS has been shown to be comparable to CT scans in the visualisation of faecal loading[43], it can quantify faecal loading without exposing the patient to radiation.The severity of faecal loading can be determined on GIUS[44], with haustra-shaped acoustic reflections suggestive of “harder” faecal loading (Figure 1A), while has shown that a composite measurement of colonic diameters has been shown to be a surrogate measure of constipation[45].
There is also the potential for novel metrics to assess bowel contents.To date, MRI has been used to evaluate differences in small and large bowel content between healthy controls and patients[46], and a constricted small bowel was more commonly found in non-constipated IBS while a dilated transverse colon was more likely in IBSC[47].GIUS can potentially subtype IBS patientsviathese measurements, while offering the added benefits of being cheaper and more widely available.
There is also interest in using GIUS to assess colonic transit time which is recommended to be evaluated in chronic constipation[48].At present transit time is measured either radiologically,viaa nuclear medical study, orviawireless motility capsule which is expensive and not widely available.GIUS has been used to evaluate colonic transit time using water-filled latex balloons containing metal particles, and then following the metal particles through the stomach, small bowel and colon.In summary, GIUS has the potential to measure faecal loading, colonic diameter, and transit time in a single test.
USING GIUS TO BUILD RAPPORT WITH PATIENTS
GIUS plays a unique role in FGID patients by helping to strengthen the physicianpatient relationship through several ways.IBS patients’ have been shown[49]to yearn for (1) increased quality time spent with their healthcare provider; (2) education on their condition; and (3) reassurance that organic diseases were excluded.Since GIUS does not involve sedation, physicians can use the time during the procedure to build rapport with patients by involving them in the discussion of their condition.GIUS was shown[32]to improve patient’s understanding of their condition and was generally preferred over endoscopy.
In a study by patients attending the emergency department were randomised to bedside ultrasound or standard clinical examination[50], and higher patient self-rated satisfaction score was found in the ultrasound group with decreased short-term health care consumption.Other studies have found similar results[51,52].It has also been shown that serial imaging using ultrasound can strengthen doctor-patient relationships[53], which is a cornerstone in the management of FGID patients[3], where cognitive processes such as symptom-specific anxiety[54]may perpetuate symptoms.For example, GIUS can be used to evaluate the painful area, and then patients can be shown the images and reassured that no abnormality was detected.Subsequently,education and discussions with regard to visceral hypersensitivity can commence.Alternatively, demonstrating faecal loading can educate and convince patients of the origin of their symptoms, and pave the way to understanding treatment options.
Physicians have often been encouraged to make a positive diagnosis of FGID[55],however, the lack of biomarkers and the concern that organic causes are missed resonate with both patients and health care providers[56], further contributing to health seeking behaviour[57,58].Using GIUS as an extension of the clinician’s physical examination has been shown[39]to reduce unnecessary investigations.In their study of 1962 consecutive patients, GIUS ruled in or out diagnostic hypotheses in about twothirds of the cases, and further testing was only required in around 37% of patients.
RESEARCH APPLICATIONS
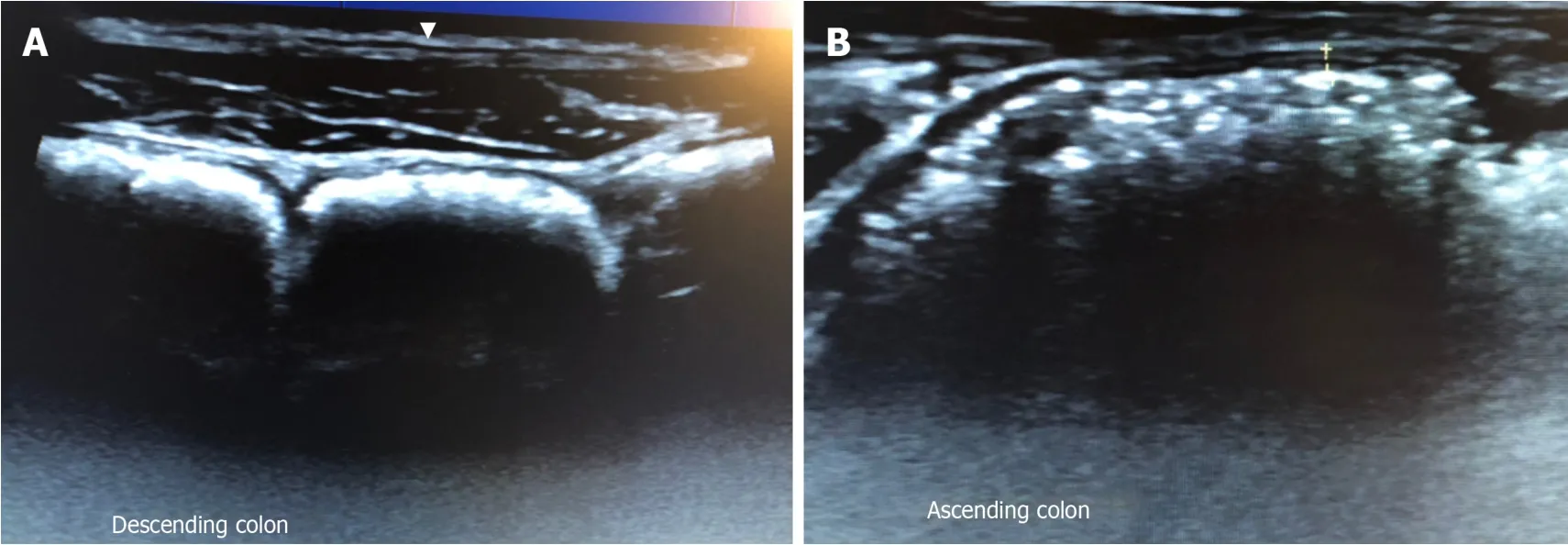
Figure 1 Gastrointestinal ultrasound images.
GIUS can determine the respective contributions of physiological findings in the GI tract to the patient’s overall symptoms by directly correlating the symptoms to these findings since the imaging is real time[59].It can analyse temporal mechanistic relations of the GI tract with medications, meals[22,59]and even stress[60], and thus is a valuable tool for research in the field of GI motility.Also, one of the major challenges in assessing treatment outcomes in patients FGID is the lack of objective biomarkers, as symptoms often show wide variability[61].Measurement of GIUS parameters can be safely and easily taken pre- and post- treatment intervention (Figure 2) to evaluate the efficacy and mode of action in real time.
An interesting use of GIUS is the evaluation of symptoms in FGID related to food intake.GIUS allows limited evaluation of the volume and content of the intestines,thus it can be used together with a food challenge to evaluate mechanisms for symptom generation.It has been shown that different types of FODMAPs generate different physiological effects on MRI scans[62].In theory, GIUS has the potential to perform some of the MRI measurements such as colonic diameter and content, and thus can be used to correlate patient’s symptoms after a substrate load, allowing greater understanding of the origin of symptoms after ingestion of certain foodstuffs,and also diagnose malabsorptive conditions such as lactose or fructose malabsorption.To demonstrate this, 32 patients with chronic abdominal complaints self-attributed to food intake were examined with GIUS after ingesting the suspected food item.The sonographic features were recorded before, during and after the food challenge, and the investigators found significant correlation between symptoms and intestinal wall thickness in the duodenal bulb and jejunum[63].
FUTURE DIRECTIONS
GIUS still does have its limitations.Not all patients are easy to evaluate using GIUS:obese patients and those with previous abdominal surgery are particularly challenging.Not all areas of the bowel are seen easily with GIUS and this may be result in over-diagnosis of pathology detected in sigmoid and terminal ileum areas,with missed pathologies in the transverse colon and rectum.Furthermore, although many studies mentioned in this review demonstrate the utility of GIUS in understanding pathophysiological mechanisms contributing to a patient’s GI symptoms, these measurements have not gained clinical relevance[19], and future studies are needed to look into GIUS measurements that may predict a worse prognosis or a response to specific treatment options.
There may be resistance to the widespread adoption of GIUS because of concern of operator ability and thus the potential to miss an important diagnosis.However, there is a slow gain in acceptance that physicians can perform focused ultrasound examinations even without previous ultrasound experience[64].It has been shown that even ultrasound-na?ve clinicians can become competent after performing around 200 supervised examinations[65].There is also a shift in perspective from a concern about missed findings to recognition that appropriate use of GIUS improves diagnostic accuracy compared to clinical examination alone[66].
CONCLUSION
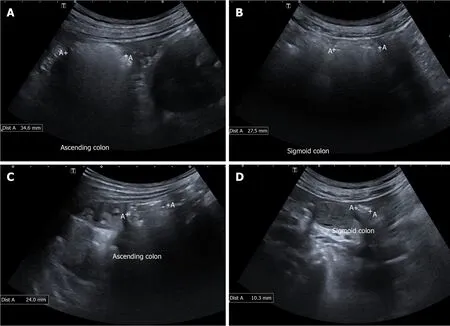
Figure 2 shows the ascending colon and sigmoid colon images of a constipated patients.
FGID are extremely common conditions seen in gastroenterology practices worldwide, and we have described the current and potential uses of GIUS in the evaluation and management of FGID (Table 1).GIUS is unique in being able to offer real-time physiological information, reliably exclude organic diseases, aid the physician in guiding treatment decisions, and also strengthen patient-physician relationships, thus it offers great potential in its use in FGID (Table 2).
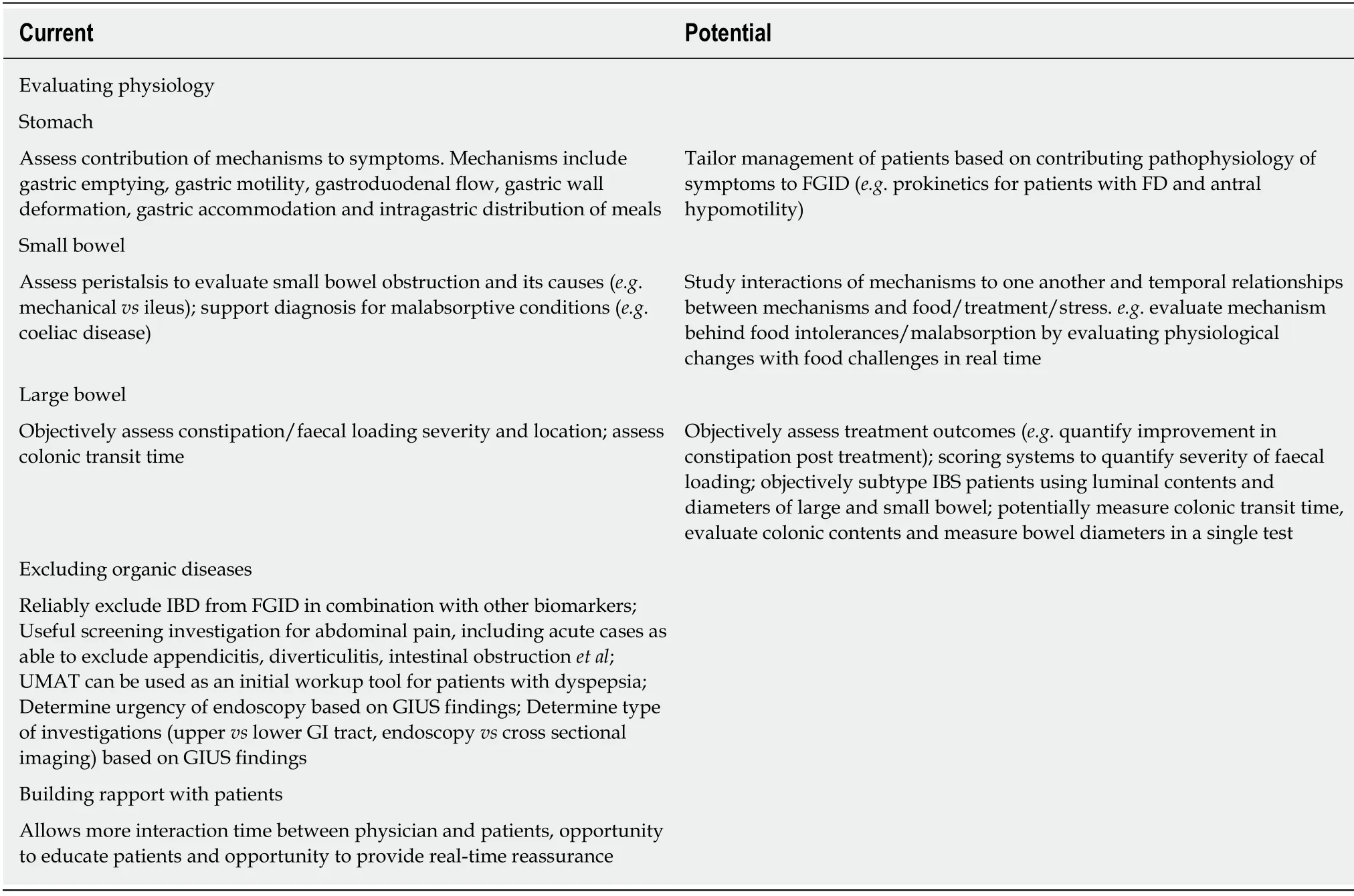
Table 1 Current and potential uses of gastrointestinal ultrasound in functional gastrointestinal disorders
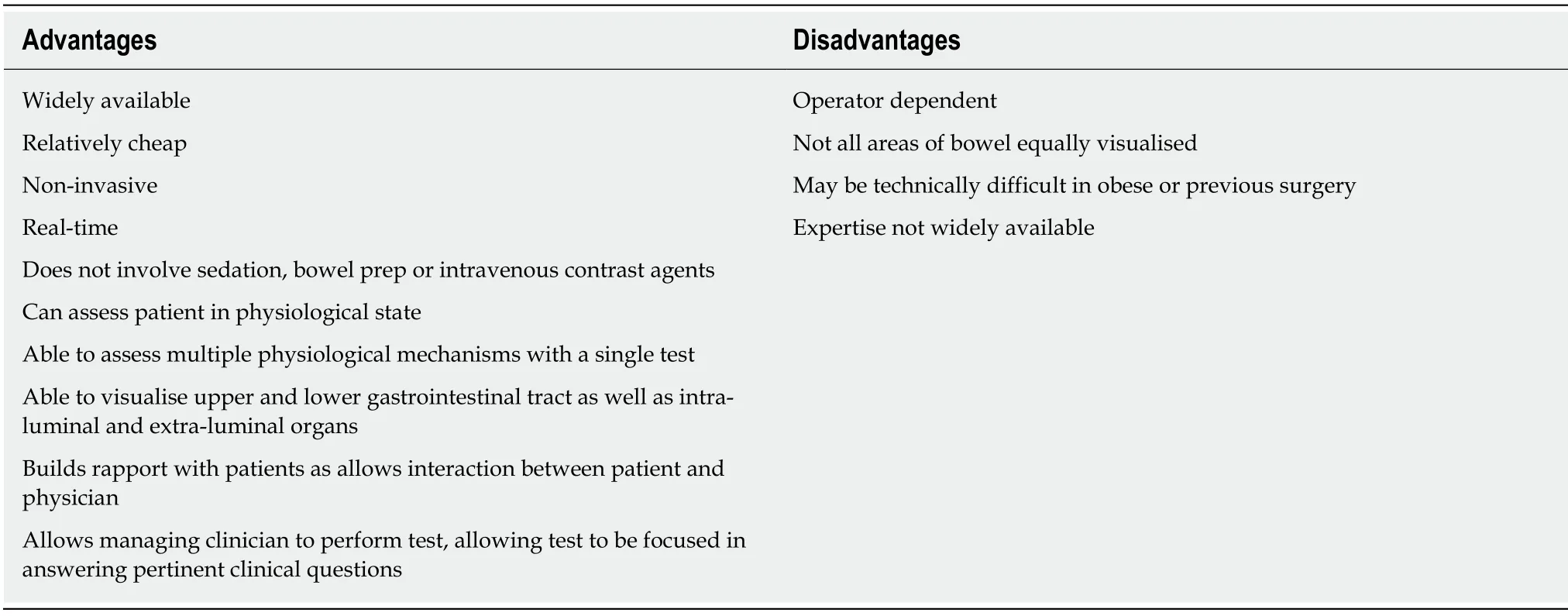
Table 2 Advantages and disadvantages of gastrointestinal ultrasound
 World Journal of Meta-Analysis2020年2期
World Journal of Meta-Analysis2020年2期
- World Journal of Meta-Analysis的其它文章
- Effectiveness and safety of sedation in gastrointestinal endoscopy:An opinion review
- Chinese research into ulcerative colitis from 1978 to 2017:A bibliometric analysis
- Single-balloon and spiral enteroscopy may have similar diagnostic and therapeutic yields to double-balloon enteroscopy:Results from a meta-analysis of randomized controlled trials and prospective studies
- Systematic review with meta-analysis of the epidemiological evidence relating smoking to type 2 diabetes
- Treatment strategies and preventive methods for drug-resistant Helicobacter pylori infection
- Helicobacter pylori and gastric cardia cancer:What do we know about their relationship?