
Comparison of vital capacity rapid inhalation and tidal ventilation induction with sevoflurane in adults:a prospective cohort study
2021-04-30 06:46:42
Medical Gas Research 2021年3期
Department of Anaesthesiology, Amala Institute of Medical Sciences, Thrissur, Kerala, India
Abstract Vital capacity rapid inhalation induction (VCRII) results in faster achievement of desired minimum alveolar concentration while reducing the incidence of excitatory phenomenon compared to conventional incremental technique.This study aimed to determine whether the VCRII can achieve faster induction of anesthesia in adults compared to the traditional tidal ventilation (TV) technique.Following the approval from the Institutional Ethics Committee, Amala Institute of Medical Sciences, with an approval No.AIMSIEC/07/2017, on July 1, 2017, 51 adults belonging to American Society of Anesthesiologists physical status I–II, undergoing elective surgery at a tertiary care teaching hospital were prospectively assigned to two groups:25 in VCRII (38.3 ± 13.3 years old, 20 (80%) females) and 26 in TV inhalation induction (35.2 ± 11.9 years old, 17 (65%) females) using 8% sevoflurane in 66% nitrous oxide.The induction time, such as time (in seconds) to the cessation of voluntary finger tapping, time to loss of eyelash reflex, time to return of regular breathing, the return of conjugate gaze, was measured.The primary outcome was time to induction as defined by time to loss of eyelash reflex.Hemodynamic effects of both methods were compared at baseline and 1, 3, 5, 10, 15-minute intervals from induction.Induction was significantly faster in the VCRII group compared with the TV group in all the measured parameters.Hemodynamic parameters were comparable in both the groups.VCRII resulted in a faster induction time compared to the TV technique in adults.
Key words:adults; excitatory phenomenon; inhalational agent; inhalational induction; minimum alveolar concentration; prospective study;sevoflurane; tidal ventilation; vital capacity
INTRODUCTION
With the advent of newer agents, inhalational induction is becoming an attractive alternative to intravenous induction.Because of its non-irritating nature and higher efficacy,sevoflurane is the preferred agent.There is evidence that inhalational induction of anesthesia is increasingly preferred by subjects over intravenous induction.1In a meta-analysis, the time to induction with sevoflurane was found to be comparable with propofol while sevoflurane was associated with higher first-time success with laryngeal mask airway insertion.2High inspired concentrations of sevoflurane are safe and do not provoke airway reflex responses as shown in a multiple adult and pediatric study.3
As required by vital capacity rapid inhalation induction(VCRII), the subject is asked to first take a deep breath followed by maximum exhalation.Afterwards, the anesthetic circuit with facemask is applied, the subject is asked to take a deep breath, hold his/her breaths for as long as possible and then breathe out to residual volume.4VCRII technique requires patient education and cooperation for a vital capacity breath and an adequate breath-hold following it.The other technique is tidal ventilation (TV) induction, in which the patient breathes normal tidal volume breaths.TV induction does not require any patient training as it involves the patient taking normal breaths.A comparison of VCRII and TV techniques performed in the pediatric age group has shown that VCRII achieved shorter time to induction and was preferred by the subjects.5This study aimed to ascertain whether the VCRII technique can result in faster induction in Asian adults compared to the traditional TV technique and to compare the incidence of adverse events using both the techniques.
SUBJECTS AND METHODS
An approval from the Institutional Ethics Committee,Amala Institute of Medical Sciences with an approval No.AIMSIEC/07/2017 on July 11, 2017 was obtained.Written informed consent was obtained from all subjects.We prospectively enrolled subjects aged 18 years and above scheduled to undergo elective urological, head and neck, orthopedic, or visceral surgeries at our tertiary care teaching hospital from June 2018 to December 2019 and belonging to the American Society of Anesthesiologists (ASA) physical status I–II.Adults with contra-indications to inhalational induction (gastroesophageal reflux, myopathy, or familial history of malignant hyperthermia) and those with a history of unstable cardiac disease, neurological disease, obstructive airway disease, and recent acute respiratory illness/infection were excluded.The circuit was primed with 8% sevoflurane (Sevotroy 250, Troikaa Pharmaceuticals Ltd., Ahmedabad, India) in nitrous oxide and oxygen before the application of a mask to the patient’s face.Before anesthesia, subjects in the VCRII group were instructed on the vital capacity breath.4The concentration of gases used was 8% sevoflurane in nitrous oxide (66%) and oxygen (33%)at a flow rate of 8 L/min in both the groups.
In the VCRII group, the subject was asked to exhale forcefully, followed by a maximal inspiration via a face mask connected to the anesthetic circuit.The subject was then asked to hold his/her breath for the maximum time possible and then exhale residual volume.In the TV group, the subject was asked to continue quiet breathing through the facemask.The onset of induction of anesthesia was assessed as the time to the cessation of voluntary finger tapping, time to loss of eyelash reflex, time to return of regular breathing, and time to return of conjugate gaze.5Heart rate, peripheral oxygen saturation,systolic, and diastolic blood pressures were compared at baseline and 1-, 3-, 5-minute intervals from induction.The occurrence of stridor, cough, laryngospasm, hypoxemia, and excitatory movements was recorded.All patients received fentanyl 2 μg/kg (Verfen, Verve Pharma, India) 3 minutes before sevoflurane induction.Rescue remedy of intravenous propofol (Troypofol, Troikaa Pharmaceuticals Ltd.) at 2 mg/kg and succinylcholine (Sucol, Neon Pharma, Mumbai, India)100 mg was prepared for laryngospasm or desaturation.The trial was non-randomized.A trained nurse who was blinded to the group allocation was recording the outcome endpoints.Acceptance of anesthesia induction technique was assessed by the willingness to undergo a repeat procedure using the same method of induction.The trial flow chart showing the distribution of patients is given in Figure 1.
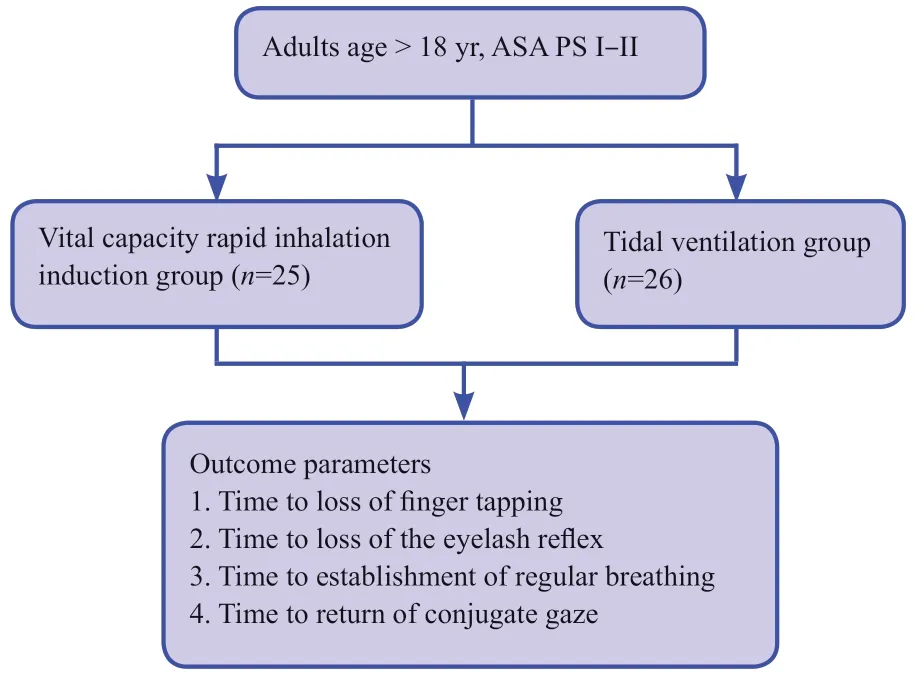
Figure 1:The flow chart.Note:ASA PS:American Society of Anesthesiologists physical status.
The sample size was calculated according to the results of Yurino et al.6A sample size of 23 in each group was calculated for a difference in onset of induction of 11 seconds for a power of 80% and an alpha of 0.01 using SPSS 23 software (IBM,Armonk, NY, USA).All results are expressed as the mean ±standard deviation (SD) or median (range; continuous variables) or as percentages of the group from which they were derived (categorical variables).Continuous variables were compared with the Student’st-test for normally distributed variables and the Mann-WhitneyUtest for non-normally distributed variables.Categorical variables were evaluated with the Chi-square analysis or two-tailed Fisher exact test.A value ofPless than 0.05 was considered significant.
RESULTS
Baseline characters of patients under vital capacity rapid inhalation and tidal ventilation induction with sevoflurane
A total of 51 patients were included in the study, 25 in the VCRII group and 26 in the TV group.The baseline parameters of both groups are depicted in Table 1.Age, sex, weight, and ASA status distributions, baseline heart rate, percutaneous oxygen saturation, systolic, and diastolic blood pressures were comparable between the two groups (P> 0.05).
Hemodynamic and respiratory outcomes of patients under vital capacity rapid inhalation and tidal ventilation induction
Induction was significantly faster in the VCRII group compared with the TV group.The time to loss of voluntary finger tapping (P< 0.001), time to loss of eyelash reflex (P< 0.001),time for the establishment of regular breathing (P< 0.001) and time to return of conjugate gaze (P= 0.046) were all significantly less in the VCRII group than those in the TV group.
To evaluate the cardiovascular effects of methods of induction, a comparison of vital signs was done between two groups before induction, and upon loss of consciousness.Heart rate in the VCRII group was significantly lower compared to the TV group at 3 minutes (P= 0.015) and 5 minutes postinduction (P= 0.012).Systolic and diastolic blood pressures were comparable between the two groups at all time points(P> 0.05; Table 2).
No adverse event (cough, laryngospasm, excitatory movements, hypoxemia) occurred in both groups.Patient willingness to return for repeat procedure using the same method of induction of anesthesia was 100% in both the groups.
DISCUSSION
In this study, the VCRII technique using 8% sevoflurane resulted in a faster induction of anesthesia, as estimated by time to loss of finger tapping, loss of the eyelash reflex, establishment of regular breathing, and return of conjugate gaze,compared with the TV technique.
The time for induction of anesthesia was taken as the time from the beginning of the administration of the agent to the loss of finger tapping which is an acceptable outcome in similar studies.7-9Though bispectral index monitoring was not done, clinical endpoints for recognition of induction like loss of finger tapping to verbal command are valid surrogates for bispectral index monitoring.10
The roadblock to wider acceptance of inhalational anesthesia is the longer time of induction compared to intravenous agents.11,12Modification of administration techniques facilitates the speed of induction.VCRII achieves a high alveolar concentration of sevoflurane in a shorter time resulting in smoother induction.Typically, this single-breath technique achieves the 2% alveolar sevoflurane concentration required to tolerate a surgical incision.2,13In a study by Lin et al.14the use of VCRII inhalational induction in 36 ASA physical status I–II patients resulted in an induction time of 60.6 ± 19.2 seconds which could be shortened to 48.3 ± 17.9 seconds with the use of fentanyl before induction.By contrast, our study employed fentanyl pre-induction in both the groups along with nitrous oxide and hence demonstrated faster induction times.In thepediatric population, the VCRII technique can produce faster induction as measured by loss of eyelash reflex, which has been preferred over tidal ventilation technique in 73 subjects over the age of 5 years in a randomized controlled trial comparing the two techniques.5This pediatric study used sevoflurane 7%in 50% nitrous oxide with oxygen at 6 L/min fresh gas flow along with midazolam premedication, while our study used sevoflurane 8% in 66% nitrous oxide with oxygen at 8 L/min fresh gas flow with fentanyl premedication, which may result in a comparable induction time in both the studies.Another pediatric study showed similar results with VCRII producing fewer adverse events, faster induction and better patient satisfaction compared with TV using 8% sevoflurane.15A similar study in adults using sevoflurane and nitrous oxide showed that VCRII, in comparison with stepwise tidal ventilation induction, resulted in an earlier loss of consciousness (54 ±10 secondsvs.108 ± 19 seconds) but was associated with a higher incidence of coughing.16This study used a lower concentration of sevoflurane at 4.5% which explains the longer induction times compared to our study.
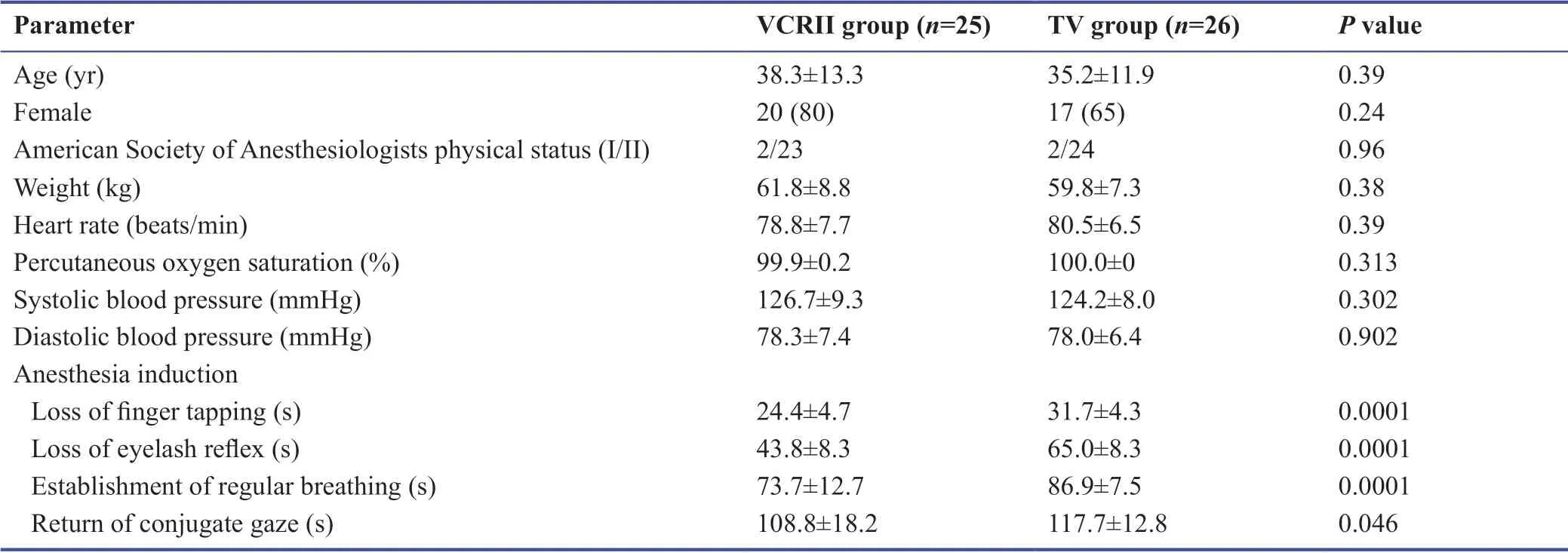
Table 1:Baseline characteristics of patients under VCRII and TV induction
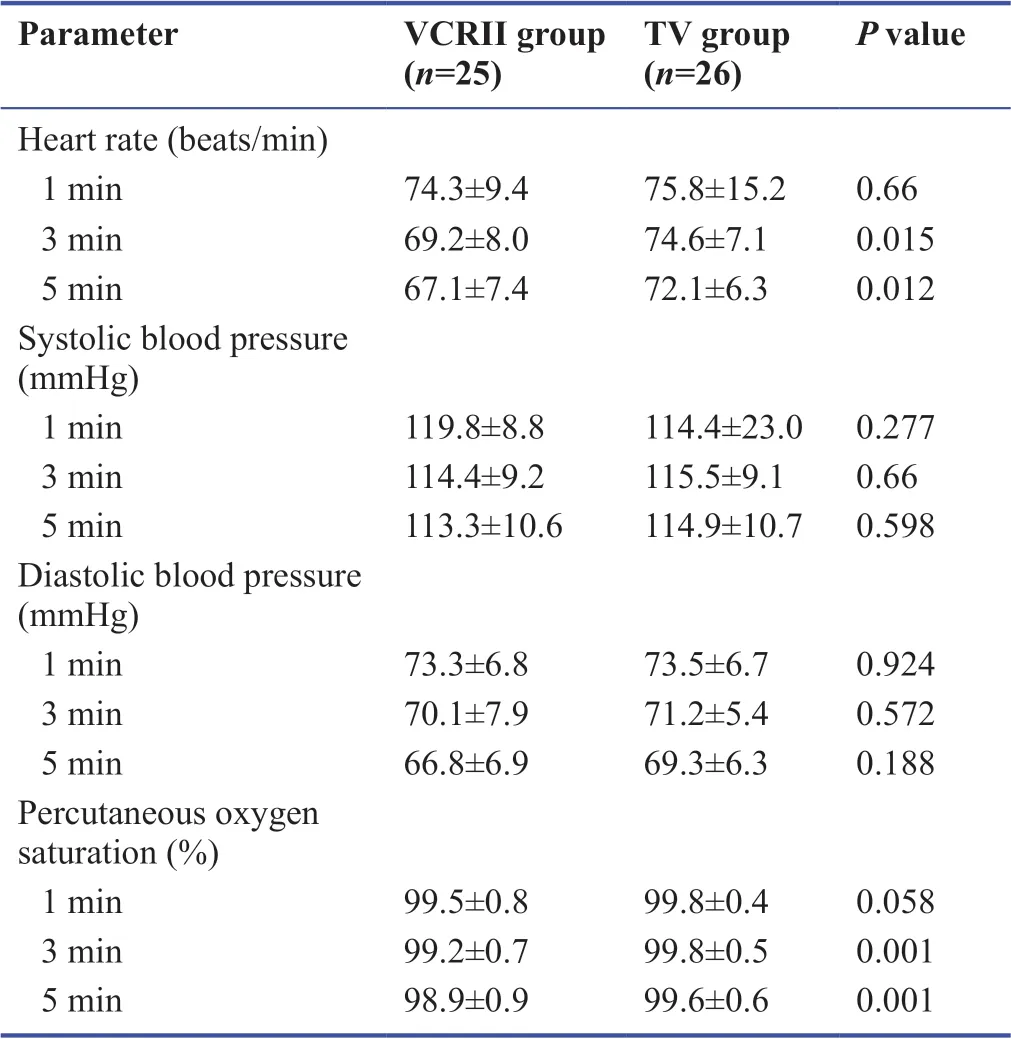
Table 2:Hemodynamic and respiratory parameters after induction of patients under VCRII and TV induction with sevoflurane
The present study shows that inhalational induction is a feasible and effective alternative to intravenous induction in Asian adults.There is emerging evidence that inhalational induction using sevoflurane has better hemodynamic stability, equal patient acceptance, and is cheaper than intravenous induction using propofol.7Usage of a single inhalational agent for induction and maintenance reduces adverse events accompanying the use of multiple intravenous agents, such as hemodynamic compromise.17
None of the patients in our study had coughing or laryngospasm.This indicates an adequate depth of anesthesia and suppression of airway reflexes.The VCRII technique requires some training but this is easily achieved in all our subjects.The feasibility of achieving adequate VCRII is 95% by 14 years of age as described in a previous study.18Besides, there was no difference in patient willingness to return for a repeat procedure under both the techniques, indicating that the VCRII technique was acceptable for the subjects.
The use of inhalational agents especially as maintenance of anesthesia is found to be feasible and cost-effective in ambulatory surgeries.19,20Our study also demonstrates the utility and safety of a faster induction technique using the same inhalational agent.
Our study has some limitations.This non-randomized study may be subject to bias.Although the VCRII technique produces a faster induction, this advantage remains small in clinical practice.In this study, intubation times or emergence times were incomparable between the two groups as we designed primarily for the comparison of induction characteristics of the two techniques.
VCRII rapid inhalational induction technique using 8%sevoflurane with nitrous oxide can result in a faster induction compared to the TV induction technique in adults.
Author contributions
Study design:JJC; patient selection:RV, JJC, RP, KM; data acquisition, statistical analysis and manuscript preparation:RV; data interpretation:RP, KM; manuscript revision:JJC, RP, KM.All authors have read and approved the final version of the manuscript.
None of the authors have any conflicts of interest.
Financial support
Nil.
Institutional review board statement
The study was approved by Institutional Ethics Committee, Amala Institute of Medical Sciences (approval No.AIMSIEC/07/2017) on July 1, 2017.
Declaration of patient consent
The authors certify that they have obtained patients’ consent forms.In the form, patients have given their consent for their clinical information to be reported in the journal.The patients understand that their names and initials not be published and due efforts will be made to conceal their identity.
Reporting statement
At the sight of it all the slaves fell upon their knees and hid their faces, and when it had three times flapped its mighty70 wings it uttered distinctly in Prince Vivien s own language the words: Prince, your only chance of happiness depends upon that which is most opposed to your own nature
The writing and editing of the study report were performed in accordance with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement.
Biostatistics statement
The statistical methods of this study were conducted and reviewed by the biostatistician of Amala Institute of Medical Sciences, India.
Copyright transfer agreement
The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement
Individual participant data that underlie the results reported in this article, after deidentification (text, tables, figures, and appendices)and anonymized trial data will be available on request.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
- Medical Gas Research的其它文章
- Ventilation with the noble gas argon in an in vivo model of idiopathic pulmonary arterial hypertension in rats
- Neuroprotective effect of helium after neonatal hypoxic ischemia:a narrative review
- Role of hydrogen in traumatic brain injury:a narrative review
- Efficacy of xenon anesthesia in preventing postoperative cognitive dysfunction after cardiac and major non-cardiac surgeries in elderly patients:a topical review
- Protective effects of hydrogen gas inhalation on radiation-induced bone marrow damage in cancer patients:a retrospective observational study
- Spontaneous breathing for managing analgesia during balanced anesthesia with remifentanil and desflurane:a prospective, single center randomized controlled trial