
Meta-analysis of the effect of continuing nursing on the psychological status of rectal cancer patients undergoing stoma
2022-02-15 04:54MengXiGaoLyuChengAiYingZhangWeiFanTianTianGaiYanWang
Nursing Communications 2022年13期
Meng-Xi Gao,Lyu Cheng,Ai-Ying Zhang,Wei Fan,Tian-Tian Gai,Yan Wang
1Department of Graduate, Tianjin University of Traditional Chinese Medicine, Tianjin 301600, China. 2Department of Nursing, Tianjin University of Traditional Chinese Medicine,Tianjin 301600,China.
Abstract Objective: To systematically evaluate the effect of continuous nursing on the psychological status of rectal cancer patients undergoing stoma. Methods: Five databases including China HowNet, Chongqing Weipu Chinese Science and Technology Database, Wanfang Database,Embase and PubMed were searched. Randomized controlled trials were collected on the effect of continuing nursing on the psychological status of rectal cancer patients undergoing stoma. The searching time was from the establishment of the database to March 30, 2019.RevMan 5.3 software was used to analyze the bias risk of the study after two researchers independently screened the researchers, extracted the data and evaluated the bias risk of the study. Results: A total of 15 studies were included. Meta‐analysis showed that the continuing nursing group improved anxiety [MD = –10.89, 95% CI (–13.52, –8.26), P <0.00001], depression [MD = –4.78, 95% CI (–5.77, –3.80, P <0.00001], fear [MD =–6.06, 95% CI (–7.70, –4.43), P <0.00001], hostile [MD = –7.00, 95% CI (–13.62,–0.38), P = 0.04 <0.05], somatization [MD = –7.63, 95% CI (–13.49, –1.77), P = 0.01<0.05]. The self‐care ability [MD = 38.24, 95% CI (35.38, 41.11), P <0.00001] was superior to the routine nursing group. Conclusion: Continuous nursing has more advantages than routine nursing, and it can improve the negative psychological state of rectal cancer patients undergoing stoma. Due to the limitations of the quantity and quality of the included studies, the above conclusions need to be verified by more high‐quality studies.
Keywords:continuous nursing care; rectal cancer; stoma; systematic evaluation
Background
The World Health Organization report shows [1] that the incidence of colorectal cancer in recent five years is about 10.9%, which is only lower than that of breast cancer and prostate cancer in malignant tumors. Surgical treatment is currently recognized as an effective method of treatment, of which about 5%‐30% of patients with low rectal cancer need permanent enterostomy [2]. About 100,000 patients in our country annually undergo the operation [3]. The appearance of rectal cancer stoma has a serious impact on the physical and psychological health of patients [4]. Studies have shown that [5]effective nursing intervention can effectively alleviate the psychological state of depression, anxiety and fear of rectal cancer patients with stoma, and promote the recovery of the stoma. Many patients and their caregivers can not fully grasp the knowledge and skills of enterostomy nursing only through nursing intervention during hospitalization [6]. Traditionally, when a patient leaves the hospital,it means that their care has nothing to do with the hospital. Only when the patient returns to the hospital can he get the health information related to the disease. This routine nursing mode is challenging to meet the health needs of most patients [7]. With the development of society, people are also accepting new health concepts, patients’ needs for their own treatment and care are also increasing, especially after discharge, which makes continuing care become a hot topic in nursing research [8].
Continuous nursing service can meet the needs of rectal cancer stoma patients from in‐hospital to out‐of‐hospital care. After discharge, patients are still given a series of nursing care, appropriate nursing and health education, improve the quality of life of patients[9], alleviate their psychological pressure [10]. Studies have shown that [11] Continuous nursing intervention for rectal cancer patients undergoing stoma after the operation can effectively help patients’anxiety, depression and other adverse emotions, and improve patients’self‐care ability. Jian‐Hai Liu’s [12] study found that continuing nursing strengthened communication with patients, alleviated the degree of patients’ autism, improved patients’ inferiority, fear,anxiety, and other negative psychological states, and the optimization effect of psychological behavior was significant. However, there is still no valid evidence for the impact of continuing nursing on the psychological status of rectal cancer patients undergoing stoma. Based on the relevant literature, this study collects and collates the existing studies at home and abroad for systematic evaluation to provide reliable evidence‐based basis for continuing nursing in rectal cancer patients undergoing stoma. To improve the psychological condition of patients to a certain extent.
Materials and methods
Inclusion and exclusion criteria
(1) study type: publicly published randomized controlled trial on the impact of continuity of care on the psychological status of patients with rectal cancer; (2) study subjects: patients with rectal cancer stoma; (3) intervention: continuity of care in the test group; and routine care in the control group.
Outcome Indicators Main Indicators. (1) Anxiety: Self‐rating Anxiety Scale (SAS) [13] has 20 items, the degree of anxiety is proportional to the score, Normal: <50 points; Mild anxiety: 50‐60 points; Moderate anxiety: 61‐70 points; Severe anxiety: >70 points.(2) Depression: Self‐rating Depression Scale (SDS) [14], the degree of depression is proportional to the score, No depression: <53 points;Mild depression: 53‐62 points; Moderate depression: >63‐72 points;Severe depression: >73 points. (3) Fear, hostility and somatization:Symptom Check‐List 90 (SCL‐90) [15] scale has 90 items and 9 factors.Derogatis grade 5 scoring method is used.Factor score(>1.5)is a positive sign. The main indicators used in this paper are fear,hostility and somatization. Secondary indicators: (1) Self‐care ability:The exercise of self‐care agency (ESCA) [16] was used. There were 4 dimensions and 43 items on the scale. The four dimensions were self‐concept, health knowledge level, self‐care skills and self‐care responsibility. The scale was scored by Lickett 5, with a total score of 172.The higher the score,the stronger the self‐care ability of patients.Exclusion criteria. (1) Repeated publications; (2) Exclusion of meetings, case reports, abstracts of conference papers and researchers’reviews; (3) Neither Chinese nor English research; (4)Non‐randomized controlled trials.
Researches Retrieval Strategy
Use the computer to retrieve the Chinese search words: “延續(xù)性護理”,“延續(xù)護理”, “延續(xù)護理干預”,“院外護理”, “連續(xù)性護理”,“持續(xù)性護理”,“直腸癌造口”, “ 心理”. Search Chinese databases such as CNKI, Wan Fang Date and VIP database. English databases such as Embase and PubMed are retrieved by keywords such as “extended nursing”,“continuing nursing”, “continuous nursing”, “transitional care intervention”, “Stoma” and “rectal cancer”. The retrieval time is from the establishment of the database to March 2019.
Researches screening and data extraction
Two researchers independently searched the research according to the strategy of research return. After the retrieval, they read the research alone. First, they read the title and abstract of the research, excluding the apparent inconsistencies. Then they read the full text according to the inclusion and exclusion criteria. If there are differences, they will be decided by a third researcher.
Bias risk assessment included in research
Two independent researchers used the Cochrane Manual evaluation criteria to assess the bias risk included in the study.
Statistical analysis
RevMan 5.3 software was used to analyze the data. Relative risk (RR)was used as the effective index for counting data, mean difference(MD) was used as the effective index for measuring data, and 95% CI was provided for each effect. Heterogeneity was determined by 2 test(a=0.1), andI2quantitatively judged the heterogeneity. If there is no statistical heterogeneity among the results, the fixed effect model is used for meta‐analysis; if there is statistical heterogeneity among the studies, the random effect model is used. The apparent clinical heterogeneity was treated by subgroup analysis or sensitivity analysis,or only descriptive analysis.
Results
Researchers’ screening process and results
A total of 897 types of research (775 in Chinese and 122 in English)were retrieved in this study. 309 duplicated articles were deleted after re‐checking, and 588 documents were included. 230 articles were excluded after reading the title and abstract, 36 articles were included after reading the full text, 21 articles were excluded after entering the exclusion criteria, and 15 randomized controlled trials were finally included,including 663 cases in the experimental group and 664 cases in the control group. The process and results of the researchers’screening are shown in Figure 1.

Figure 1 Researchers screening flow chart
Basic characteristics of included studies
All the 15[17‐31] researches were randomized controlled trials. There was no significant difference in the primary data between the experimental group and the control group. The baseline was well comparable. The basic features included in the study are shown in Table 1.
Results of bias risk assessment included in the study
All 15 [17‐31] randomized controlled trials (RCTs) were evaluated strictly according to the Cochrane Manual evaluation criteria. 15 RCTs did not mention the implementation of random allocation hiding and blind method. Only 7 RCTs reported the generation method of random sequence, and 8 RCTs only said randomization. The bias risk assessment included in the study is shown in Figures 2 and 3.
Meta-analysis results
The effect of continuous nursing on the anxiety of rectal cancer patients undergoing stoma. A total of 875 patients in 10 RCTs were included [17, 19, 20, 21, 22, 23, 24, 25, 28, 30]. 438 patients in the experimental group and 437 patients in the control group were assessed by a self‐rating anxiety scale. Heterogeneity test results showed thatP<0.00001,I2= 96% >50%. Meta‐analysis using random effect model showed significant statistical significance[MD =–10.89, 95% CI(–13.52, –8.26),P<0.00001], see Figure 4.
The effect of continuous nursing on depression of rectal cancer patients undergoing stoma. A total of 580 patients in 7 RCTs were included [17, 18, 20, 23, 25, 28, 29, 30]. 291 patients in the experimental group and 289 patients in the control group. Self‐rating depression scale was used to evaluate the effect of continuing nursing on the depression status of rectal cancer stoma patients.Heterogeneity test results showed thatP= 0.12 >0.05,I2= 41 <50%. A random effect model was used for analysis. Meta‐analysis showed that the difference was significant [MD = -4.78, 95% CI (-5.77, -3.80),P<0.00001], as shown in Figure 5.
The influence of continuous nursing on fear, hostility and somatization of rectal cancer patients undergoing stoma.
Inclusion of 3 [26, 27, 31] studies reported the psychological status of patients in fear, hostility and somatization. Heterogeneity test results showed that the heterogeneity among the studies was greater (P<0.05,I2>50%), so the random effect model was used for analysis.Meta‐analysis showed that fear [MD = –6.06, 95% CI (–7.70, –4.43),P<0.00001], hostility [MD = –7.00, 95% CI (–13.62, –0.38),P=0.04 <0.05], somatization [MD = –7.63, 95% CI (–13.49, –1.77),P= 0.01 <0.05]. There was a significant difference between the two groups. Compared with the control group, the experimental group had a better psychological state of fear, hostility and somatization, as shown in Table 2.
The influence of continuous nursing on patients’self-care ability.
Inclusion of 3 [23, 25, 30] studies reported the status of patients in terms of self‐care capabilities. Heterogeneity test results showed that there was no statistical difference between the studies (P= 0.43 >0.05,I2= 0% <50%). Therefore, the stationary effect model was used to analyze the difference between the two groups [MD = 38.24,95% CI (35.38, 41.11),P<0.00001]. The self‐care ability of the experimental group was higher than that of the control group, as shown in Figure 6.
Publication bias
The funnel chart was drawn with the effect of depression as the outcome index, and the publication bias of 7 articles was observed.The results show that most studies focus on the upper and middle parts of the inverted funnel map, which are distributed within the interval, but their symmetry is low. Possibly because of publication bias or negative deletion results, see Figure 7.

Table 1 Basic features included in the study
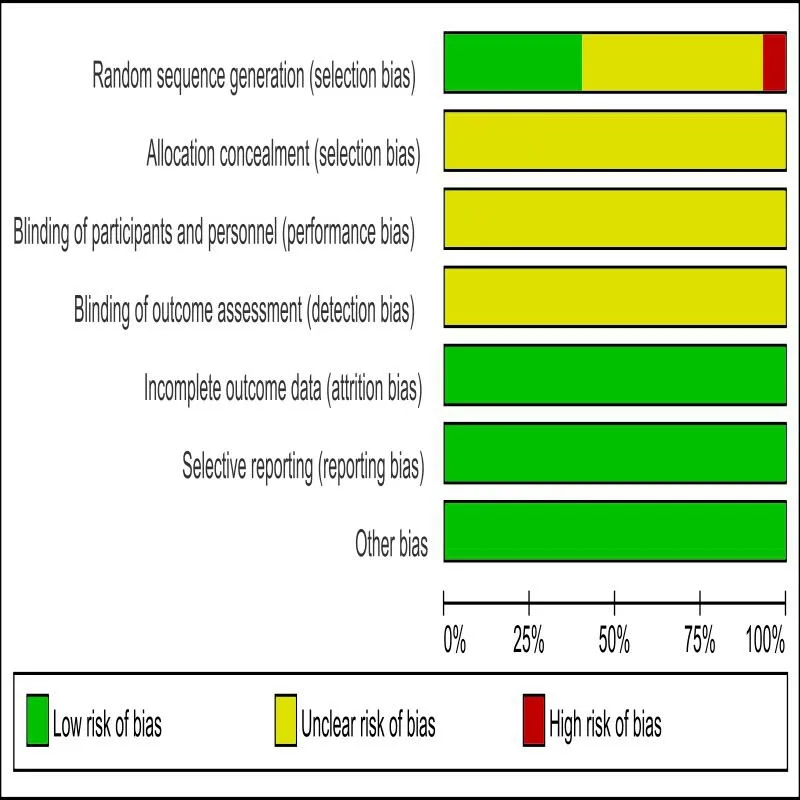
Figure 2 Results of risk assessment of inclusion bias

Figure 3 Results of risk assessment of inclusion bias

Figure 4 Meta-analysis of anxiety status in two groups of rectal cancer patients undergoing stoma

Table 2 Meta-analysis of fear,hostility and somatization in two groups of rectal cancer patients undergoing stoma
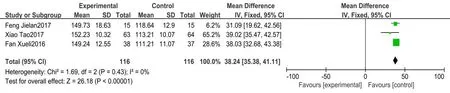
Figure 6 Meta-analysis of self-care ability of two groups of rectal cancer patients undergoing stoma
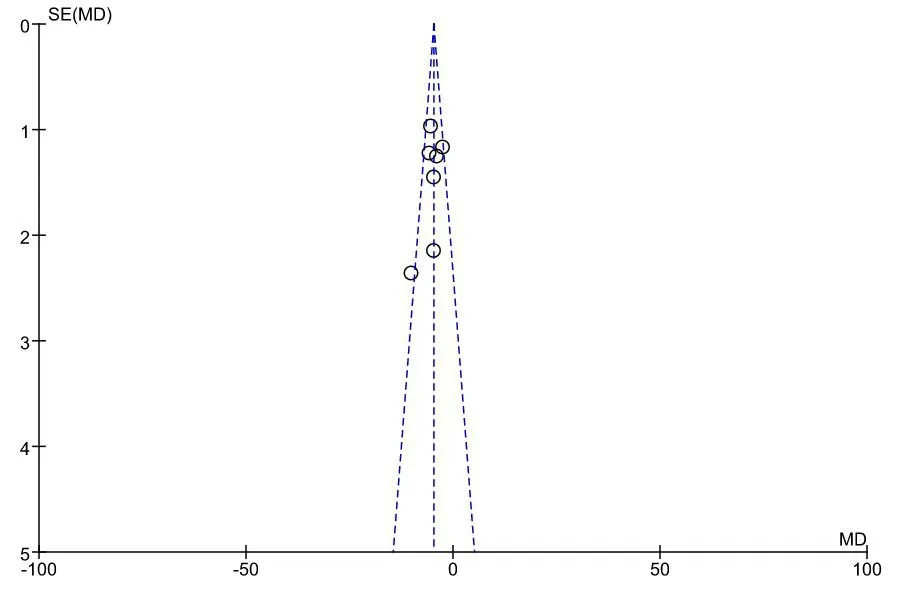
Figure 7 Funnel chart for comparison of depression status between two groups of rectal cancer patients undergoing stoma
Discussion
Because of the change of people’s lifestyle and dietary habits, the morbidity of modern colorectal cancer is increasing year by year.According to Chinese cancer statistics [32], 376,000 new cases and 191,000 deaths of colorectal cancer were reported in 2015, and the incidence and mortality ranked fifth among all malignant tumors.Rectal cancer is one of the most common malignant tumors of the digestive tract in China, and its incidence is high. About 75% of them are low [33]. In 1908, Dr. Miles published in Lancet a radical operation for rectal cancer, abdominoperineal resection (APR) [34].Combined abdominoperineal resection (APR) is the complete removal of the whole tissue including the tumor itself, the diseased intestine and mesentery, and the lymph nodes around the tumor through the combined abdominoperineal approach [35]. Up to now, combined abdominal and perineal resection (Miles operation) is still the standard operation for treating low rectal cancer [36].
Because of the need for treatment, the colostomy is to fix the proximal colon outside the abdominal wall, from which excrement is discharged outside the body, also known as the artificial anus [37].The establishment of enterostomy has greatly changed the physiological structure of patients, caused great inconvenience to patients’ daily life, and also brought psychological pressure to patients, making patients feel inferior because they are different from ordinary people [38]. Continuous nursing refers to a series of nursing activities, such as telephone follow‐up, home visits, health education based on a network platform, continuous nursing center, Community Cancer Rehabilitation Club, patient association, etc. To ensure the coordination and continuity of medical care received by patients when they are transferred between different health care sites or healthcare institutions at different levels, so as to prevent the deterioration of the health status of high‐risk patients [39].
After the patient is discharged from the hospital, the medical staff can directly talk with the patient or family members through telephone follow‐up and a home visit, and provide individual nursing,treatment and other related health information for the patient by understanding the situation of different patients. Some studies have shown that by increasing the communication between cancer patients who have been discharged from the hospital, the compliance of cancer patients with pain after discharge can be improved, to improve their pain control ability and psychological burden [40]. Medical staff set up a QQ group, WeChat group, forum, etc. Through the network platform to carry out health education for patients in the form of group chat, answer questions and solve doubts for patients and their families, maintain good doctor‐patient interaction, and reduce patients’ uneasiness. The continuous nursing center also provides more professional and convenient patients services. After the patients are discharged from the hospital, the constant nursing center provides constant service and complete process management of skilled nursing.Medical staff can give special lectures on the treatment, rehabilitation,self‐care and health concept of related diseases.
The community cancer rehabilitation organization can introduce the knowledge of intestinal training, stoma nursing and diet guidance to patients and their families in detail by holding free clinics, special lectures, meeting professors, singing and dancing performances and other activities, and using emotional cognitive therapy and other related methods to make patients actively face their conditions,change patients’ wrong cognition of colostomy and make patients slowly accept it change of defecation mode. It is beneficial to increase patients’ confidence and safety, reduce their fear of colostomy,promote the adjustment of patients’ psychological state, and effectively avoid complications caused by colostomy infection. The establishment of patients’ associations [41] encourages patients to help each other and share experiences, fully understand the physical and psychological conditions of patients, and provide psychological care to patients through experience sharing, playing light music,relaxation training, which is conducive to alleviating their anxiety,depression and other negative emotions, thereby improving the quality of life.
According to the statistical analysis of 15 RCTs included in this study, the continuous nursing intervention programs mainly include telephone follow‐up, door‐to‐door follow‐up, customized personal files of patients, health education based on the network platform,continuous nursing center, Community Cancer Rehabilitation Club,patient fellowship, etc. Through these nursing intervention programs,the medical staff can pay more attention to the psychological situation of patients after stoma, guide patients to adopt a more appropriate lifestyle, conduct better psychological guidance to patients, and promote the physical and mental health.
There are still some limitations in this study: (1) Publishing bias may exist if only a published study is included. (2) Included studies are domestic studies, which do not exclude the possibility of selection bias.(3) All the included studies have not reported whether to allocate concealment and blind methods, and there may be bias. More clinical trials are needed to confirm this. (4) Nursing strategies may differ among the intervention groups,which may lead to bias in the outcome of the merger. Therefore, it is suggested that these conditions be fully considered in future studies to minimize bias, ensure inter‐group comparability, and improve the feasibility and quality of the study.
Conclusion
In conclusion, the existing evidence shows that continuing nursing can affect patients’ psychological status, improve patients’ negative emotions such as anxiety, depression, fear, hostility and somatization,and also improve patients’ self‐care ability to a certain extent. Limited by the quantity and quality of research, more and higher quality studies need to verify the above conclusions.
猜你喜歡
經(jīng)濟與管理(2020年4期)2020-12-28
實用醫(yī)學雜志(2020年19期)2020-10-31
數(shù)學年刊A輯(中文版)(2020年2期)2020-07-25
新世紀智能(語文備考)(2019年12期)2020-01-13
新聞傳播(2018年13期)2018-08-29
災害醫(yī)學與救援(電子版)(2018年1期)2018-06-05
中華老年口腔醫(yī)學雜志(2016年2期)2017-01-15
中學生數(shù)理化·七年級數(shù)學人教版(2016年4期)2016-11-19
中國老年保健醫(yī)學(2015年5期)2015-01-25
中華皮膚科雜志(2014年4期)2014-12-19
 Nursing Communications2022年13期
Nursing Communications2022年13期
- Nursing Communications的其它文章
- Delphi and Analytic hierarchy process for the construction of a risk assessment index system for post-stroke shoulder-hand syndrome
- A review of obstacles and facilitating factors of implementing Clinical Ladder Programs in nursing
- Spiritual health, empathy ability and their relationships with spiritual care perceptions among nursing students in China:A cross-sectional correlational study
- Qualitative study on influencing factors of refusal of gastric tube placement in stroke patients with dysphagia
- The influence of professional identity and ageism on turnover intention in nursing homes: a cross-sectional study from suzhou, China
- The relationship of family separation and nutrition status among under-five children: a cross-sectional study in Panti Public Health Center, Jember Regency of East Java, Indonesia