
A cross-sectional study on traditional Chinese medicine syndromes distribution for chronic atrophic gastritis based on data mining
2021-10-16 07:48:00ZeHuiChenLiXinMaYueWeiHaiXiaoHanEnLongXingJinXiangYang
Medical Data Mining 2021年3期
Ze-Hui Chen, Li-Xin Ma, Yue Wei, Hai-Xiao Han, En-Long Xing, Jin-Xiang Yang
A cross-sectional study on traditional Chinese medicine syndromes distribution for chronic atrophic gastritis based on data mining
Ze-Hui Chen1, Li-Xin Ma2, Yue Wei3 *, Hai-Xiao Han4, En-Long Xing5, Jin-Xiang Yang3
1Institute of Information on Traditional Chinese Medicine, Chinese Academy of Chinese Medical Sciences 100700, China.2Key Laboratory of Public Health Safety of Hebei Province, College of Public Health, Hebei University, Hebei 071002, China.3The Third Affiliated Hospital of Beijing University of Chinese Medicine, Beijing 100029, China.4Dongfang Hospital of Beijing University of Chinese Medicine, Beijing 100078, China.5Beijing Rehabilitation Hospital of Capital Medical University, Beijing 100144, China.
Chronic atrophic gastritis (CAG) is a common digestive system disease characterized by reduced gastric mucosa inherent glands and often accompanied by intestinal metaplasia and dysplasia. Traditional Chinese medicine believes that syndrome elements dampness and blood stasis are closely related to the occurrence and development of CAG and promote the occurrence of precancerous lesions of gastric cancer. However, there is a lacking of more in-depth and detailed study on the above syndrome elements. This study aimed to made a quantitative description by cross-sectional study on the frequency of key syndrome elements dampness and blood stasis of CAG.201 CAG patients who met with inclusion criteria were divided into 4 groups including: only dampness group, only blood stasis group, none of dampness and blood stasis group, dampness and blood stasis group according to their four diagnostic information. The severities and levels of patients’ clinical symptoms, pathological signs and patient-reported outcome scale used as evaluation indexes were collected. Data mining method of exploratory factor analysis was used for statistics.The results suggested that the frequencies of dampness and blood stasis were reflected in the severity and levels of gastric symptoms, helicobacter pylori infection and the distribution and severity of dysplasia. And blood stasis played a more prominent role in promoting the progression of the CAG to cancer.Our results might provide a quantitative syndrome description for the traditional Chinese medicine differentiation in treating precancerous lesions of gastric cancer and preventing gastric cancer.
Chronic atrophic gastritis, Precancerous lesions of gastric cancer, Traditional Chinese medicine syndrome, Data mining
Background
Chronic atrophic gastritis (CAG) is a common digestive system disease characterized by reduction of inherent glands in gastric mucosa, gastric atrophy (GA), or intestinal metaplasia (IM). It is often accompanied by non-specific symptoms such as upper abdominal fullness, pain, loss of appetite and belching [1]. At present, GA and IM are considered as precancerous lesions of gastric cancer (PLGC) with the risk of gastric cancer (GC). A systematic review revealed that the incidence rate of GC in patients with GA ranged from 0.53 to 15.24 per 1,000 person years, whereas there was more variation in GC incidence in patients with IM (0.38 to 17.08 per 1,000 person years) [2]. Prevention and treatment of high-grade dysplasia (Dys) and invasive GC are targets for patients with CAG or IM [3]. Clinical studies on the process of GA to GC had found that chronic inflammation can promote genetic and epigenetic abnormalities through a variety of pathogenic mechanisms. And treatments aiming at reducing the level of cancer-promoting inflammation has become one of the main strategies for the prevention and treatment of GC [4–5]. Therefore, active exploration of the prevention and treatment of CAG can effectively intervene the Dys and malignant transformation of GC, and is also a necessary way to block the occurrence of GC.
CAG has a long clinical course and lingering disease tendency. Due to lack of specific effective drugs, it is more difficult to cure CAG. However, traditional Chinese medicine (TCM) has advantages and efficacy on the treatment of CAG, which has been paid more and more attention. By further data mining to a large number of clinical cases and basic researches, more and more evidences have shown that TCM can alleviate the inflammatory reaction in GA, enhance the ability of anti-damage and repairment, and even reverse IM and Dys in the treatment of CAG [6].
TCM characterized for its holistic views and concepts based on “syndrome” (or Zheng in Chinese) differentiation, emphasizes the dynamic changes in the process of disease pathogenesis. “Syndrome” is a comprehensive conception and has inclusion of related pathological elements of location, etiology, disease potential and so on in a certain stage of a disease process. It reflects the essence of the disease and is also the basis for establishing the treatment prescription [7]. Since “syndrome” reflects a comprehensive pathogenicity of different disease stage, differentiation of syndromes plays an important role to the therapeutic treatment. A large number of clinical studies have shown that the pathogenesis of CAG is asthenia in origin Qi and excess in pathological damage, that is to say, the weakness of “spleen Qi” (function to transport and digest) mixed with other pathological damages such as “dampness” (pathological fluid), blood stasis in the stomach tissue, “Qi stagnation” (stagnation of the circulation of vital energy) and “heat” (leading to redness, swollen and inflammation) [8–11]. These pathogenesis syndrome elements of CAG have been received attention recently and recognized as key link in the prevention and treatment of PLGC and GC. Previous studies have found that sputum, dampness and blood stasis are closely related to the occurrence and development of PLGC, and are important syndrome elements to promote the occurrence of PLGC [12–16]. However, there is a lack of transparent and detailed study on the above syndrome elements, including the assessment of degree of its symptoms, gastroscopy or pathological signs, the related signs to identify the pathological stage and effectiveness after syndrome differentiation and treatment. Based on this we conduct a cross sectional study to explain the key role of syndrome elements such as dampness and blood stasis in CAG development.
Furthermore, these TCM syndrome elements are the outcome and goal of clinical four-diagnosis information and will be extracted. In addition to establishing a unified judgment standard, seeking scientific research methods to improve the objectivity and credibility of research results, we use unsupervised data mining strategies, method of machine learning, and statistics of database system intersection to reveal the relationships in large data sets. These data mining process enables us to better understand the relationships between variables and to predict the corresponding subsystem data behavior [17]. The literature research shows that data mining has been widely used in TCM syndrome research [18–20]. Under premise of no prior assumptions (such as the gold standard for syndrome element determination), the software self-analysis can directly classify and sort out the sample data with similar characteristics from a large amount of clinical information, explore the association and characteristics among various variables, and dig out the potential rules [21]. Therefore, based on the clinical collection of the four diagnostic information of CAG patients, this study intends to apply the exploratory factor analysis (EFA) method, methods of data mining, to conduct data processing, and detect the syndrome characteristics through multicollinearity elimination and dimension reduction, so as to realize the induction and determination of the syndrome element types of CAG.
Materials and methods
Study population
This cross-sectional study was conducted in 2 medical centers in China, including Beijing University of Chinese Medicine Third Affiliated Hospital and Dong fang Hospital Affiliated to Beijing University of Chinese Medicine. The study began in September 2017 and ended in October 2019 based on participant survey. Patients in 18–85 years old, who met diagnostic criteria of CAG with gastroscope and pathological report to the out-patient department of the aforementioned hospital and signed informed consent were recruited.
Ascertainment of CAG
Diagnostic criteria of CAG were based on the consensus opinions presented at the[22].
Criteria for Inclusion and Exclusion of cases
Inclusion criteria. Met CAG diagnostic criteria with detailed medical records and diagnostic reports; over 18 years of age; consented and volunteered to participate in the study.
Exclusion criteria. Cases that did not meet the inclusion criteria and were mistakenly included; incomplete pathologic report information; fail to answer or fill in survey questionnaire as required by the study.
Survey questionnaire: clinical observation form and patient-reported outcome scale
Clinical observation form was designed based on literature research, expert advice, and clinical guidelines [22–25]. Clinical observation form content included general information (name, age, gender), medical information (symptoms, signs, course of disease, past and family history, TCM tongue and pulse), auxiliary examinations (pathology and gastroscopy report), modern medicine diagnosis. Clinical symptoms contained cardinal symptoms (CS) and secondary symptoms. The CS were evaluated in terms of frequency (none, occasional, sometimes, most of the time, constantly all day) and severity (none, mild, moderate, and severe) respectively, while the secondary symptoms were evaluated in terms of frequency. According to the pathological report, gastric mucosal pathology was divided into six categories: chronic inflammation, GA, IM, activity, helicobacter pylori (Hp) infection, and Dys.
The CAG patient-reported outcome (PRO) scale was developed based on the TCM PRO scale for spleen and stomach diseases to self-evaluate items for patients. These items was generally divided into four modules: physiological field (PHF), independent field (IF), psychological field (PSF) and social environment field (SEF) [26–27]. 30 selected items assessed by patients themselves to comprehensively reflect the quality of life of CAG patients. Scores were counted according to frequencies of item or severity (Figure 1).
Survey methods and quality control
We performed a cross-sectional study to collect clinical data from patients who met the diagnostic criteria for CAG. Patients’ informed consents were obtained and collected before they were included in the study. Data were collected and statistics methods were used in data analysis. To reduce the measurement bias, prior to the initiation of clinical research, all the investigators in this study were trained in accordance with standard operating procedures. Duties of investigators were defined in the clinical research program, and should be supervised and guided by at least two or more deputy senior experts. Clinical epidemiologic inquiries and measurements for each patients was conducted by at least two resident physicians or graduate students at the same time to ensure the authenticity and reliability of the data collecting and recording.
Data analysis
We assigned corresponding values to the answers of each item in the clinical observation form questionnaire. The severities of the CS was scored as follows: none = 0, mild = 2, moderate = 4, severe = 6, and the scores of frequencies were divided by: none = 0, occasionally = 2, sometimes = 4, most of the time = 6, and constantly all day = 8. The frequencies of secondary symptoms (SS) were scored by 0 for no and 2 for yes. The grading criteria and scoring methods of pathological conditions for chronic inflammation, GA and IM were divided by: none = 0, mild = 2, moderate = 4, severe = 6.

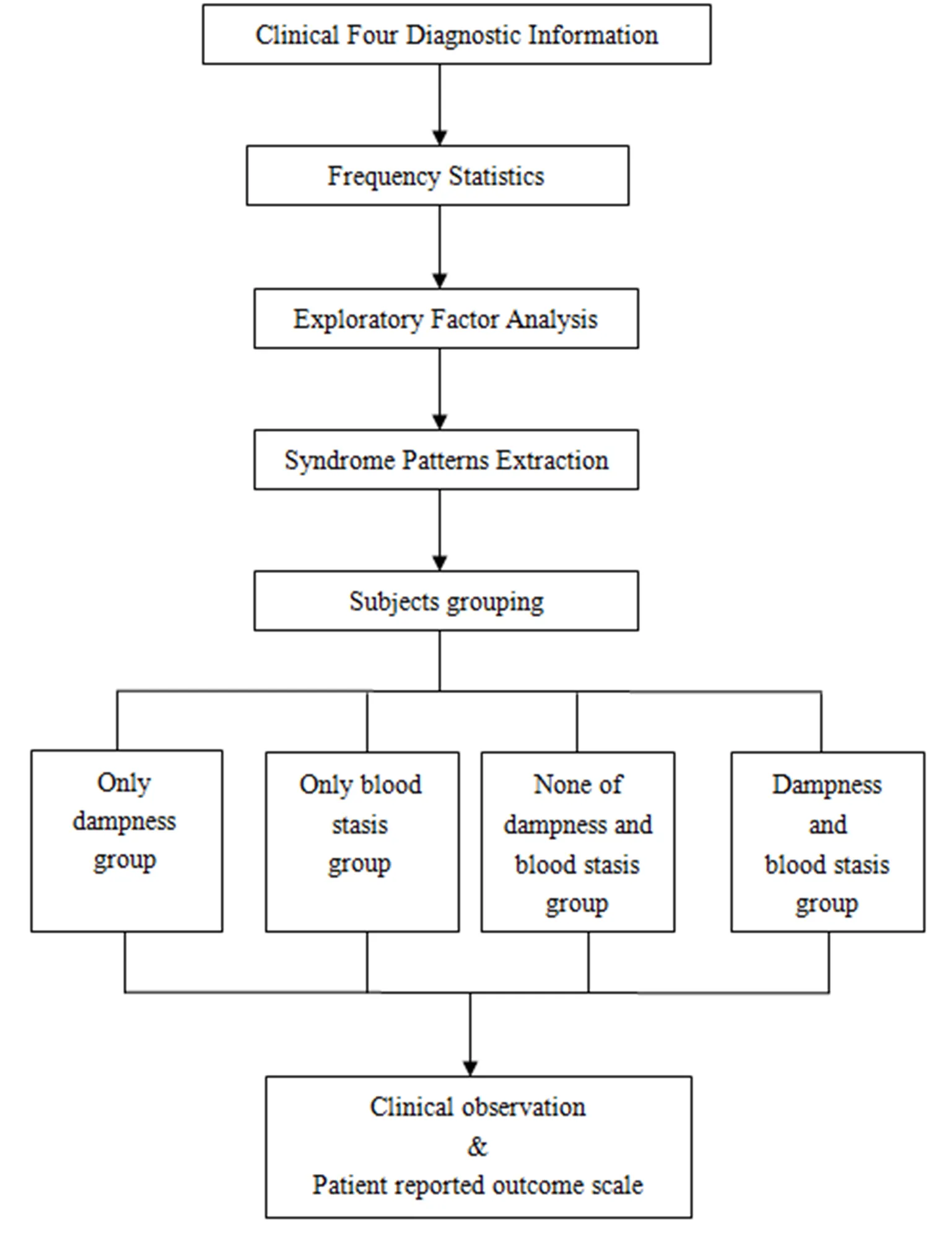
Figure 1 Flow diagram of clinical research
Results
Characteristics of participants
In this study, 210 cases of clinical information were collected, 9 cases were eliminated according to the exclusion criteria, and 201 qualified cases were finally included in this study, with a 95.7% qualified questionnaires. There were 81 males and 120 females with a sex ratio of 1:1.48. The youngest was 31 years old, the oldest was 84 years old, and the average age was 60.78 ± 10.90 years old. All the variables of four diagnostic detected were pre-analyzed, and 44 variables of which with more than 20% frequency of occurrence were chosen for subsequent analysis. These variables were then listed in sequence in order of the frequency of distribution (Table 1).
Extraction of TCM syndrome elements based on EFA
Before analysis, the Kaiser-Meyer-Olkin test and Bartlett’s test of sphericity were used to determine whether the data met the EFA analysis requirements. Principal component analysis was then performed to extract common factors from the original variables. Based on literature research and present diagnostic criteria of TCM syndrome elements [28–29], the diagnostic variables and nature of disease obtained from the four diagnostic information were ultimately assigned to 15 common factors. Based on the above EFA results, the same syndrome elements were summarized and combined, and the 7 syndrome elements finally obtained were as follow: �1) Qi deficiency; �2) dampness; �3) heat; �4) blood stasis; �5) Qi stagnation; (6) Yang deficiency; (7) Yin deficiency (Table 2 and Table 3).
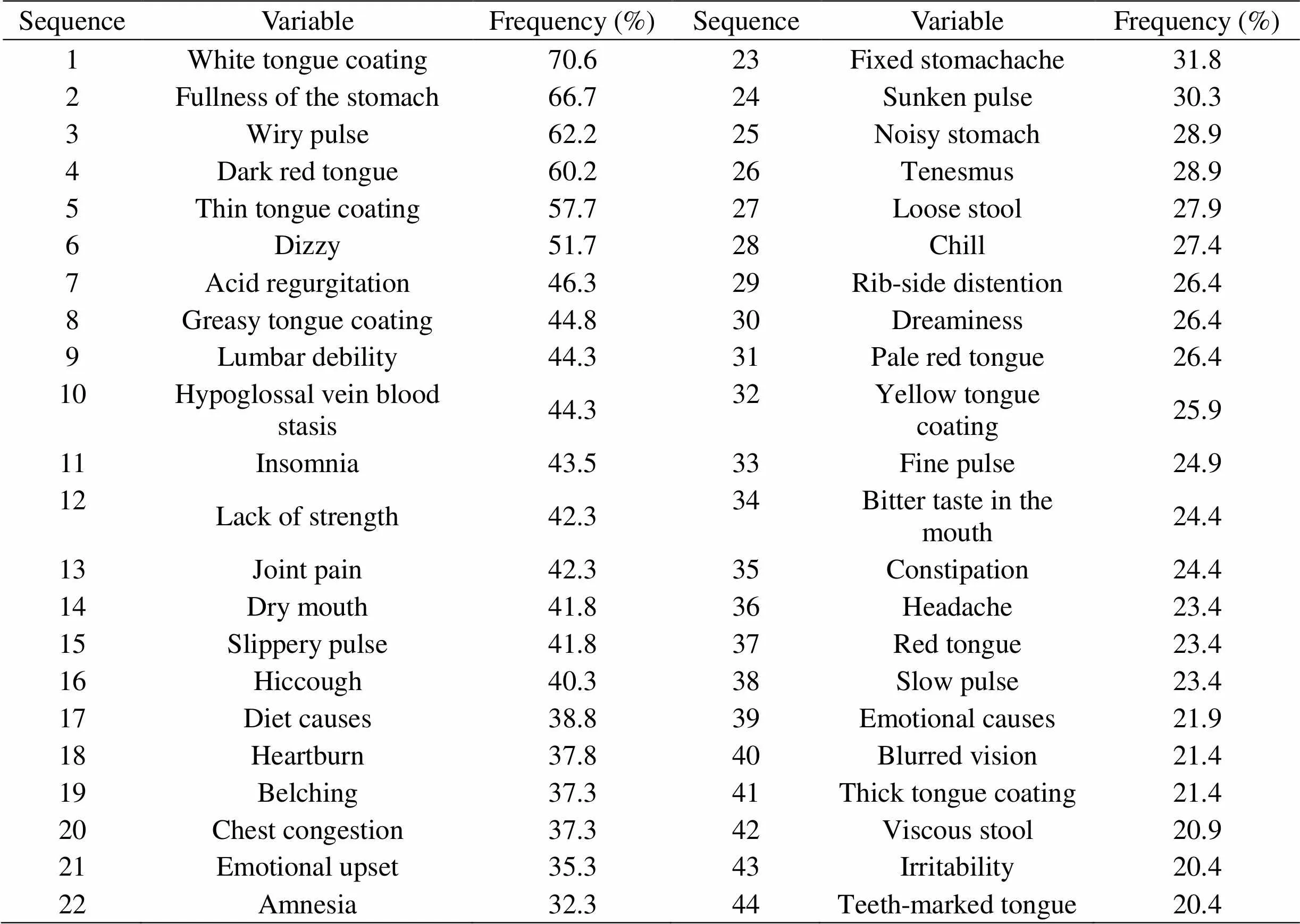
Table 1 Frequency of variables of four diagnostic for patients with CAG (N=201)
Note: CAG, chronic atrophic gastritis.
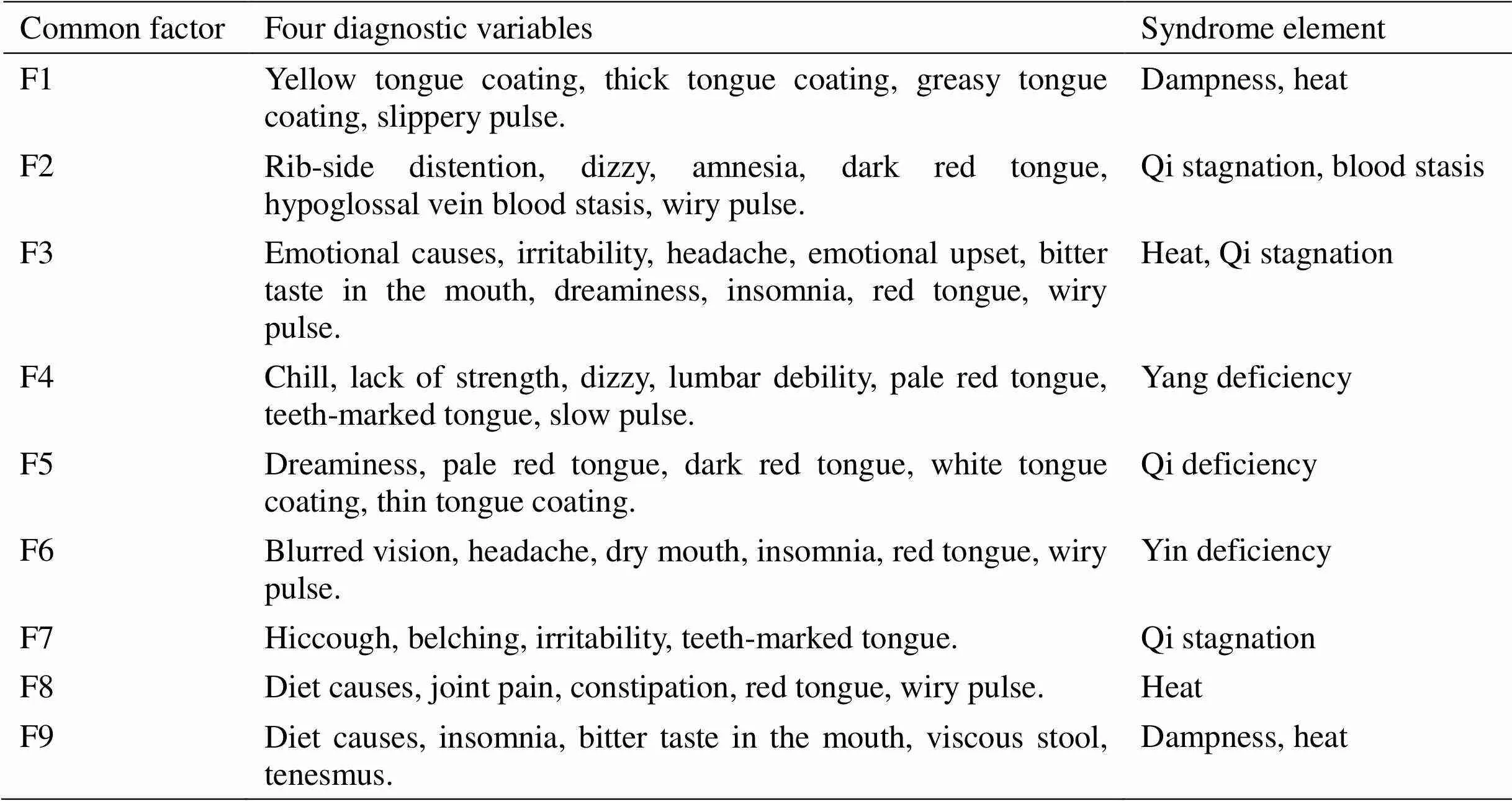
Table 2 EFA based common factor extraction and their corresponding four diagnostic variables and disease nature
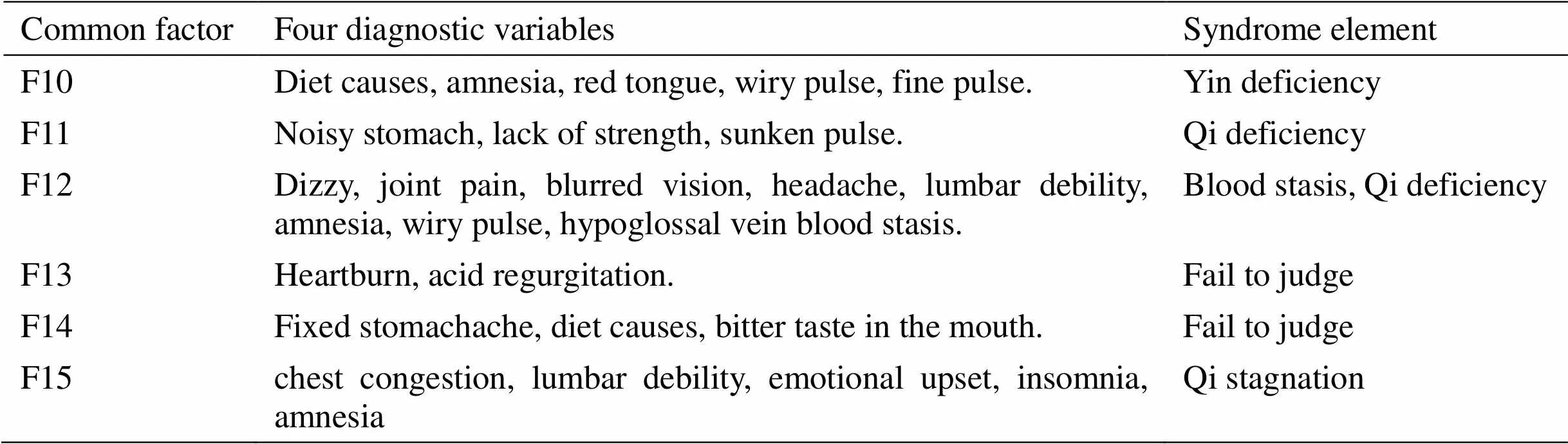
Table 2 EFA based common factor extraction and their corresponding four diagnostic variables and disease nature (Continued)
Note: EFA, exploratory factor analysis.
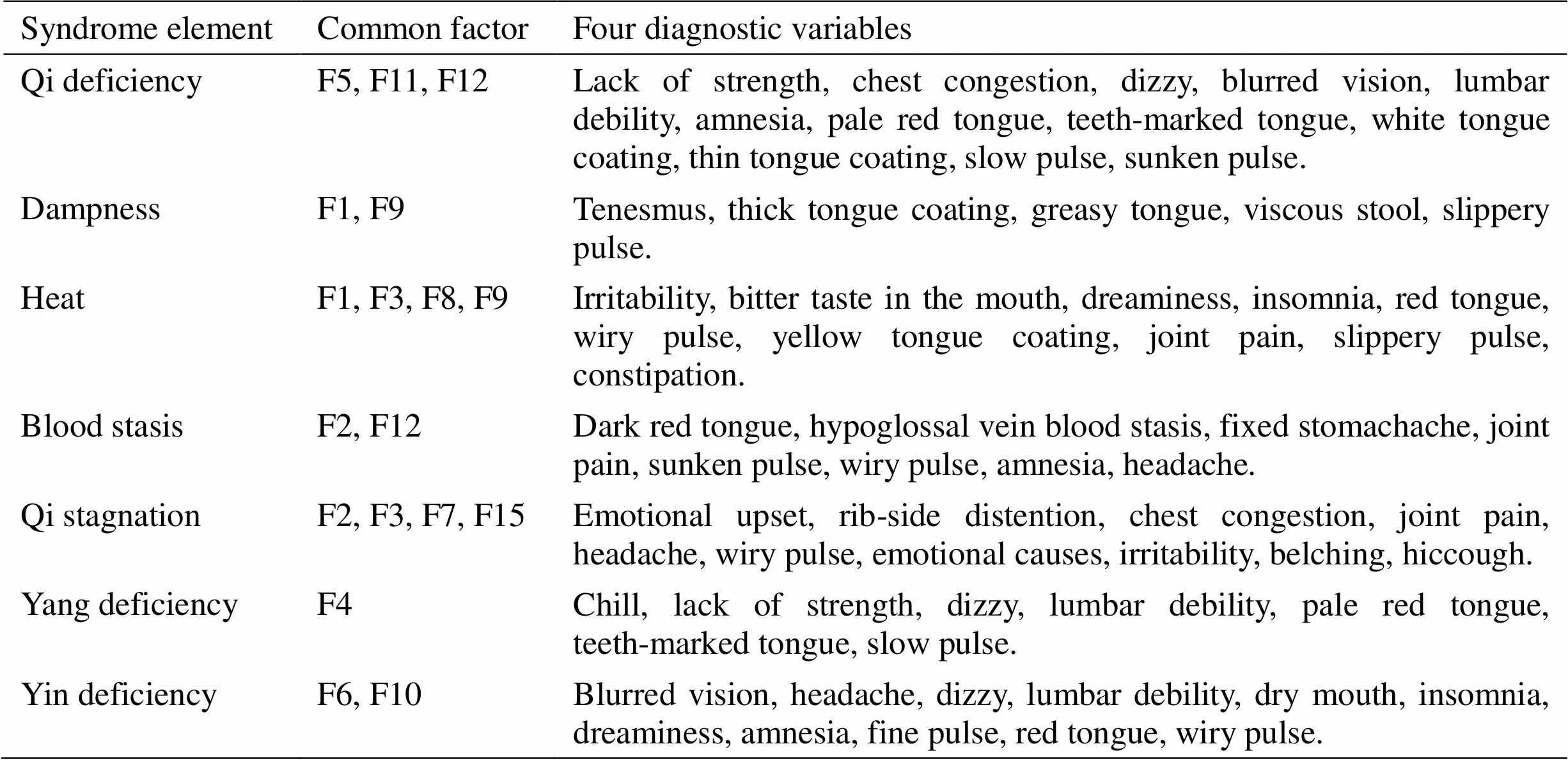
Table 3 Summary table of syndrome elements and information of four diagnostic variables after common factors combination
Relationship between TCM syndrome elements and clinic pathological features in CAG patients
According to the EFA factor score, the score of each patient in each common factor can be obtained, and the common factors scoring > 1 were selected to judge all the syndrome elements possessed by each patient based on Table 2 and Table 3. 201 Patients were divided into four groups according to whether there were dampness and blood stasis in the syndrome elements determined by EFA. The four groups were: (1) only dampness group (ODG); (2) only blood stasis group (OBSG); �3) none of dampness and blood stasis group (NDBSG); �4) dampness and blood stasis group (DBSG). Pearson chi-square test showed that there were statistically significant differences between four syndrome element types and Hp and Dys (< 0.05), whereas other data had no significant difference (> 0.05), as shown in Table 4 and Figure 2.
Relationship between TCM syndrome elements and scale score in CAG patients
Pathological severity score. Kruskal-Waillis rank sum test showed that there were statistically significant differences between four syndrome element types and Hp score and total score (< 0.05), whereas other data had no significant difference (> 0.05), as shown in Table 5. Comparison of the score on the same pathology variable between the two groups showed that there were significantly statistical differences between NDBSG and ODG in IM score, OBSG and NDBSG and ODG in CI score, NDBSG and OBSG and ODG in Hp score, OBSG and NDBSG and ODG in Dys score, OBSG and NDBSG and ODG and DBSG in total score (< 0.05).
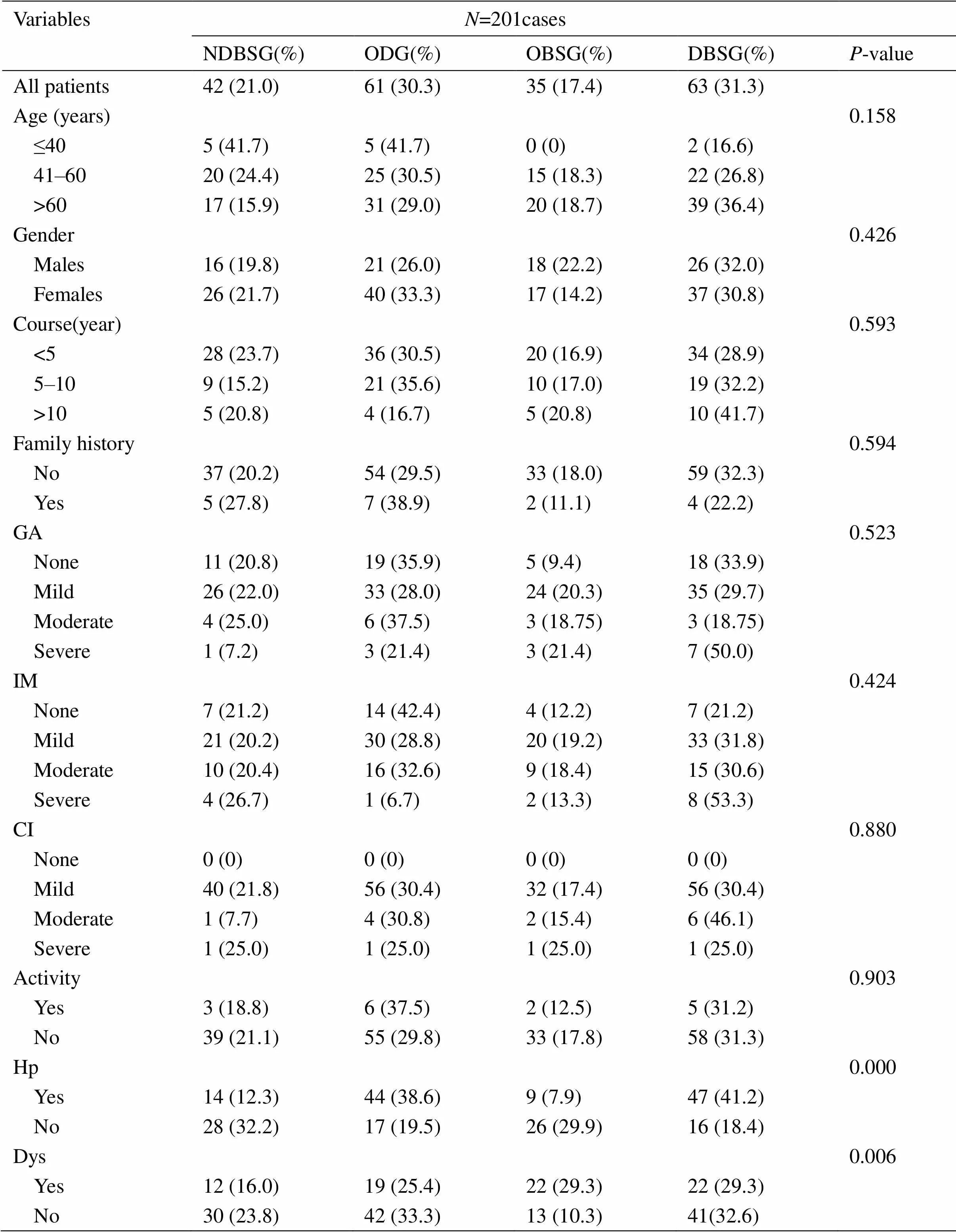
Table 4 Descriptive characteristics of different syndrome element groups
Note: NDBSG, none of dampness and blood stasis group; DBSG, dampness and blood stasis group; OBSG, only blood stasis group; ODG, only dampness group; GA, gastric atrophy; IM, intestinal metaplasia; CI, chronic inflammation; Hp, helicobacter pylori; Dys, dysplasia.
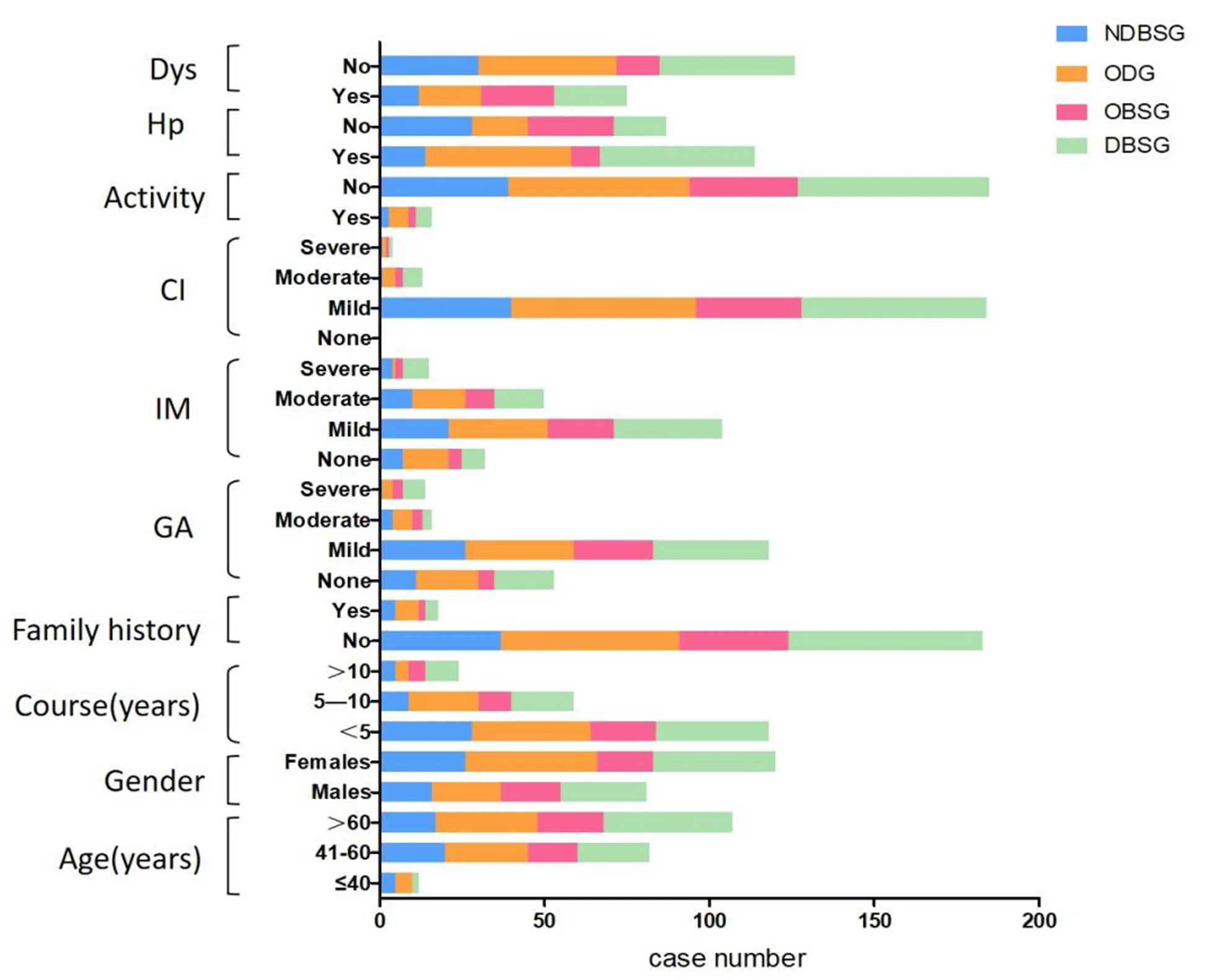
Figure 2 Distribution of factors in different syndromes element groups. NDBSG, none of dampness and blood stasis group; DBSG, dampness and blood stasis group; OBSG, only blood stasis group; ODG, only dampness group; GA, gastric atrophy; IM, intestinal metaplasia; CI, chronic inflammation; Hp, helicobacter pylori; Dys, dysplasia.
Table 5 Pathological severity score of different syndrome element groups ()
Note: compared with NDBSG,◆< 0.05; compared with ODG,▲< 0.05; compared with OBSG,△< 0.05. NDBSG, none of dampness and blood stasis group; DBSG, dampness and blood stasis group; OBSG, only blood stasis group; ODG, only dampness group; GA, gastric atrophy; IM, intestinal metaplasia; CI, chronic inflammation; Hp, helicobacter pylori; Dys, dysplasia.
Symptom severity score. Kruskal-Waillis rank sum test showed that there were significant differences between four syndrome element types and CS score and total score (< 0.05), whereas other data had no statistically significant difference (> 0.05), as shown in Table 6. Comparison of the score on the same variable between the two groups showed that there were statistically significant differences between DBSG and NDBSG and ODG in CS score, DBSG and NDBSG and ODG in total score (< 0.05).
Table 6 Symptom severity score of different syndrome element groups ()
Note: compared with NDBSG,◆< 0.05; compared with ODG,▲< 0.05. NDBSG, none of dampness and blood stasis group; DBSG, dampness and blood stasis group; OBSG, only blood stasis group; ODG, only dampness group; CS, cardinal symptoms; SS, secondary symptoms.
PRO scale score. Kruskal-Waillis rank sum test showed that there were statistically significant differences between four syndrome element types and PHF score and total score (< 0.05), whereas other data had no statistically significant difference (> 0.05), as shown in Table 7. Comparison of the score on the same variable between the two groups showed that there were statistically significant differences between NDBSG and OBSG and DBSG in PHF score, NDBSG and OBSG and DBSG in total score (< 0.05).
Table 7 PRO scale score of different syndrome element groups ()
Note: compared with NDBSG,◆< 0.05. PRO, patient-reported outcome; NDBSG, none of dampness and blood stasis group; DBSG, dampness and blood stasis group; OBSG, only blood stasis group; ODG, only dampness group; PHF, physiological field; IF, independent field; PSF, psychological field; SEF, social environment field.
Appearance of syndrome elements dampness and blood stasis in different stages of CAG
Referring to the currently widely accepted Correa model [30], the progression stage of CAG was divided into three stages: GA, IM and Dys. The pathological results showed that only the CA was the atrophy stage, accompanied by IM but no Dys was the IM stage, and accompanied by Dys was the Dys stage. Pearson chi-square test showed that there were statistically significant differences in the distribution of cases in different groups at different stages of disease (< 0.05), as shown in Table 8 and Figure 3.
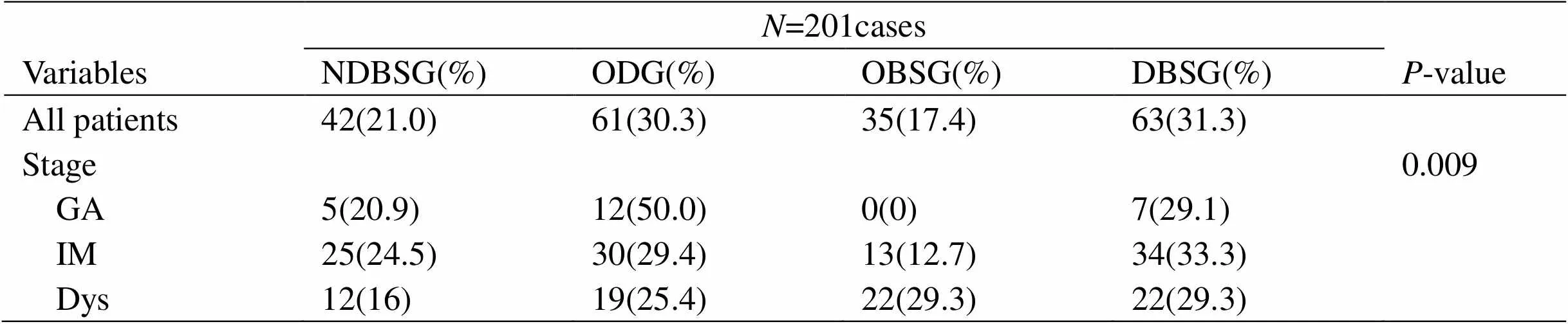
Table 8 Proportion of different syndrome element groups in different stages of CAG
Note: CAG, chronic atrophic gastritis; NDBSG, none of dampness and blood stasis group; DBSG, dampness and blood stasis group; OBSG, only blood stasis group; ODG, only dampness group; GA, gastric atrophy; IM, intestinal metaplasia; Dys, dysplasia.
Discussion
TCM syndrome differentiation focus on and summarizes the internal potential rules by observing the external symptoms and signs and summarizing the closely related symptoms and symptoms, symptoms and signs. The syndrome elements generated in this processarethesmallestandmostbasicunitsthat directlyreflecttheinternalpathogenesisfromthe observable external signs. Syndrome elements reflect the disease nature which are the essence of disease complexity through diversification [31]. Therefore, the characteristics of the syndrome elements, such as fuzziness, nonlinearity and concealment, can not be found through the simple data analysis of linearity. Data mining method, however, can be extracted from huge amounts of information and the unknown of potential features, more objectively revealing the universal law of syndrome differentiation and predict the development trend of disease. It conforms to the main goal of TCM treatment based on syndrome differentiation, and is close to the holistic concept of TCM from the outward appearance to the inner part and grasping the essence from the phenomenon in methodology, making TCM’s grasp of the essence of disease more specific and operable. In addition to the above, some researchers believe that the unsupervised data analysis process do not need to refer to prior knowledge to automatically complete the calculation, so it make up for the lack of a unified and recognized gold standard to determine the syndrome elements, which has a certain advantage over the supervised data analysis [21]. EFA, as one of the unsupervised data mining method, uses dimensionless correlation analysis to investigate the covariance or correlation coefficient matrix of variables, and to explain the correlation between variables (observable explicit variables, i.e., four-diagnostic information) and a few common factors (unobservable latent variables, i.e., syndrome elements). In this study, factor analysis was used to integrate the information items of the four diagnoses and convert them into syndrome elements.
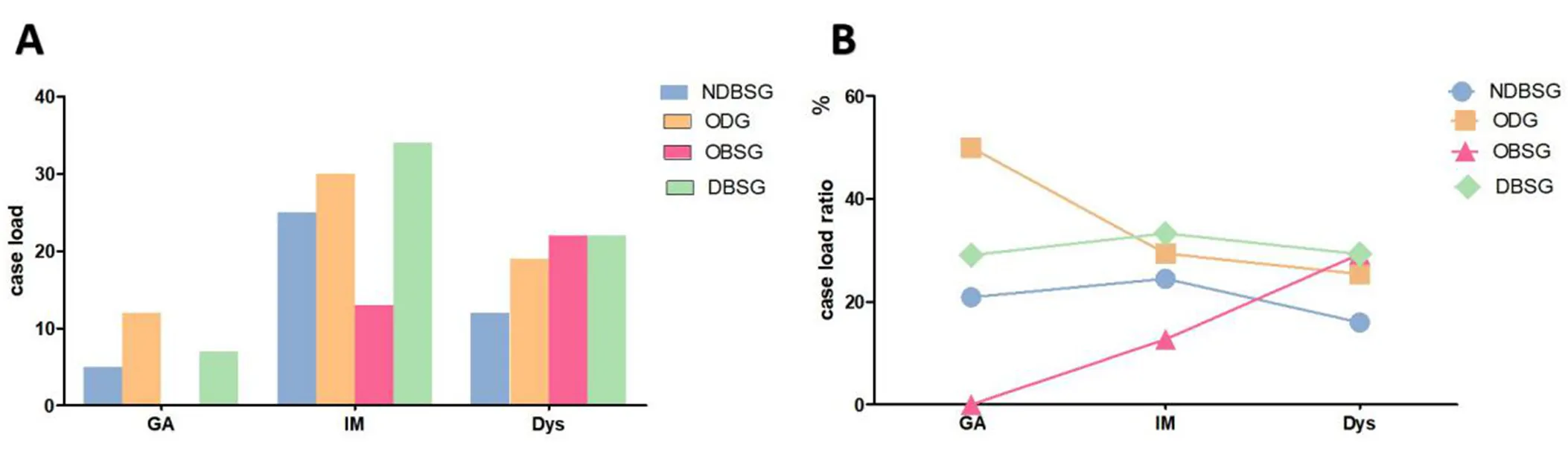
Figure 3 Proportion of each groups in different stages of CAG. NDBSG, none of dampness and blood stasis group; DBSG, dampness and blood stasis group; OBSG, only blood stasis group; ODG, only dampness group; CAG, chronic atrophic gastritis.
In the evaluation of the degree of symptoms, the score of DBSG was the highest, and there was a statistical difference with the NDBSG and the ODG (< 0.05), but no statistical difference was found with the OBSG, suggesting that CAG patients with both dampness and blood stasis syndrome elements may have more serious clinical symptoms (significant stomach symptoms).In addition, compared with the influence of the syndrome element dampness, blood stasis plays a more prominent role in the symptom manifestation. Blood stasis is one of the most common pathological factors after a long illness. With the development of the disease, both Qi stagnation and Qi deficiency can result in blood damage, and Qi-blood disharmony can lead to Qi stagnation and blood stasis, which is closely and positively correlated with the disease progression. The experiment showed that the CAG model rats with a model cycle of 16 weeks saw the first symptom of Qi deficiency in the fifth week, the symptoms of blood stasis appeared after the 13th week, and the signs of blood stasis were significant until the 16th week [32], suggesting that blood stasis was an important pathological reflection in the later stage of the disease. Therefore, it is speculated that the degree of gastric symptoms may gradually increase with the progression of the disease. In addition, modern medicine believes that blood stasis is closely related to the gastric mucosa microcirculation blood anoxic. Gastric mucosa microcirculation disorder associated with ischemic hypoxia can lead to the continuous aggravation of CAG course, and the decrease of effective blood flow of gastric mucosal microvessels can directly affect the metabolism of substances in the mucosal epithelium, leading to the injury of gastric mucosal defense system, thus increasing the probability of gastric mucosal injury caused by various pathogenic factors [33], which may be one of the causes of obvious or aggravating gastric symptoms. According to TCM, Qi-blood disharmony and Qi movement disorder are the important etiology and pathogenesis of stomach symptoms, such as stomachache, fullness of the stomach, noisy stomach, etc. Blood stasis impeding the movement of Qi and blood is often manifested as general pain, and the pain has a definite place. In this study, it was found that patients had common stomach distention pain, most of which showed definite pain, reflecting the pathogenesis characteristics of Qi-blood disharmony and Qi stagnation and blood stasis. The more blood stasis, the more Qi block, clinical symptoms were more prominent. The effect of dampness is weaker than that of blood stasis, which is speculated to be due to its direct effect on Qi block, which can promote the formation of blood stasis, namely Qi disease affecting the blood. Blood stasis may be a direct factor affecting the clinical symptoms. Therefore, the presence of the syndrome element blood stasis increases the degree of clinical symptoms. Blood stasis occurs in blood aspect which may be a direct factor affecting clinical symptoms. Therefore, the presence of the syndrome element blood stasis increases the level of clinical symptoms.
PRO scale was used to evaluate the effect of CAG patients' overall quality of life. The results showed that there were statistically significant differences between the NDBSG,ODG and DBSG in terms of PHF and total PRO score (< 0.05). The PHF reflects the severity of clinical symptoms of the patients, which is basically consistent with the effect of blood stasis on the severity of symptoms in the clinical observation form. However, there were no statistically significant differences among groups in PSF, IF, SEF and quality of life score, indicating that the differences in syndrome factors had a low impact on the above fields. It showed that the effect of this disease on psychology, independence and social environment is relatively balanced. It showed that the effect of this disease on psychology, independence and social environment was relatively balanced. At the same time, the influence intensity of the above three fields on CAG patients was low. Some researchers speculate the reason is that the patients are mainly aged, and most of them have retired from the work environment to bear the reduction of social and life pressure. Therefore, the effect of the disease on social function is not significant [16]. However, relevant studies have shown that CAG patients have a variety of psychological troubles. For example, depression is relatively common in CAG patients, and interpersonal sensitivity is positively correlated with depression and regulated by coping styles [34–35]. It is still necessary to make further exploration on whether the majority of elderly patients will gradually weaken interpersonal sensitivity and reduce the occurrence of psychological problems after leaving the social work environment. Since CAG patients are not limited to the elderly population, stratification analysis carried out by age groups, psychological factors such as anxiety and depression disorders will make the treatment effect of CAG in terms of the psychological and social functions more convincing.
According to the distribution of pathological changes, GA, IM, CI and activity showed no statistical difference among the syndrome element groups. The distribution of syndrome elements in Hp and Dys had obvious tendency. Hp infection was mostly concentrated in patients with syndrome elements dampness. The blood stasis group was more prone to Dys, which was correlated with the existence of Dys.
In terms of Hp infection, a number of previous studies have shown that syndrome of dampness-heat are highly correlated with Hp infection [23–25]. Hp, as a toxic pathogen, invaded gastric mucosa and resulted in obstruction of Qi and blood circulation. Dampness-heat may provide objective conditions for Hp to colonize gastric mucosa and cause disease. Some researchers speculated that one of the important microscopic factors for the formation of dampness-heat of spleen and stomach was that granulocyte-macrophage colony-stimulating factor and regulated upon activation normal T cell expressed and secreted factor, effecters related to gastric mucosa protection and inflammatory response, were directly or indirectly involved in Hp infection [26]. The results of this study suggested the prevalence of dampness in Hp infection in CAG patients. Dampness has the characteristics of stickiness and lingering, which is similar to Hp infection that is easy to be repeated and difficult to eradicate. The occurrence of dampness is closely related to the rich and thick diet and the dysfunction of spleen-transportation. Moreover, evidence shows that high-fat diet causes gastric microflora imbalance, and the change of microflora is accompanied by the increase of gastric leptin, which leads to the occurrence of PLGC [36]. In addition, the presence of blood stasis increases the probability of the occurrence of Dys, which is the result of pathogenic toxins in TCM theory [24]. Toxin is a comprehensive pathogenic factor that causes serious injury to human body by accumulation of various pathological products. Both toxin and blood stasis, as pathological metabolites at the end stage of disease, can be transformed by other pathological factors and often exist in combination. Some researchers believe that Qi deficiency and toxin-blood stasis is the basic pathogenesis of the occurrence and development of malignant tumors [27]. Therefore, the gradual formation of blood stasis may lead to the occurrence of Dys, an important PLGC, and even carcinogenesis.
Further analysis of the effect of syndrome elements dampness and blood stasis on the severity of pathological changes showed that blood stasis had a relatively large effect on the severity of pathology in general. The results of this study suggested that blood stasis not only had a certain concentration in the distribution of Dys, but also had an important influence on the severity of pathological changes, mainly reflecting in CI, Hp infection and Dys. Evidence shows that abnormal changes of microscopic indicators related to blood stasis affect the occurrence and development of PLGC [37], and Dys is currently the most recognized PLGC [38]. Therefore, this study speculated that blood stasis had a particularly critical impact on the severity of precancerous lesions of gastric cancer. In addition, there is a close correlation between inflammation and blood stasis. Inflammatory factors can induce vascular endothelial injury, microcirculation disorder, change of blood flow rheology, local stasis and thrombosis. Emotional disorder and stress state are the inducement of inflammation, and also one of the causes of Qi stagnation and blood stasis [39]. The results showed that the severity of CI was relatively high in the OBSG, which may be related to the above reasons.
CAG is a long course of disease, and there may be carcinogenesis progression under non-intervention conditions. According to the currently recognized Correa model [30], it can be seen that the pathological evolution characteristics of each stage have certain regularity. In the initial stage, GA is the dominant factor, and after IM and Dys, the tendency of cancerization is increased. Based on the above theories, this study further analyzed whether the syndrome elements dampness and blood stasis were related to the CAG development process. The results indicated that the occurrence of CAG in different stages of each group was different. Among them, the proportion of OBSG increased significantly with the progress of the disease, while ODG showed a downward trend, while NDBSG and DBSG remained basically stable, suggesting that there might be a trend of the transformation of syndrome elements from dampness to blood stasis in the development of the disease, which was basically consistent with the views of relevant scholars before [40]. In addition, literature studies on big data specifically pointed out that Yin deficiency was more common in the GA of gastric mucosa, heat and dampness was more common in the GA and IM period, and blood stasis and Yang deficiency were more common in the Dys stage [41]. Eating disorders, spleen deficient or exogenous damp-toxin invasion (Hp infection) may result in an apparent symptoms of dampness in the early stages of the disease. As the disease progresses, the dampness blocks Qi, affecting blood circulation, and blood stasis gradually appears. Due to the accumulation of various pathological factors, the blood stasis and toxin becomes more and more prominent. This reflects the pathogenesis transformation of CAG from dampness to blood stasis and toxin, and provides theoretical basis for the important role of clearing damp, activating blood circulation and detoxication method in blocking the PLGC.
Conclusions
Unsupervised data mining represented by EFA is an important method to discover the hidden law of multi-dimensional and multi-linear TCM syndrome elements, revealing that CAG syndrome elements mainly include Qi deficiency, dampness, heat, blood stasis, Qi stagnation, Yin deficiency and Yang deficiency. The in-depth study of the syndrome elements dampness and blood stasis proves that they are critical in the development of CAG, mainly reflected in the severity of gastric symptoms, Hp infection and the distribution and severity of Dys, and blood stasis plays a particularly prominent role in promoting PLGC. In the later stage of CAG course, especially in the PLGC stage, prolonged illness can damage Qi, leading to the combination of Qi deficiency with toxic- blood stasis, which are the key factors to induce CA. We concluded that the core pathogenesis of PLGC might start with Qi deficiency and further caused by toxic-blood stasis. Establishment of a principle based on syndrome differentiation of supplementing Qi, removing blood stasis and detoxifying toxin for the treatment of PLGC, will provide a promise for its clinical effectiveness in reversing PLGC and preventing GA.
1. Fang JY, Du YQ, Liu WZ, et al. Consensus on chronic gastritis in China (Shanghai, 2017).. 2017;22(11):670–687.
2. Spence AD, Cardwell CR, McMenamin úC, et al. Adenocarcinoma risk in gastric atrophy and intestinal metaplasia: a systematic review.. 2017;17(1):157.
3. Pimentel-Nunes P,Libanio D,Marcos-Pinto R, et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019.. 2019;51(4):365–388.
4. Piazuelo MB, Riechelmann RP, Wilson KT, et al. Resolution of gastric cancer-promoting inflammation: anovel strategy for anti-cancer therapy.. 2019;421: 319–359.
5. Murata M. Inflammation and cancer.. 2018;20;23(1):50.
6. Song Q, Liu Z, Huang D. Research progress on the treatment of chronic atrophic gastritis with traditional Chinese medicine.. 2019;40(03):479–482
7. Yan SY, Li QZ.. Beijing: People’s Medical Press;2007.
8. Zhang HB, Duan SW, Zhao TY, et al. Literature case analysis of syndrome bases combined with syndromes in patients with chronic atrophic gastritis.. 2019;19(12): 23–24.
9. Cai YQ, Wei W, Jiang LY. Literature review on distribution features of traditional Chinese medicinesyndromes of chronic atrophic gastritis.. 2018;27(01): 16–18.
10. Su ZQ, Jia MD, Pan JL, et al. Literature review on distribution features of traditional Chinese medicine syndromes and syndrome elements of chronic atrophic gastritis.. 2015;10(12):1636–1639.
11. Xu DZ, Wang Y, Zhang W, et al. The study of literatures on common syndromes and syndrome factors of chronic gastritis.. 2015;35(07):54–56.
12. Lai QQ. Explore the correlation of chronic atrophic gastritis “phlegm, blood stasis” and deficiency syndrome element. Fujian University of Traditional Chinese Medicine;2019.
13. Li Y. The characteristics research of chronic atrophic gastritis precancerous lesions related to “phlegm” and “wet” based on the theory of syndrome factor. Fujian University of Traditional Chinese Medicine;2016.
14. Lin Y. The preliminary study of the relation between chronic atrophic gastritis and blood stasis syndrome element. Fujian University of Traditional Chinese Medicine;2017.
15. Liu G. Study on characteristics of TCM syndrome and therapeutic effect evaluation of chronic atrophic gastritis. China Academy of Chinese Medical Science;2009.
16. Wang P. Study on TCM syndrome treatment and clinical efficacy evaluation of chronic atrophic gastritis. China Academy of Chinese Medical Science;2008.
17. Tang YC, Zhao T, Huang N. et al. Identification of traditional Chinese medicine constitutions and physiological indexes risk factors in metabolic syndrome: adata mining approach.. 2019;2019:1686205.
18. Zhang Y, Zhou AJ, Liu Y. et al. Exploratory factor analysis for validating traditional Chinese syndrome patterns of chronic atrophic gastritis.. 2016;2016:6872890.
19. Liu Y, Liu D, Zhang Y. et al. Markov clustering analysis-based validation for traditional Chinese medicine syndrome patterns of poststroke cognitive impairment.. 2019;25(11):1140–1148.
20. Xu F, Cui W, Kong Q. et al. A real-world evidence study for distribution of traditional Chinese medicine syndrome and its elements on respiratory disease.. 2018;2018:8305892.
21. Zhang Y. Study on the characteristics of syndrome distribution of chronic atrophic gastritis and the mechanism of treating chronic atrophic gastritis by regulating Qi and activating blood and detoxifying based on cytodynamic phenotype. Beijing University of Chinese Medicine;2015.
22. Fang JY, Du YQ, Liu WZ, et al. Consensus on chronic gastritis in China (Shanghai, 2012).. 2013;33(1):5–12.
23. Ministry of Health, PRC.. Beijing: China Medical Science and Technology Press;2002.
24. Li JB, Ma L.. Beijing: China Medical Science and Technology Press;2015.
25. Li JX, Chen J, Lv B, et al. Common views on the diagnosis and treatment of chronic atrophic gastritis combined with traditional Chinese and western medicine (2017).. 2018;26(02):121–131.
26. Liu FB, Wang WQ. Establishment of the spleen-stomach patients reported outcomes scale in Chinese medicine and the corresponding item selection modernization of traditional Chinese medicine and materia medica.. 2009;11(4):527–531.
27. Huang YD. Development and assessment of chronic gastritis module of traditional Chinese medicine spleen and stomach diseases PRO scale. Guangzhou University of Traditional Chinese Medicine;2009.
28. Zhu WF.. Beijing: People’s Medical Press;2008.
29. Ji SL, Cheng ZZ.. Beijing: People’s Medical Press;2002.
30. Correa P, Piazuelo MB. The gastric precancerous cascade.. 2012;13(1):2–9.
31. Liang H, Peng QH, Zhou XQ, et al. Similarity, difference and correlation between syndrome elements and syndrome essential factors.. 2015;38(01): 18–21.
32. Yu CY, Liu T, Liu KG, et al. Establishment and evaluation of disease and syndrome integrated animal model on chronic atrophic gastritis China.. 2018;33(05): 2140–2144.
33. Yin J, Yi JY, Xu B, et al. Diagnosis and treatment of chronic atrophic gastritis with blood stasis theory.. 2019;37(03): 624–627.
34. Zhao X, Wu M, Zhang D, et al. The relationship of interpersonal sensitivity and depression among patients with chronic atrophic gastritis: The mediating role of coping styles.2018;27(5–6):e984–e991.
35. Sun Y, Wang S, Qi M, et al. Psychological distress in patients with chronic atrophic gastritis: the risk factors, protection factors, and cumulative effect.. 2018;23(7):797–803.
36. Arita S, Inagaki-Ohara K. High-fat-diet–induced modulations of leptin signaling and gastric microbiota drive precancerous lesions in the stomach.. 2019;67–68:110556.
37. Liu YM, Zhu FS. Study on therapeutic mechanism of activating blood circulation to remove blood stasis in treating.. 2017;44(11):2299–2301.
38. Zhang BH, Ca YD, Wang P, et al. Consensus of clinical application of gastric mucosa calibration biopsy technique (2018).. 2018;38(12):1496–1500.
39. He HQ, Chen G, Gao JL, et al. Biological basis research progress of syndrome of Qi stagnation and blood stasis.. 2019;34(09):4167–4171.
40. Xu XH, Zhang CP, Sun YN, et al. Study on the syndrome evolution of spleen and stomach damp-heat chronic gastritis.. 2019;21(06):51–57.
41. Huang YC, Pan JL, Huang CY, et al. Literature study on distribution features of traditional Chinese medicine syndromes and syndrome elements in the precancerosis of chronic atrophic gastritis.. 2019;60(20): 1778–1783.
Yue Wei. The Third Affiliated Hospital of Beijing University of Chinese Medicine, No. 51, Xiaoguan Street, Chaoyang District, Beijing 100029, China. E-mail:123109668@qq.com.
:
This study was supported by the National Natural Science Foundation of China (No. 81173232). Authors gratefully acknowledge the value cooperation of Rui-Rui Wang, Ying-Zi Yang, Wan Wang, Ya-Ting Zhao, Chun-Hua Zhang and staff members in the gastroscope room of Dongfang Hospital in collecting data of this survey.
:
CAG, chronic atrophic gastritis; CS, cardinal symptoms; DBSG, dampness and blood stasis group; Dys, dysplasia; EFA, exploratory factor analysis; GA, gastric atrophy; GC, gastric cancer; Hp, helicobacter pylori; IF, independent field; IM, intestinal metaplasia; NDBSG, none of dampness and blood stasis group; OBSG, only blood stasis group; ODG, only dampness group; PHF, physiological field; PLGC, precancerous lesions of gastric cancer; PRO, patient-reported outcome; PSF, psychological field; SEF, social environment field; SS, secondary symptoms; TCM, traditional Chinese medicine.
:
The authors declare that they have no conflict of interest.
:
Chen ZH, Ma LX,Wei Y,Han HX,Xing EL,Yang JX. A cross-sectional study on traditional Chinese medicine syndromes distribution for chronic atrophic gastritis based on data mining.. 2021;4(3):14. doi: 10.12032/MDM2021063010.
:Shan-Shan Lin.
:06 May 2021,
18 June 2021,
:21 July 2021
? 2021 By Authors. Published by TMR Publishing Group Limited. This is an open access article under the CC-BY license (http://creativecommons.org/licenses/BY/4.0/).

- Medical Data Mining的其它文章
- Internet public opinion monitoring in public health emergencies may benefit from artificial intelligence
- Data Mining Method for Exploring the Composition Law and Therapeutic Mechanism of Chinese medicine of macroscopic
- A meta-analysis of the efficacy of traditional Chinese medicine alone in the treatment of refractory gastroesophageal reflux disease
- Study on pharmacodynamic mechanism of compound Shuanghuanglian in prevention and treatment of pneumonia based on network pharmacology and association analysis
- Reporting quality of systematic review protocols of interventions for knee osteoarthritis: a systematic review protocol