
Treatment of hyperkalemic emergencies
2022-09-17 07:10:08YaoWuYangyangFuHuadongZhuJunXuJosephHaroldWalline
Yao Wu, Yang-yang Fu, Hua-dong Zhu, Jun Xu, Joseph Harold Walline
1 Emergency Department, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Science and Peking Union Medical College, Beijing 100730, China
2 Centre for the Humanities and Medicine, the University of Hong Kong, Hong Kong, China
Hyperkalemic emergency (HE) refers to life-threatening hyperkalemia consisting of a high serum potassium level with severe complications (e.g., dysrhythmias, cardiac arrest, or myopathy).Hyperkalemic emergencies (HEs)are commonly encountered (2%–3%) in the emergency department (ED).In-hospital mortality rate for hospitalized hyperkalemic patients is about 14.1%and 4.5 times higher than that of those with normal potassium.Quick recognition and treatment are critical for decreasing morbidity and mortality.Nevertheless,great variety and sparse evidence lie in current HE treatment. In this article, we will review the current medical literature on the treatment of HEs and propose a treatment f lowchart for HEs (Figure 1).
THRESHOLDS FOR INITIATING TREATMENT OF HEs
No consistent thresholds for potassium levels warranting treatment have been proposed.First, higher serum potassium is associated with higher mortality.A retrospective multicenter study revealed that higher serum potassium levels, severe underlying diseases,and developing acute kidney injury (AKI) from normal baseline renal function were associated with higher mortality.Second, electrocardiogram (ECG) changes indicate higher risk of mortality in hyperkalemia.Elevated serum potassium in cardiac myocytes results in cardiac instability inducing ventricular fibrillation and cardiac arrest.Higher mortality occurs in patients with serum potassium ≥6.0 mmol/L possessing new ECG changes than those without ECG changes.
Based on present studies and guidelines, we recommend treatment should be initiated under the following circumstances: (1) serum potassium ≥6.0 mmol/L with or without ECG changes; (2) presence of more than two ECG changes, clinical manifestations of hyperkalemia, and risk factors for hyperkalemia(Table 1), with serum potassium 5.5–5.9 mmol/L;(3) a clinical course likely to progress to hyperkalemia, suchas in anuresis patients complicated by rhabdomyolysis or tumor lysis syndrome, even if the serum potassium is <6.0 mmol/L.Nonetheless, more evidence-based studies are necessitated concerning thresholds for HE treatment.
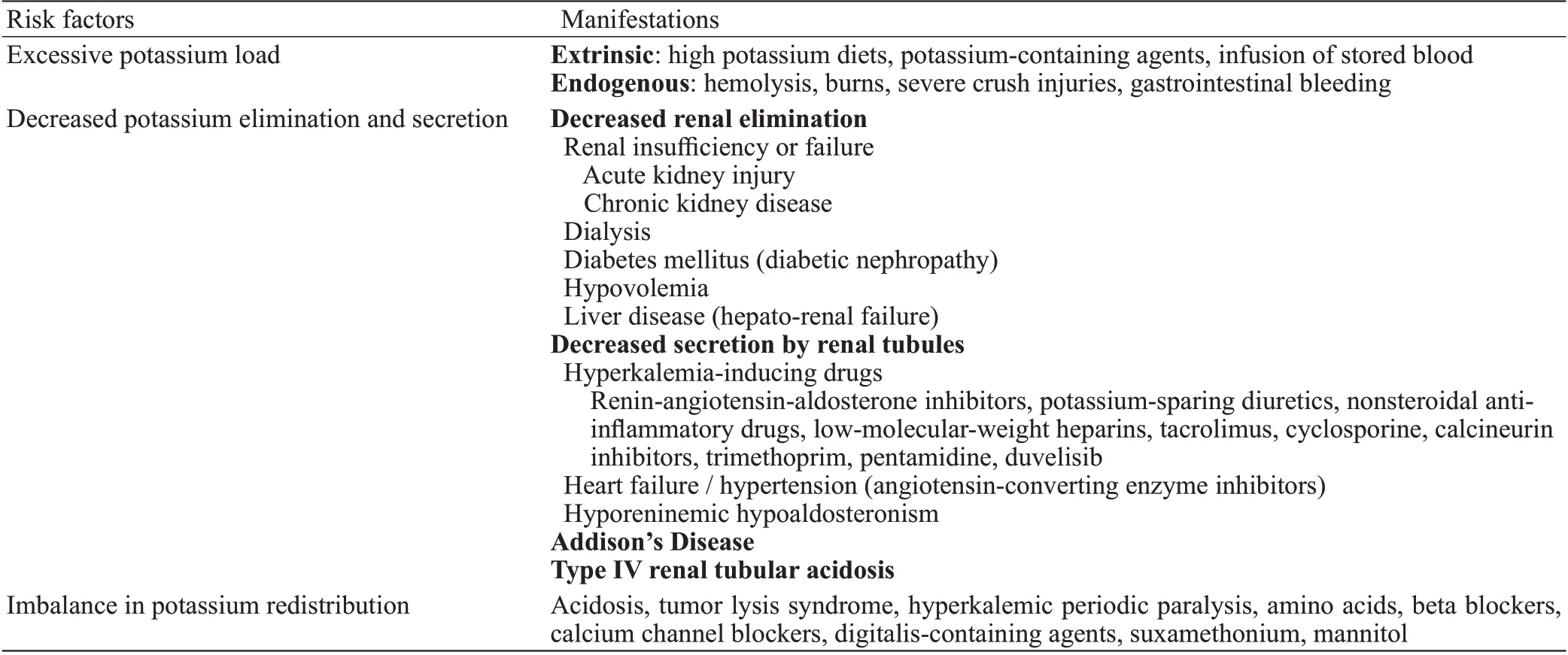
Table 1. Risk factors for hyperkalemia

Figure 1. A f lowchart for treatment of hyperkalemic emergencies. ECG: electrocardiogram; POC: point of care; K+: potassium; IV: intravenous;SZC: sodium zirconium cyclosilicate.
TREATMENT
Cardiac myocyte protection—intravenous (IV)calcium salts
Calcium salts antagonize the cardiotoxic effects of hyperkalemia, restore the cardiac membrane potential,and stabilize the myocardium.A total of 10 mL of 10% calcium gluconate or one ampule of calcium chloride should be administered intravenously if new and potentially fatal ECG changes including absent P waves,widened QRS, peaked T waves, sine waves, ventricular arrhythmias, or cardiac arrest, appear.Efficacy of IV calcium salts can be seen within 5 min. If life-threatening ECG changes persist after 5–10 min, repeat calcium salts are necessary.
Since calcium salts do not lower serum potassium levels, they need to be combined with potassium-lowering treatments. More proven side eff ects of calsium chloride include tissue necrosis, which can be avoided by using a central venous catheters. Hypotension can be induced by the peripheral vasodilation and bradycardia effects of calcium chloride infusions.Advanced studies are needed because the effi cacy of calcium salts was more based on case reports and anecdotal experience rather than large prospective cohort study.
Shifting serum potassium intracellularly
The combination of insulin and glucose is rapid and a mainstay of treatment for HEs.Insulin increases the activity of sodium- and potassium-activated adenosine triphosphatase (Na-K-ATPase) in skeletal muscle cells thus decreasing serum potassium levels.When blood glucose is ≥13.9 mmol/L and serum potassium exceeds 6.0 mmol/L, insulin could be given alone to lower serum potassium. If blood glucose is <13.9 mmol/L, an IV bolus injection of 10 units of regular insulin should be followed by a 25 g (50 mL of a 50% solution) bolus of dextrose.Alternatively, IV infusion with 10 units of insulin in 25 g dextrose (250 mL of a 10% solution) over 60 min is another option. Of the two, IV boluses are the faster means of lowering serum potassium in HEs.
One in six hyperkalemic patients developed hypoglycemia between 1–3 h after receiving an insulinglucose treatment,which suggests that current glucose and insulin regimens have much room for improvement.An IV infusion of 10% dextrose at a rate of 50–75 mL/h and close monitoring of glucose after IV insulin-glucose treatment for 5–6 h is recommended to avoid iatrogenic hypoglycemia.
-
Beta-2 agonists can also promote potassium moving intracellularly by activating Na-K-ATPase.If calcium salts and insulin-glucose fail to control HEs, nebulized beta-2 agonists (albuterol 10–20 mg) should be given as an adjuvant treatment but should not be given as monotherapy due to some hyperkalemia patients being unresponsive to beta-2 agonists.Beta-2 agonists induce a mild hyperglycemic state, so simultaneous administration of beta-2 agonists with IV insulinglucose can achieve better effi cacy and lower the risk of hypoglycemia.However, high doses of beta-2 agonists may cause side effects such as palpitations, tremors,headaches, and angina, particularly in patients with coronary heart disease. Therefore, cardiac monitoring is recommended in HEs, particularly in those patients receiving beta-2 agonists.
Theoretically, infusing sodium bicarbonate elevates blood pH, promotes the movement of hydrogen ions extracellularly, and activates the sodium-hydrogen exchange and Na-K-ATPase, causing potassium to move intracellularly.In clinical practice, however,sodium bicarbonate scarcely lowers serum potassium at all in patients without metabolic acidosis.In patients with metabolic acidosis, the serum potassium lowering eff ect is not apparent until 4–6 h after infusion.Additionally,excessive sodium bicarbonate induces hypernatremia and f luid overload.In conclusion, sodium bicarbonate is not recommended as a sole agent in HEs in the absence of metabolic acidosis.
Removing potassium from the body
—
Loop diuretics increase renal potassium excretion and are particularly beneficial in patients with normal to moderately compromised kidney function or volume overload.Diuretics should be given with caution in hemodynamically unstable patients. Loop diuretics are very effective and can achieve synergistic effects when combined with other diuretics like thiazides.However,diuretics as a monotherapy for HEs are far from enough.
—
Sodium polystyrene sulfate (SPS) is a nonselective potassium binder.SPS has a lot of disadvantages such as uncertain efficacy, risk of hypocalcemia and hypomagnesemia, and significant gastrointestinal adverse effects, life-threatening colonic necrosis, or perforations.SPS is therefore not recommended for HEs unless dialysis or other drugs that remove potassium from the body are ineff ective or not available. SPS 15–60 g can be given orally and may be repeated 4–6 h later, if necessary.Sorbitol is no longer suggested to be given with SPS because it may augment the risk of colonic necrosis and perforations.
Sodium zirconium cyclosilicate (SZC) and patiromer are both novel non-absorbed selective cation exchangers and potassium binders.When hemodialysis is not immediately available, 10 g of SZC three times a day for up to 72 h or 8.4 g of patiromer once daily is recommended alongside standard treatment with insulin-glucose and beta-agonists in HEs, which may theoretically postpone or even avoid dialysis. SZC has a relatively fast onset of action of less than 1 h and is also 25 times more selective than patiromer for potassium and is 9.3 times more effective in lowering serum potassium than SPS.SZC and patiromer have higher tolerability than SPS due to less gastrointestinal sideeffects, although SZC still has some adverse effects like hypertension, sodium overload, and edema.Constipation,diarrhea, and hypomagnesemia are common adverse eff ects of patiromer.
Potassium binders are independent of kidney function and can be prescribed to anuric HE patients.Studies pertaining to the efficacy and safety of potassium binders in lowering serum potassium were overwhelmingly conducted in mild to moderate chronic hyperkalemia patients. More studies related to whether potassium binders are eff ective in acute, high-potassium level HE patients is still needed.
Dialysis is the definitive and the most effective treatment for HEs and the only treatment that achieves normalized serum potassium within 4 h.Rossignol et alsuggested that emergency dialysis should be considered in patients with persistent ECG changes or those with an insufficient response to beta-2 agonists or insulin-glucose, particularly in patients with renal insufficiency. Pirklbauerindicated that emergency blood purification was mandatory whenever acute renal failure presented with severe hyperkalemia due to the impending risk of fatal arrhythmias. However, whether dialysis is performed in HE symptomless patients with chronic kidney disease remains controversy.Notwithstanding its extraordinary capacity to lower serum potassium, dialysis is invasive, costly, and may not immediately be available in the ED.
MONITORING
Frequent monitoring of serum potassium and glucose is necessary for timely treatment adjustments.Medications that lower serum potassium work together most efficiently for about 2 h. A rebound effect due to additional potassium being released from intracellular stores may appear at 2–3 h if further treatments eliminating potassium from the body have not been instituted.Thus, re-evaluation of serum potassium is recommended at 1–2 h after medication administration.
CONCLUSIONS
Timely treatment can avoid life-threatening complications of hyperkalemia. However, treatment of hyperkalemia in the ED is highly variable, and no agreed f lowchart exists because prospective, randomized controlled trials are minimal. Nevertheless, there is widespread agreement on three approaches to treatment:cardiac myocyte protection, shifting serum potassium intracellularly, and removing potassium from the body.Systematic treatment with frequent monitoring and evaluation according to the proposed flowchart might help ED clinicians make quick and reasonable decisions and improve outcomes.
This research received no funding from any funding agency, commercial or not-for-prof it entity.
Not applicable.
Authors have no f inancial or other conf licts of interest related to this submission.
YW proposed the study and wrote the first draft.JX and JHW edited the manuscript. All authors reviewed and approved the f inal version of the manuscript.
 World Journal of Emergency Medicine2022年3期
World Journal of Emergency Medicine2022年3期
- World Journal of Emergency Medicine的其它文章
- Mortality-related electrocardiogram indices in methanol toxicity
- The combination of creatine kinase-myocardial band isoenzyme and point-of-care cardiac troponin/contemporary cardiac troponin for the early diagnosis of acute myocardial infarction
- Increasing angiotensin-converting enzyme (ACE) 2/ACE axes ratio alleviates early pulmonary vascular remodeling in a porcine model of acute pulmonary embolism with cardiac arrest
- Shrinking lung syndrome in autoimmune inflammatory diseases: A case series and review of literature
- Traumatic tension pneumocephalus: A case report
- Blunt myocardial injury and gastrointestinal hemorrhage following Heimlich maneuver: A case report and literature review