
A meta-analysis of the efficacy of traditional Chinese medicine alone in the treatment of refractory gastroesophageal reflux disease
2021-10-16 07:48:02YiHuaFanJingYuXuYunYueZhangLiZhaoWangLingQingYangRuiLiXinJuLi
Medical Data Mining 2021年3期
Yi-Hua Fan, Jing-Yu Xu, Yun-Yue Zhang, Li-Zhao Wang, Ling-Qing Yang, Rui Li, Xin-Ju Li *
A meta-analysis of the efficacy of traditional Chinese medicine alone in the treatment of refractory gastroesophageal reflux disease
Yi-Hua Fan1, 2, Jing-Yu Xu1, 2, Yun-Yue Zhang3, Li-Zhao Wang3, Ling-Qing Yang3, Rui Li3, Xin-Ju Li3 *
1First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin 300193, China.2National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, Tianjin 300381, China.3Tianjin University of Traditional Chinese Medicine, Tianjin 301617, China.
To systematically evaluate the efficacy and safety of traditional Chinese medicine in the treatment of refractory gastroesophageal reflux.PubMed, The Cochrane Library, Embase, Web of Science, China National Knowledge Infrastructure, Wanfang Database, China Science and Technology Journal Database and Chinese BioMedical Literature Database were searched for randomized controlled trials of traditional Chinese medicine in the treatment of refractory gastroesophageal reflux from database establishment time to December 2020. After two researchers independently screened the literature, extracted data and evaluated the bias risk included in the study, RevMan5.3 software was used for meta-analysis.A total of 12 randomized controlled trials, were included, including 893 patients. The results of meta-analysis showed that the total effective rate of the treatment group (relative risk= 1.28, 95% confidence interval (CI) (1.19, 1.38),< 0.00001), RGERDQ (refractory gastroesophageal reflux disease) score (mean difference (MD) = ?3.35, 95% CI (?4.13, ?2.57),< 0.00001], acid reflux (acid in the stomach comes out of the mouth) [MD = ?0.30, 95% CI (?0.45, ?0.15),< 0.00001], heartburn (the feeling that the heart is burned) (MD = ?0.44, 95% CI (?0.60, ?0.29),< 0.00001, and retrosternal pain (MD = ?0.27, 95% CI (?0.44, ?0.10),< 0.00001, belching (MD = ?0.40, 95% CI (?0.57, ?0.24),< 0.00001], endoscopic mucosal score (MD = ?0.62, 95% CI (?0.78, ?0.46),< 0.00001], the differences were statistically significant, and the effective rate of mucosal improvement under endoscopy was= 0.93 > 0.05, with no statistically significant difference.The current evidence shows that traditional Chinese medicine in the treatment of refractory gastroesophageal reflux disease is better than that of western medicine in the total effective rate, relieving acid reflux, heartburn, retrosternal pain and belching symptoms, but it is impossible to judge the improvement of mucosa under endoscope. Due to the limitations of the quality and quantity of included studies, more high-quality studies are needed to confirm the above conclusions.
Oral administration of traditional Chinese medicine, Refractory gastroesophageal reflux disease, Meta-analysis, Randomized controlled trial
Background
In recent years, the incidence of gastroesophageal reflux disease (GERD) has been increasing gradually, and the prevalence of GERD in Western Europe and North America is 10%–20% [1]. GERD patients are also common in China. Among adults in China, the prevalence of symptomatic GERD is 3.1% [2, 3]. After standardized proton pump inhibitor treatment, most GERD patients’ symptoms such as acid reflux (acid in the stomach comes out of the mouth) and heartburn (the feeling that the heart is burned or burned) can be completely relieved, but up to 30% of GERD patients’ symptoms are not well controlled. At present, it is widely considered that GERD, whose symptoms such as acid regurgitation and heartburn cannot be significantly improved after 8–12 weeks of standardized treatment with double dose of proton pump inhibitor, can be called refractory gastroesophageal reflux disease (RGERD) [4, 5].
At present, western medicine believes that the pathogenesis of refractory gastroesophageal reflux includes esophageal functional disorders, high esophageal sensitivity, persistent weak acid and non-acid reflux, persistent acid reflux, differences in drug metabolism, and psychological factors, etc. [6, 7]. Optimized proton pump inhibitor regimen is the preferred method for the treatment of RGERD [8], which is often combined with H2receptor antagonists, gastric motivity drugs, antacids and neuromodulators, etc. For those who fail to respond to conservative treatment, endoscopic surgery can be performed [9, 10]. However, the clinical effect is poor and prone to recurrence [6]. Traditional Chinese medicine has the advantages of obvious curative effect and less side effects in treating this disease through syndrome differentiation [11]. In traditional Chinese medicine, RGERD is classified into the categories of “vomiting acid”, “noisy”, “stomachache” and “regurgitation”. The etiology and pathogenesis are as follows: the weakness of the spleen and stomach is caused by unsmooth emotion, injury caused by diet, excessive fatigue or weakness of the spleen and stomach or common bile disease, the liver and gallbladder fail to drain, the stomach loses harmony and decreases, and the stomach Qi (a special Chinese medicine term: refers to the physiological functions and essence of the stomach) is reversed due to deficiency [11]. In the, it is recommended that Chaihu Shugan powder (classic ancient prescription), Zuojin pill combined with Huagan decoction, Sinisan combined with Liujunzi decoction, Wendan decoction, Sijunzi combined with Danshen decoction and Banxia Xiexin decoction (all of those decoction belong to the classic ancient prescription) should be treated according to syndrome differentiation[12].
The reasonable and effective treatment scheme for RGERD is still a difficult problem urgently solved by the medical profession. It is the first priority of treatment to solve the actual pain for patients by giving play to the respective therapeutic advantages of Chinese and western medicine [13]. In recent years, the clinical treatment of RGERD by oral administration of traditional Chinese medicine is more and more reported, but the sample size is small. There is no systematic evaluation on the treatment of RGERD with traditional Chinese medicine. Therefore, a meta-analysis of randomized controlled trials (RCTs) on the treatment of RGERD by oral administration of traditional Chinese medicine was conducted to provide reliable evidence for clinical work and scientific research.
Methods
Inclusion criteria
Study type. RCT, whether blinded or not, the language was limited to Chinese or English.
Subjects. Patients with RGERD diagnosed according to the diagnostic criteria of RGERD. Gender, age, race, nationality and region are not limited.
Intervention measures. The treatment group was treated by oral administration of simple Chinese medicine; The control group was treated by oral administration of western medicine.
Efficacy indicators. Main efficacy indicators: total effective rate, clinical efficacy judgment according to theissued by the Ministry of Health in 1993. Secondary efficacy indicators: (1) symptom score, referring to GERDQ questionnaire, including total score and symptom score about acid reflux, heartburn, subternal pain and belching; (2) the changes of Endoscopic assessment of oesophagitis were referred to the clinical and functional correlates and further validation of the Los Angeles classification, USA in 1994 [14]; (3) the expression of PAR2 and TRPV1; (4) the pressure of upper and lower esophageal sphincter of, length of lower esophageal sphincter, amplitude of esophageal peristalsis and percentage of synchronous contraction; (5) the incidence of adverse reactions. One of the above primary and secondary efficacy indicators was included in the analysis.
Exclusion criteria
(1) The most complete and high-quality studies were included in the repetitive publications. (2) Non-clinical RCT articles, such as reviews, theoretical studies, retrospective studies and animal experiments. (3) In addition to oral administration of traditional Chinese medicine, there are other intervention measures in, such as acupuncture and moxibustion combined with traditional Chinese medicine, etc.. (4) Literature on the treatment of RGERD with integrated traditional Chinese and Western medicine. (5) here are no relevant literature on efficacy indicators. (6) Studies in which the outcome efficacy rating criteria are not standardized or not mentioned. (7) Research that cannot obtain indicator data.
Retrieval strategy
Pubmed, the Cochrane Library, Embase, Web of Science, China National Knowledge Infrastructure, Wanfang Database, China Science and Technology Journal Database and Chinese BioMedical Literature Database were searched by computer. The search time limit is from the establishment of the database to December 2020. The search adopts the combination of subject words and free words. English keywords include: “refractory gastroesophageal reflux disease”, “refractory reflux esophagitis”.
Literature screening and data extraction
Two investigators independently screened the literature, extracted the data, and cross-checked. In case of any disagreement, the dispute shall be settled through discussion with a third party. First, read the title and abstract to conduct a preliminary screening of the literature, after excluding the literature that obviously does not meet the inclusion criteria, further read the full text for re-screening, and determine the final inclusion of the literature. If necessary, contact the original study authors by email or telephone to obtain unidentified but important information for this study. The data extracted included: (1) basic information of the included study: the title of the article, the first author, the year of publication, the number of cases in each group, the baseline characteristics of the patients, and the diagnostic criteria of the disease; (2) intervention measures and treatment course; (3) efficacy indicators; (4) judgment elements of bias risk, such as random method, with or without allocation concealment and blind method.
Quality evaluation of literature included in the study
Two researchers assessed the methodological quality of the included studies in terms of “l(fā)ow risk”, “high risk” and “unclear” in terms of random method generation, allocation scheme, blind method implementation of researchers and subjects, measurement bias of result evaluators, data integrity of results, selective reporting bias and other bias. The third party shall assist the judgment. The risk of bias was assessed using the risk assessment tool of RCT bias recommended by Cochrane Handbook 5.1.0 [15].
Statistical analysis
The meta-analysis was performed using the software RevMan 5.3 provided by the Cochrane Collaboration. For continuous variables, if the units or tools of the measurement indexes are the same, the mean difference (MD) is used as the effect analysis statistic; if the measurement tools or units are not consistent, the standard mean difference (SMD) is used as the effect analysis statistic. Relative risk (RR) was used as the effective analysis statistic for the two categorical variables, with 95% confidence interval (CI) provided for each effect size. Heterogeneity among the included study results was quantitatively judged by2tests combined with2. If> 0.10,2≤ 50%, there was no significant heterogeneity among the studies, and the fixed effect model was used for meta-analysis. If≤ 0.10,2> 50%, the heterogeneity among studies is considered significant, then the source of heterogeneity is analyzed. After excluding the influence of obvious clinical heterogeneity, a random effect model was used for meta-analysis. The level for the meta-analysis was set as α = 0.05. Sensitivity analysis was used to observe the effect of a single study on pooled effect size and analyze the stability of meta-analysis results. When more than 10 studies were included for outcome measures, funnel plots were used to qualitatively evaluate publication bias.
Results
Literature screening process and results
A total of 3,044 relevant articles were retrieved, and 2,030 articles were obtained after re-examination. 1,793 articles were excluded from reading titles and abstracts, 225 articles were excluded from reading 237 articles in full text, and finally 12 articles were included [16–27]. The literature screening process is shown in Figure 1.
Basic characteristics of including studies
The basic characteristics of the study included are shown in Table 1. The treatment group was treated with simple oral traditional Chinese medicine alone, with different drug taste composition. The control group was treated with a proton pump inhibitor combined with gastrointestinal motility drugs. See Table 2 for the characteristics of the interventions with treatment periods of 8 or 12 weeks.
Bias Risk Evaluation Results for including Studies
The quality of the included 12 articles [16–27] was evaluated using the RCT bias risk assessment tool recommended in Cochrane Handbook 5.1.0. Five literature [19, 24–27] correctly used the method of random sequence generation; three articles [16, 20, 21] were evaluated as high risk in allocation concealment, and the other nine articles [18, 19, 22–27] were not mentioned; three articles [16, 20, 21] evaluated high risk in terms of blinding; all articles [16–27] were evaluated as low risk in terms of incomplete outcome measures, selective reporting, and other biases. The results of the bias risk evaluation are shown in Figure 2.
Meta-analysis results
Total effective rate. A total of 10 RCTs were included [16–22, 24–26], including 813 patients. There was no statistical heterogeneity among the studies (= 0.96,2= 0%). And meta-analysis using a fixed effects model showed: the difference of total effective rate between treatment group and control group was statistically significant (RR = 1.28, 95% CI (1.19, 1.38),< 0.00001). Subgroup analysis was performed on RCT at 8 weeks and 12 weeks respectively, and 8 RCT were included at 8 weeks of treatment [16–19, 22, 24–26]. Including 669 patients, there was no statistical heterogeneity among the studies (= 0.95,2= 0%) (Figure 3). The results of fixed effect model meta-analysis showed that the difference of total effective rate between the treatment group and the control group was statistically significant (RR = 1.26, 95% CI (1.17, 1.36),< 0.00001). Two RCTs were included over 12 weeks[20, 21], including 144 patients, with no statistical heterogeneity between studies (= 0.98,2= 0%). The results of fixed effect model meta-analysis showed that the difference of total effective rate between the treatment group and the control group was statistically significant (RR = 1.41, 95% CI (1.10, 1.80),< 0.00001) (Figure 3).
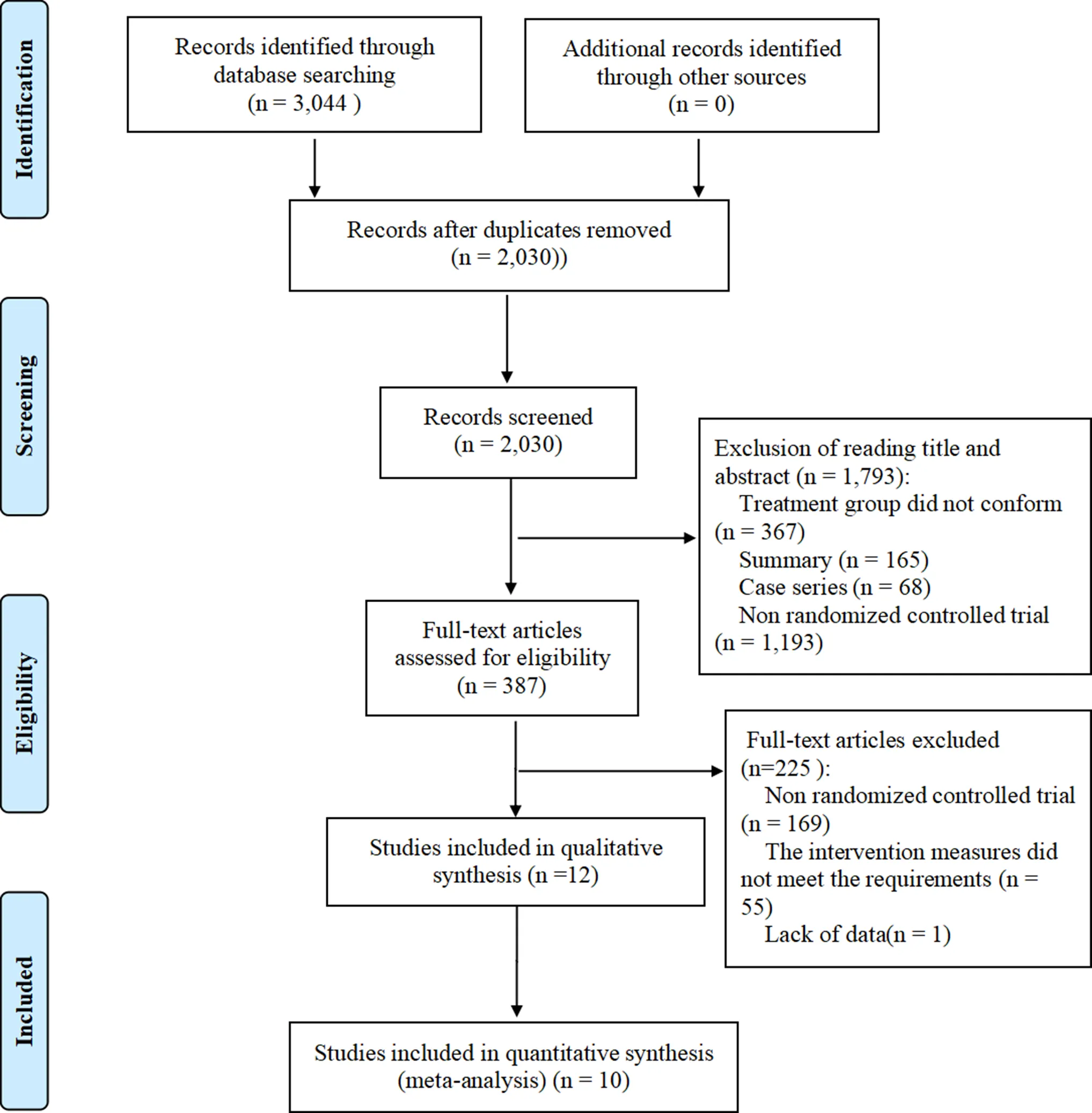
Figure 1 Flow chart of literature screening

Table 1 Basic characteristics of included studies
Outcome indicators: ① total effective rate; ② acid reflux (acid in the stomach comes out of the mouth), heartburn (the feeling that the heart is burned or burned), subternal pain; ③ belching; ④ endoscopic mucosal improvement; ⑤ adverse reactions; ⑥ total score of symptoms and signs; ⑦ PAR2 and TRPV1 protein expression; ⑧ esophageal upper and lower sphincter pressure, lower esophageal sphincter length, esophageal peristaltic amplitude and synchronous contraction percentage. Diagnostic criteria: a,; b,; c,; d,; e,; f,; g,; T, treatment group; C, control group; -, not mentioned.
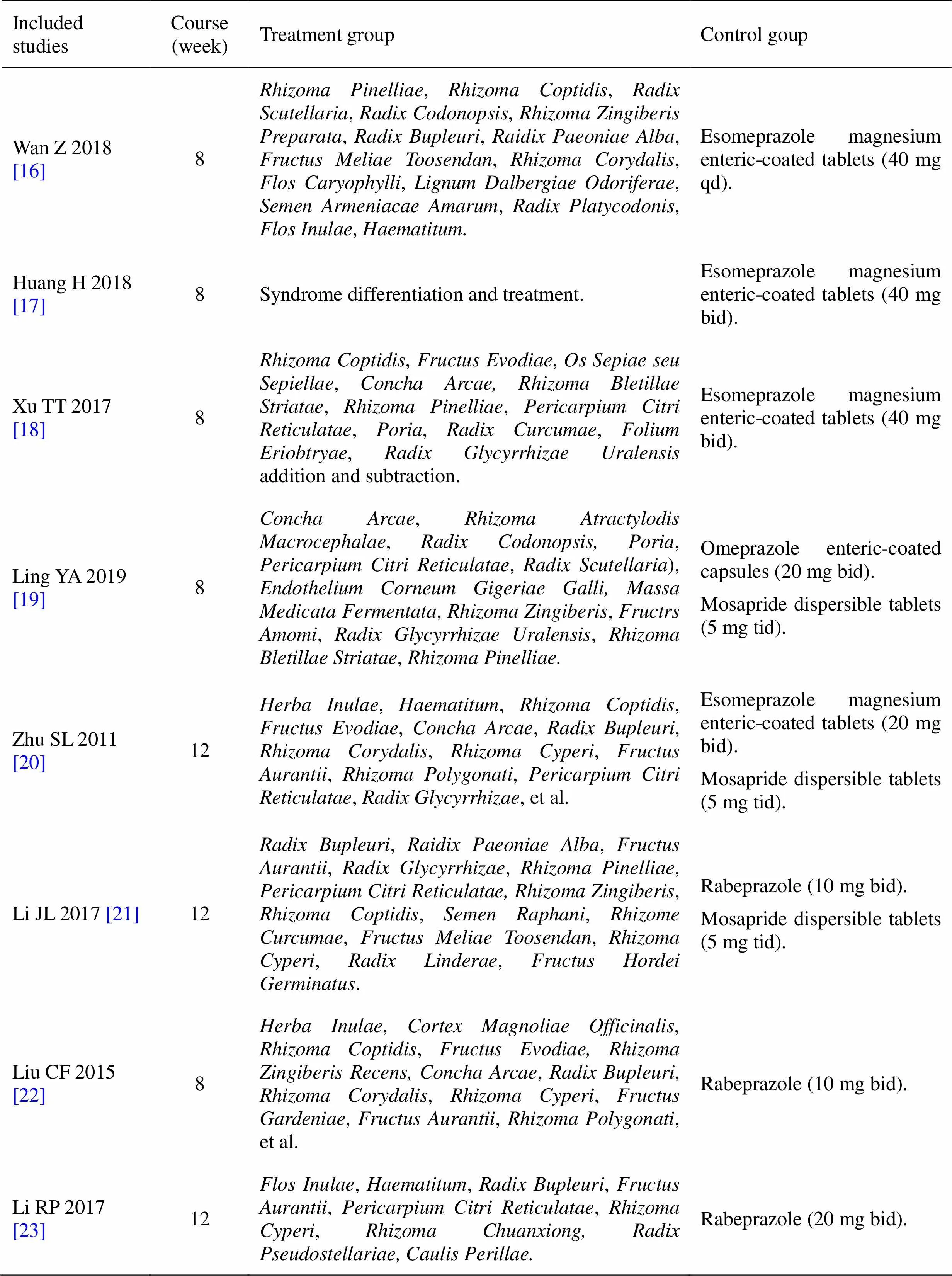
Table 2 Characteristics of interventions
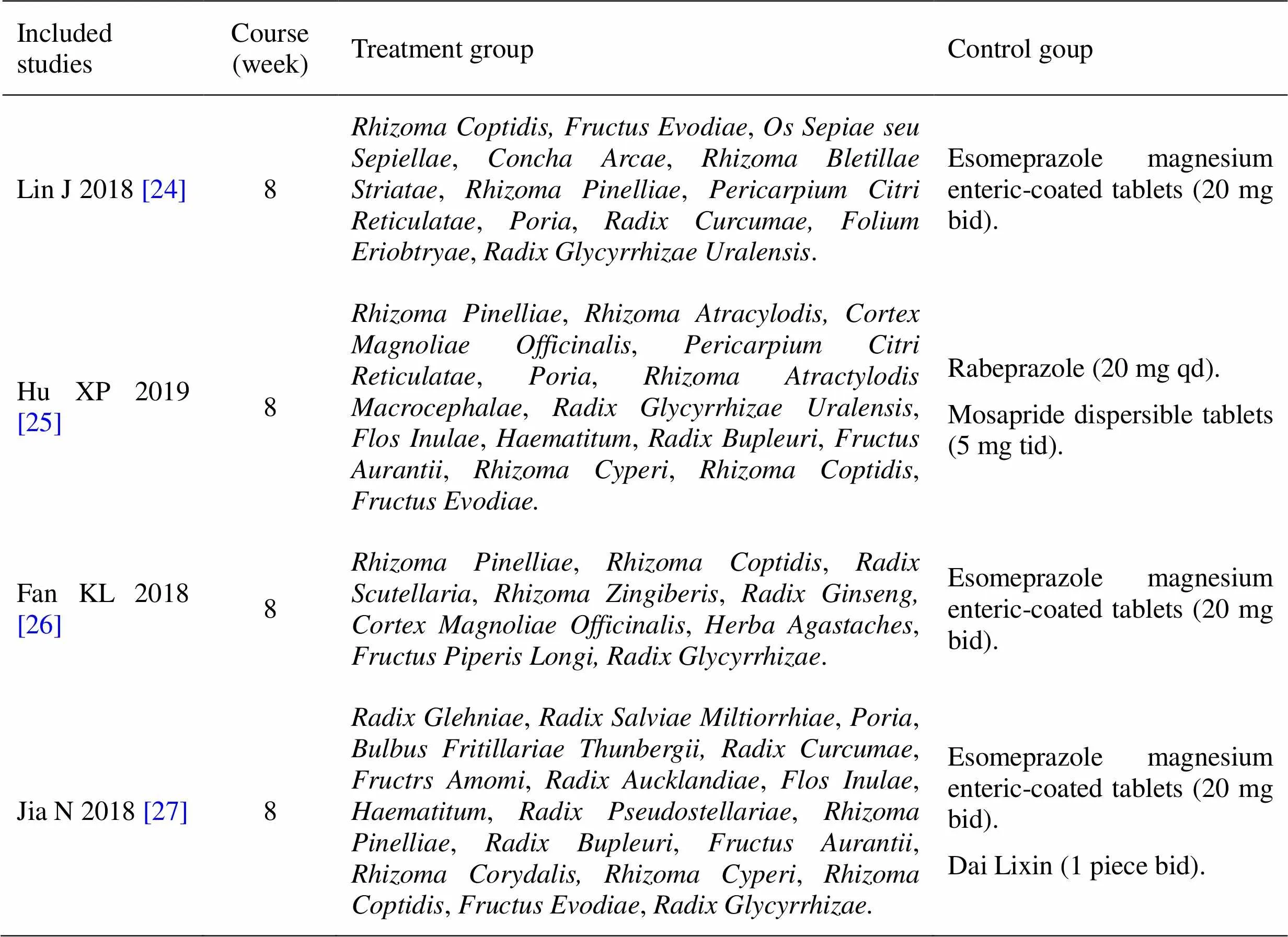
Table 2 Characteristics of interventions (Continued)
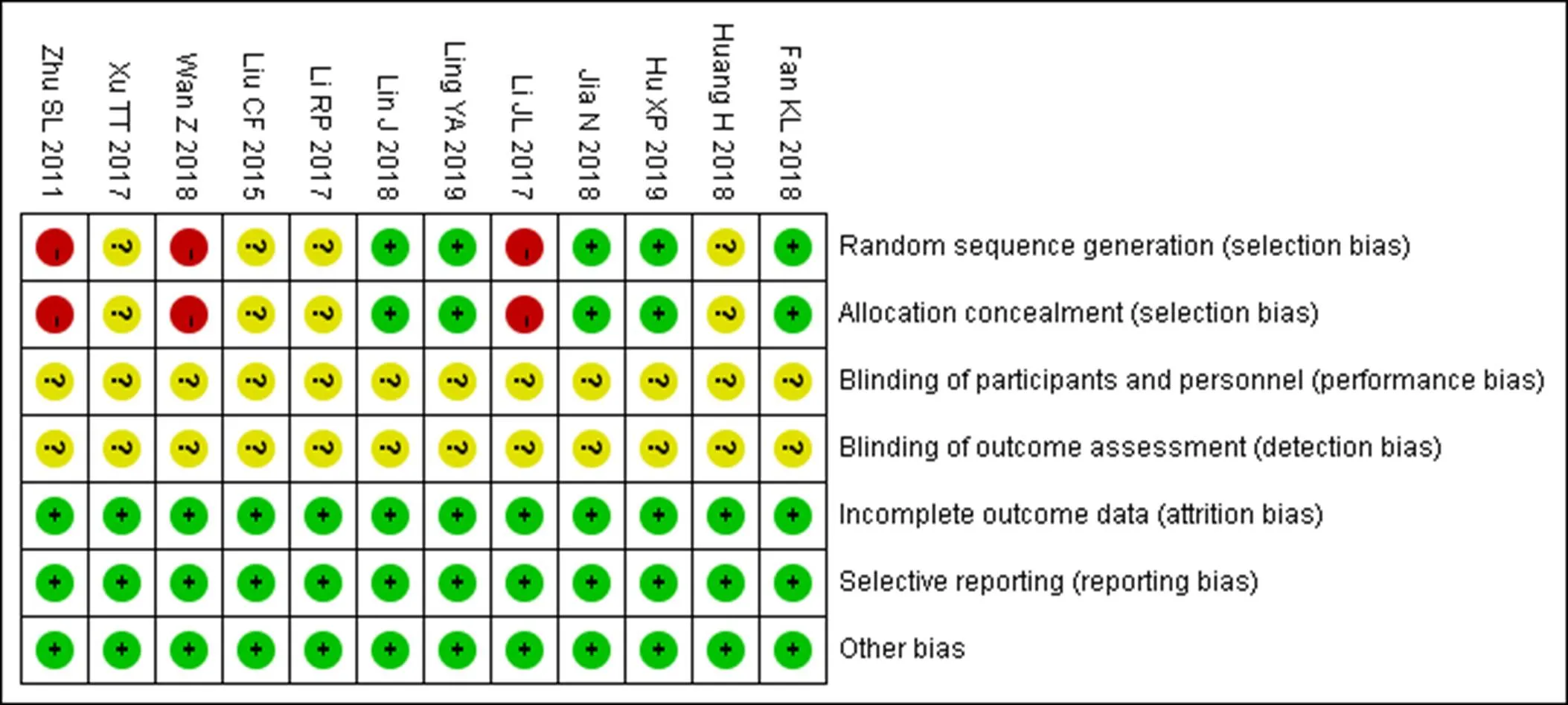
Figure 2 Bias risk summary chart
Figure 3 Meta-analysis of total effective rate of treatment group and control group for refractory gastroesophageal reflux disease
Symptom and signs integral. Seven RCTs [17, 18, 20–22, 25, 26] reported total scores of symptoms and signs, comprising 539 patients, heterogeneity test:= 0.49,2= 0%, no statistical heterogeneity, the fixed effect model Meta results showed the total score of symptoms and signs in the treatment group and the control group (MD = ?3.35, 95% CI (?4.13, ?2.57),< 0.00001), the difference was statistically significant (Figure 4). Five RCTs [16, 18, 19, 25, 26] reported symptoms score of acid reflux, heartburn, and subternal pain, each comprising 406 patients, three RCTs [16, 18, 26] reported belching symptom score, including 212 patients.There was no statistical heterogeneity among the studies (= 0.12,2= 30%). The results of meta-analysis using fixed effect model showed that the diffierence was statistically significant in acid reflux (acid in the stomach comes out of the mouth) in treatment group and control group (MD = ?0.30, 95% CI (?0.45, ?0.15),< 0.00001), heartburn (the feeling that the heart is burned or burned) status (MD = ?0.44, 95% CI (?0.60, ?0.29),< 0.00001), retrosternal pain status (MD = ?0.27, 95% CI (?0.44, ?0.10), P < 0.00001), belching symptoms (MD = ?0.40, 95% CI (?0.57, ?0.24), P < 0.00001) (Figure 5).
Endoscopic mucosal improvement. Four RCTs [16, 20, 22, 26] reported an effective rate of endoscopic mucosal improvement, comprising 223 patients, heterogeneity test:= 0.04,2= 64%, indicating heterogeneity between studies. Through the analysis of the study, it was found that the course of study of Zhu SL was 12 weeks, while the course of study of the other three was 8 weeks. Excluding Zhu SL’s study, the heterogeneity did not change, but no other clinical heterogeneity was found, so statistical heterogeneity was considered and random effect model was used. The results of meta-analysis showed that= 0.93 > 0.05, indicating that there was no statistical significance between groups (Figure 6). Two RCTs [17, 19] reported changes in endoscopic mucosal score in 220 patients, heterogeneity test:= 0.35,2= 0%, no heterogeneity. Meta results of fixed effect model were used to show the endoscopic mucosal score of the treatment group and the control group (MD = ?0.62, 95% CI (?0.78, ?0.46), P < 0.00001), the difference was statistically significant (Figure 7).
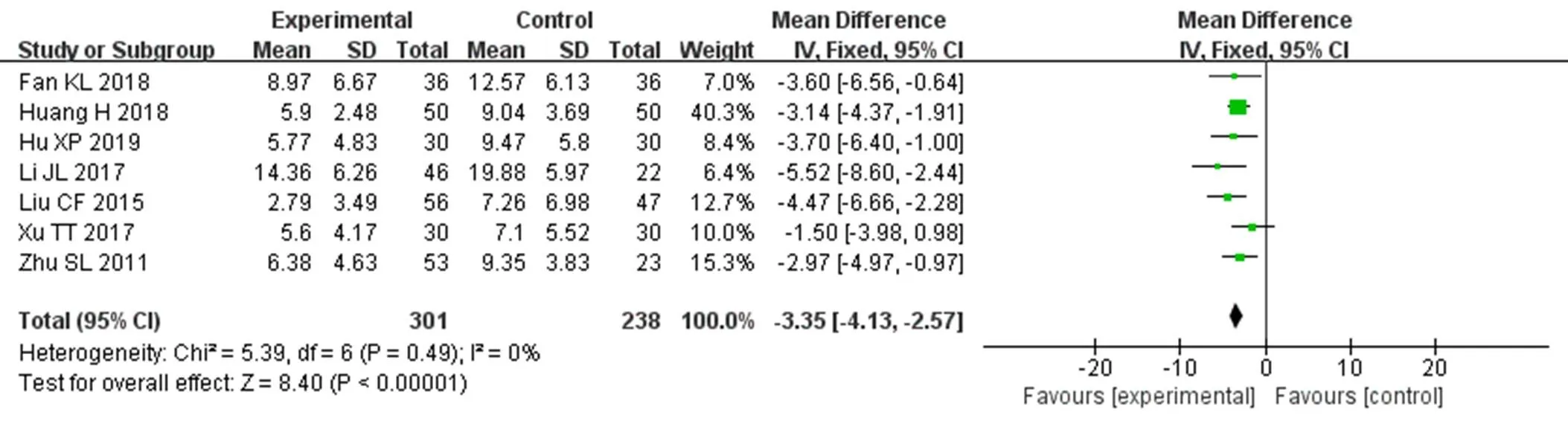
Figure 4 meta-analysis of total score of symptoms and signs between treatment group and control group
Figure 5 Meta-analysis of symptom score comparison between treatment group and control group
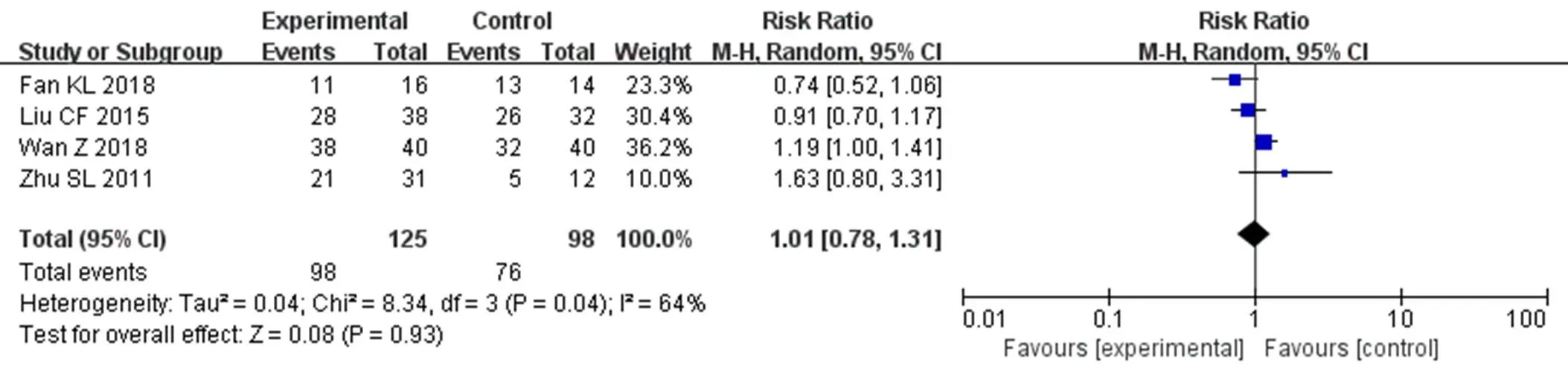
Figure 6 Meta-analysis of the effective rate of endoscopic mucosal improvement between the treatment group and the control group
Figure 7 Meta-analysis of endoscopic mucosal score in treatment group and control group
PAR2 and TRPV1 protein expression. One RCT[23]reported the expression of PAR2 and TRPV1 protein in esophageal mucosa, which indicated that both the treatment group and the control group could reduce the expression of PAR2 and TRPV1 protein in esophageal mucosa. However, there was no statistical difference between the groups. The sample included in this study is small, and it has little help in clinical guidance.
Pressure of upper and lower esophageal sphincter, length of the lower esophageal sphincter, amplitude of esophageal peristalsis and percentage of synchronous contraction. One RCT [27]reported upper and lower esophageal sphincter pressure, lower esophageal sphincter length, esophageal peristaltic amplitude and percentage of synchronous contraction, the results indicated that the treatment group was superior to the control group in improving the pressure of upper esophageal sphincter and the amplitude of esophageal fluctuation, and the treatment group was similar to the control group in improving the pressure of lower esophageal sphincter and the length of lower esophageal sphincter. There was no statistical difference between the groups in the percentage of synchronous contraction. The sample included in this study is small, and the clinical guidance is of little significance.
Adverse reactions. Six RCTs [16–18, 24–26] reported no adverse reactions in the treatment group and the control group during the course of the disease, and the other six RCTs[19–23, 27]did not describe the adverse reactions.
Sensitivity analysis. The sensitivity analysis of the above indexes was performed by eliminating one by one, and the change of effective quantity and-value was observed after excluding one by one and including the study. The results showed that there was no significant change in the effective quantity and-value of the above outcome indicators excluding anyone article, suggesting that the results of meta-analysis have good stability and reliability.
Publication bias detection. The funnel plot of the publication bias of the total effective rate of the included articles is shown in Figure 8, which is asymmetric, suggesting that there may be publication bias.
Discussion
Characteristics and efficacy of oral Chinese medicine in treatment of RGERD
The difficulty of RGERD treatment lies in how to control non-acid reflux (acid in the stomach comes out of the mouth) such as gas or bile, lack of clear western medicine treatment when multiple symptoms appear, poor effect of acid inhibition treatment and easy recurrence of disease [28]. At present, there is no unified special prescription for the treatment of RGERD of traditional Chinese medicine, and the clinical treatment is mainly based on syndrome differentiation. Zhang J et al. [29] analyzed the common prescriptions of this disease through literature: Chaihu Shugan powder, Banxia Xiexin decoction, Zuojin pill, Banxia Houpu decoction, Xuanfu Daizhe decoction and Huangqi Jianzhong decoction (all of those belong to the classic ancient prescription). But there are also physicians who add or subtract treatment with a principal formula, for example, Wei BH [30] treated RGERD with the empirical formula (,,,,,,,, etc.) with satisfactory clinical effect. Liu W [31]treated RGERD with self-prepared prescription (,,,,,,,,,,,). The clinical effect was satisfactory.
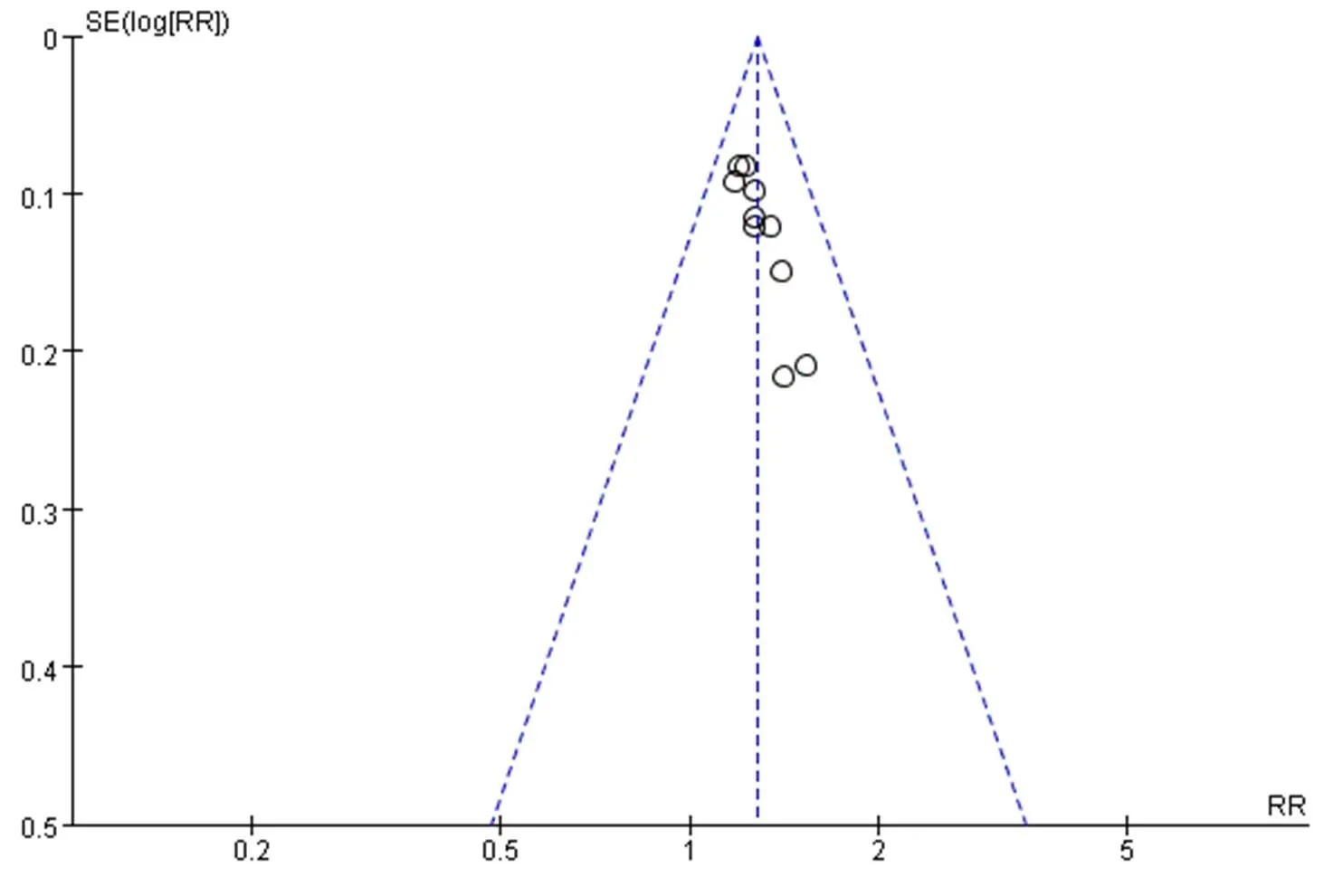
Figure 8 Funnel plot
Although different treatments are different, according to the 12 RCTs included in this study, some drugs have common features, such ascan lower stomach Qi, and can relieve depression of heat;,dry dampness and eliminate phlegm;,soothe the liver and regulate Qi;produce acid to relieve acid reflux (acid in the stomach comes out of the mouth) symptoms;harmonize various medicines to strengthen and protect the spleen and stomach and relieve the cold and heat of the whole prescription. Modern pharmacology studies have found thathas anti-inflammatory, inhibitory gastric acid secretion and anti-ulcer effects [32];can promote the secretion of digestive enzymes, relieve gastrointestinal gas accumulation, regulate gastrointestinal function, enhance appetite, and have spasmolysis effect [33];has good anti-inflammatory, anti-ulcer and anti-emetic effects [34]; tetrahydropalmatine incan non-competitively inhibit gastric acid secretion in rat stomach, and has certain protective effect on ulcer[35];can increase gastric mucosal defense factor to achieve anti-ulcer effect, with anti-inflammatory and immunomodulatory effects [36].
Twelve RCTs of oral administration of traditional Chinese medicine alone in the treatment of refractory GERD were evaluated. The results of meta-analysis are shown blow. (1) In terms of the total effective rate, no matter the course of treatment was 8 weeks or 12 weeks, the treatment of RGERD was treated with traditional Chinese medicine alone. Compared with western medicine, the total effective rate was higher. (2) The total score of GERDQ questionnaire and the single score of acid regurgitation, heartburn (the feeling that the heart is burned or burned), subternal pain and belching in the treatment group were significantly lower than those in the control group. The results showed that oral administration of traditional Chinese medicine alone was superior to western medicine in improving the common symptoms of patients. (3) There was no statistical difference between the treatment group and the control group in the effective rate of endoscopic mucosal improvement, so it was impossible to evaluate the advantages and disadvantages of the treatment group and the control group in the effective rate of gastric mucosal improvement. However, in the endoscopic mucosal score, the treatment group was superior to the control group in improving the mucosal score, and the reasons leading to the difference in the results of similar indicators were analyzed. It may be that in the case of small sample size, it is not easy to count the difference in count data, but it is relatively easy to count the difference in measurement data, so it is necessary to increase the sample size to prove the advantages and disadvantages between the two groups. (4) There was no significant difference in reducing the expression of PAR2 and TRPV1 between the two groups. (5) The treatment group was superior to the control group in improving the pressure of upper esophageal sphincter and the amplitude of esophageal fluctuation, and the treatment group was similar to the control group in improving the pressure of lower esophageal sphincter and the length of lower esophageal sphincter. There was no significant difference in the percentage of synchronous contraction between the two groups. (6) No adverse reactions were reported in the included studies, indicating that both traditional Chinese medicine and western medicine have high safety.
Study limitations
There are some limitations in this study. (1) The quality of some included studies is low, the specific random methods, allocation concealment and blind methods are less described, and there may be some bias, which has some influence on the reliability of the results. (2) The sample size of the included study was small and the test power was insufficient, which affected the accuracy of the results. (3) The included studies were all from China, and their universality was poor. (4) Only three studies reported the follow-up after treatment, which was not enough to judge the long-term efficacy and safety of the drug. (5) Due to the treatment of TCM syndrome differentiation and the particularity of TCM decoction itself, there are great differences in the composition, dosage and syndrome type of prescriptions used in various studies. To some extent, the evaluation of the effectiveness of the intervention affects the authenticity of the results. (6) The sample size of some outcome indicators is too small and the clinical guidance is insufficient.
Conclusion
To sum up, the current evidence proves that compared with western medicine treatment, the total effective rate of oral administration of traditional Chinese medicine alone in the treatment of RGERD is, the curative effect is better in relieving the clinical symptoms of acid reflux (acid in the stomach comes out of the mouth), heartburn (the feeling that the heart is burned or burned), subternal pain and belching, and the safety is better. However, in terms of improving the endoscopic mucosa, it also needs to increase the sample size for further judgment, and in addition, there needs to be a long-term follow-up study to prove the long-term efficacy of traditional Chinese medicine treatment. And most of the literature included in this study are of low quality, and more high-quality studies are needed to confirm the above conclusions.
1. Ates F, Francis DO, Vaezi MF. Refractory gastroesophageal reflux disease: advances and treatment.2014;8(6):657–667.
2. Hershcovici T, Fass R. An algorithm for diagnosis and treatment of refractory GERD.. 2010;24(6): 923–936.
3. Scarpellini E, Ang D, Pauwels A, et al. Management of refractory typical GERD symptoms.. 2016; 13(5):281–294.
4. Branch of Digestive, China Medical Association. Expert consensus on gastroesophageal reflux disease in China in 2014.. 2015;20(3):155–168.
5. Fock KM, Talley N, Goh KL, et al. Asia-pacific consensus on the management of gastro-oesophageal reflux disease: an update focusing on refractory reflux disease and Barrett’s oesophagus.. 2016;65(9):1402–1415.
6. Chen YR, Que RY, Shen YT, Lin LB, Li Y. Research progress of traditional Chinese and Western medicine in refractory reflux esophagitis.. 2017;41(6): 575–577, 584.
7. Hershcovici T, Fass R. An algorithm for diagnosis and treatment of refractory GERD.. 2010;24(6): 923–936.
8. Jia JN, Tang YP, Liu X. Comparative study on Causes and treatment of refractory gastroesophageal reflux disease.. 2019;40(11):2646–2649.
9. Ivashkin VT, Maev IV, Trukhmanov AS, et al. Modern achievements in the diagnosis and treatment of the refractory gastroesophageal reflux disease.. 2018;90(8):4–12.
10. Li SF, Li WB, Fan FF, et al. Advances in treatment of refractory gastroesophageal reflux disease.. 2017;22(7): 439–442.
11. Song N, Tang LM, Yuan HX. Distribution of TCM Syndromes of refractory gastroesophageal reflux disease based on cluster analysis.. 2018; 50(10):58–61.
12. Guo Y, Su XL, Shi HX, et al. Current situation and strategy of traditional Chinese and Western medicine treatment of refractory gastroesophageal reflux disease.. 2016;11(9):1185–1188, 1191.
13. Lu Q, Lei TT, Wang YL, et al. Pathogenesis and treatment progress of refractory gastroesophageal reflux disease.. 2017;38(10): 1212–1216.
14. Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification.. 1999;45(2): 172–180.
15. Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions. http://handbook.cochrane.org.
16. Wan Z. Clinical observation on 40 cases of refractory reflux esophagitis teated with Hejiang method. Hubei University Traditional Chinese Medicine;2018.
17. Huang H, Zhang Y, Liu ZC, et al. Chief physician Huang Fu Bin’s experience in treating refractory gastroesophageal reflux disease.. 2018;41(4):30–33.
18. Xu TT. Clinical efficacy of Jiawei Zuojin pill in the treatment of refractory gastroesophageal reflux disease of liver stomach stagnation heat type. Nanjing University Traditional Chinese Medicine;2017.
19. Ling YA, Li XH. Clinical study on method of regulate cold and warm mildly for refractory reflux esophagitis of cold and heat in complexity type.. 2019;51(8):128–130.
20. Zhu SL, Wang GF, Cheng YM, et al. Therapeutic effect of modified Shugan Hewei recipe on 53 cases of refractory gastroesophageal reflux disease. Presented at: China Association of Chinese Medicine. Proceedings of the 23rd National Symposium on Spleen and Stomach Diseases of Spleen and Stomach Disease Branch of China Association of Chinese Medicine; Haikou.
21. Li JL, Zhang SX. Clinical study on 46 cases of refractory gastroesophageal reflux disease treated with Sinixiexin decoction.. 2017;12(8):1045–1047, 1063.
22. Liu CF. Peripheral mechanism of visceral hypersensitivity in refractory gastroesophageal reflux disease and intervention of Shugan Hewei herbs. Shanghai University Traditional Chinese Medicine;2015.
23. Li RP, Cao W, Zhang JJ, et al. Effect of Shugan Jianpi Hewei recipe on PAR2 and TRPV1 protein expression in esophageal mucosa of patients with refractory gastroesophageal reflux disease.. 2017;39(2):80–82.
24. Lin J. Comparative observation on the efficacy of modified Zuojin pill and esomeprazole in the treatment of refractory gastroesophageal reflux disease of liver stomach stagnation heat type.. 2018;23(3):364–366.
25. Hu XP. Clinical efficacy of modified Erchen Pingwei Powder on refractory gastroesophageal reflux disease of Qi stagnation and phlegm obstruction type. Guangxi University Traditional Chinese Medicine;2019.
26. Fan KL. Clinical observation of Shunwei Jiangni decoction in the treatment of refractory gastroesophageal reflux disease. Shanxi University Traditional Chinese Medicine;2018.
27. Jia N, Tang YP. Curative effect of Yisuan Jiangni compound on refractory gastroesophageal reflux disease.. 2018;24(1):3–6.
28. Branch of Gastrointestinal Disease, China Association of Chinese Medicine. Expert consensus traditional Chinese medicine diagnosis and treatment of GERD (2017).. 2017;25(5):321–326
29. Zhang J, Wang FY, Wang AL, et al. The law of commonly used prescriptions and couplet medicines for gastroesophageal reflux disease.. 2015;56(10):881–883.
30. Zhou T, Shen QY. Clinical efficacy of professor Wei Beihai in the treatment of refractory gastroesophageal reflux disease. Presented at: Digestive System Diseases Committee of Chinese Society of Integrated Traditional Chinese and Western Medicine. Proceedings of the 27th National Conference on Digestive System Diseases of Integrated Traditional Chinese and Western Medicine; Changsha.
31. Liu W. Traditional Chinese medicine treatment of 30 cases of refractory gastroesophageal reflux syndrome.. 2007;20(4):56–57.
32. Qiu YP. Research progress on chemical constituents and pharmacological effects of Coptis chinensis.. 2018;10(22):141–143.
33. Wang ZL, Zhang X, Liu SJ, et al. Historical evolution and research status of.. 2017;35(10):118–122.
34. Zuo J, Mou JG, Hu XY. Research progress in the chemical constituents and modern pharmacological effects of.. 2019;21(9): 26–29.
35. Shang K, Li JW, Chang MY, et al. Research ofW.T.Wang pharmacological effects.. 2019;39(1): 108–110.
36. Li J, Li X, Cao MM, et al. Research progress in pharmacological actions of liquorice and proportion of couplet medicines in combination.. 2019;53(7):83–87.
Xin-Ju Li. Tianjin University of Traditional Chinese Medicine, No. 10, Poyang Lake Road, West District, Tuanbo New Town, Jinghai District, Tianjin 301617, China. E-mail: mars402498971@126.com.
:
GERD, gastroesophageal reflux disease; RGERD, refractory gastroesophageal reflux disease; RCT, randomized controlled trial; MD, mean difference; RR, relative risk; CI, confidence interval.
:
The authors declare that they have no conflict of interest.
:
Fan YH, Xu JY, Zhang YY, et al. A meta-analysis of the efficacy of traditional Chinese medicine alone in the treatment of refractory gastroesophageal reflux disease.. 2021;4(3):15. doi: 10.53388/MDM2021073011.
:Shan-Shan Lin.
:06 May 2021,
25 May 2021,
:30 July 2021
? 2021 By Authors. Published by TMR Publishing Group Limited. This is an open access article under the CC-BY license (http://creativecommons.org/licenses/BY/4.0/).

- Medical Data Mining的其它文章
- Internet public opinion monitoring in public health emergencies may benefit from artificial intelligence
- Data Mining Method for Exploring the Composition Law and Therapeutic Mechanism of Chinese medicine of macroscopic
- A cross-sectional study on traditional Chinese medicine syndromes distribution for chronic atrophic gastritis based on data mining
- Study on pharmacodynamic mechanism of compound Shuanghuanglian in prevention and treatment of pneumonia based on network pharmacology and association analysis
- Reporting quality of systematic review protocols of interventions for knee osteoarthritis: a systematic review protocol