
Common carotid artery distortion before percutaneous dilatational tracheostomy
2022-09-17 07:10:08LiwenDuKaiXunLeileiZhuPengLiu
Li-wen Du, Kai Xun, Lei-lei Zhu, Peng Liu
1 Emergency Department, Hwa Mei Hospital, University of Chinese Academy of Sciences, Ningbo 315010, China
2 Ningbo Institute of Life and Health Industry, University of Chinese Academy of Sciences, Ningbo 315010, China
Dear editor,
The neck is rich in blood vessels. Abnormal origins are rarely seen in clinical practice, but some are found accidentally during relevant imaging examinations,autopsy, and surgery. Abnormal neck vessels are mostly asymptomatic; however, approximately 10%of patients with abnormal blood vessels may have clinical manifestations due to the compression of adjacent tissues and organs.The innominate artery is a short artery branching off from the right side of the main arch obliquely to the upper right behind the right sternoclavicular joint; it divides into the right common carotid artery (RCCA) and the right subclavian artery(RSA). Variations in the location and distortions of the innominate artery and its branches are rare. We encountered a case of distortion and malformation of the RCCA resulting in compression of the trachea, as reported by Madan et al.
CASE
A 78-year-old female (body mass index [BMI] 24.9 kg/m) was admitted to our hospital after being found unconscious. The diagnosis was hypoxic ischemic encephalopathy. To clear airway secretions and maintain vital signs, percutaneous dilatational tracheostomy (PDT)was considered. At the site of tracheostomy, pulsation on the cricoid cartilage was evident, and ultrasound was performed immediately. The RCCA was found to run on the right side of the trachea, crossing the trachea anteriorly below the cricoid cartilage and descending posteriorly, as shown in Figure 1. The decision was made to suspend the tracheostomy, and carotid angiography was performed on the same day. The family denied any history of congenital vascular malformation. Combined with the patient’s long history of hypertension and carotid atherosclerosis, the carotid artery was considered to be distorted and deformed. A coronal view revealed that the trachea was shifted to the right, potentially due to traction from surrounding tissues; the innominate artery transversely covered the position between the 1and 2tracheal rings, as shown in Figure 2. The tracheostomy method was changed the next day. After the RCCA was separated under direct vision, tracheostomy was performed, and a tracheal cannula was implanted. The whole operation was carried out under electrocardiogram(ECG), blood pressure and blood oxygen saturation monitoring, and there was no obvious bleeding during or after the operation. Later, the patient was successfully weaned off the ventilator and transferred out of the emergency intensive care unit (EICU). Ultimately,the patient’s family could not afford the expensive rehabilitation treatment and abandoned treatment.
DISCUSSION
The great vessels of the human head and neck include the aortic arch, the brachiocephalic trunk (BCT),the left common carotid artery (LCCA) and RCCA, the left and right vertebral arteries, and the left subclavian artery (LSA) and RSA. The aortic arch is one of the three thoracic segments of the aorta and the only segment located in the superior mediastinum (SM). The arch begins with the aorta rising from the pericardium and passing upward, backward, and left across the SM and ends at the level of the T4-T5 vertebrae. Three branches arise from the upper boundary of the artery: the BCT,the LCCA, and the LSA. The BCT divides into the RCCA and the RSA.However, it has been reported in the literature that cervical vascular variations and distortions are more common on the left side, with abnormalities on the right side of the neck accounting for less than 1% of the total.In addition, a study of 556 patients with thoracic aortic disease showed that 33.5%(186 patients) demonstrated anomalies of the aortic arch, 6.3% (35 patients) had an isolated left vertebral artery, and 1.8% (10 patients) had an aberrant RSA.PDT is currently an important means of clinical rescue.Although the curative effect is exact and the technique is mature, hemorrhage is a serious complication after this operation. The literature indicates that the mortality rate due to hemorrhage after tracheostomy is high, especially innominate artery hemorrhage, with a mortality rate of 90%.Thus, appropriate indications are required for tracheostomy.Based on the literature and clinical experience, the emergency unit of our institution requires all patients intended to be treated with PDT to undergo a preincision evaluation, except in extreme cases where cricothyroid tracheostomy may be necessary.In cases of BMI 28 kg/m, vague anatomical landmarks(brevicollis, giant thyroid, after surgery or radiotherapy),neck instability or infection, and hypocoagulability,physicians and surgeons need to decide together whether the patient would benefit from tracheostomy and which technique would be the most suitable. An uncorrected bleeding disorder (platelet count <50,000/mmand/or international normalized ratio >1.5 and/or partial thromboplastin time >2 normal) is an absolute contraindication to all surgical procedures.We require an ultrasound examination before PDT because it helps identify abnormal blood vessels, and ultrasound during PDT helps prevent tracheal misalignment.This requirement is based on four open randomized studies in a total of 560 patients. We typically used a single dilator in our PDT technique,as this method causes the least bleeding among all methods and tools for PDT (multiple dilator, guide wire dilating forceps, single dilator,rotating dilation, and balloon dilation).
CONCLUSIONS
The incidence of cervical vascular variation is not high in clinical practice, but carelessness during tracheostomy may lead to serious complications and irreparable consequences. PDT can be performed quickly and safely at the bedside with the use of a modified Seldinger technique and bronchoscopic guidance.Compared with the open tracheostomy, this approach is associated with fewer bleeding complications, a shorter operation time, and a decreased incidence of stoma infection and inflammation, but a similar long-term morbidity rate.While performing tracheostomy early or late does not aff ect the prognosis, early tracheostomy seems to reduce the consumption of hypnotic drugs. At our institution, early tracheostomy (after the fourth day of mechanical ventilation) is performed for patients with severe cerebrovascular disease. Therefore, fundamental measures to prevent complications of tracheostomy include standardizing the evaluation and manipulation of the trachea before tracheostomy and strengthening observation and nursing practices after tracheostomy.Based on the treatment involved and summary of this case, we provide a basis for the clinical response to similar cases.
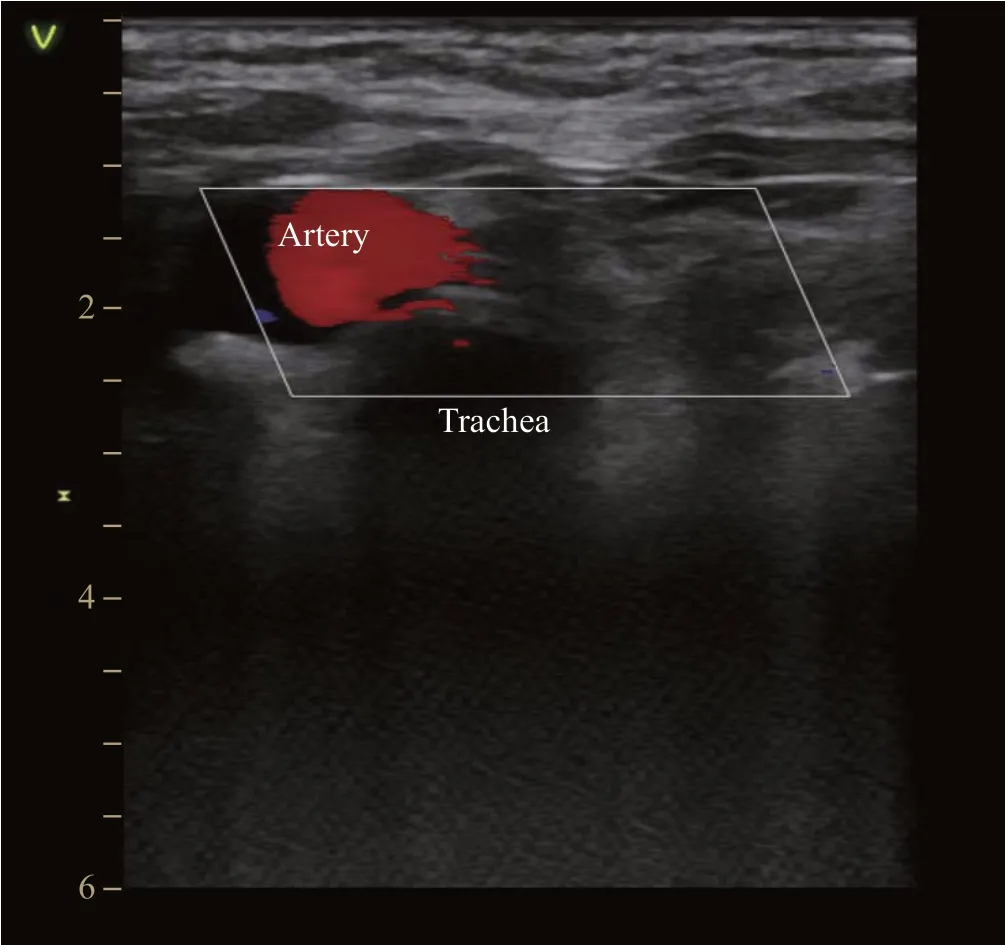
Figure 1. The ultrasound image of the patient. The right common carotid artery found to run on the right side of the trachea.
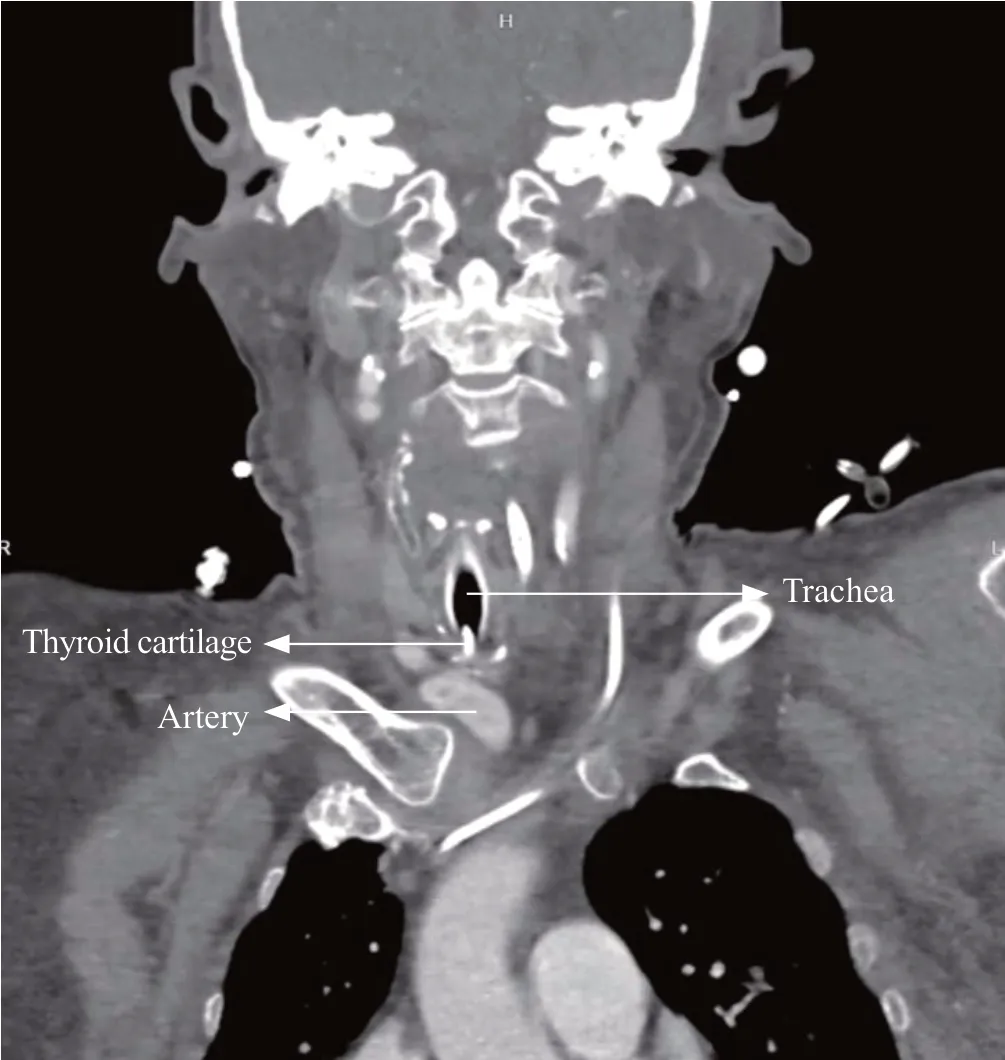
Figure 2. The carotid angiography image of the patient. The innominate artery transversely covered the position between the 1st and 2nd tracheal rings.
This research was supported by grants from the Research Foundation of Hwa Mei Hospital, University of Chinese Academy of Sciences, China (2020HMKY22); the Zhejiang Medicine and Health Science and Technology Project (2021424731); and Ningbo Medical Key Discipline (2022-F16).
The study was approved by the Ethics Committee of Hwa Mei Hospital. Informed written consent was obtained from the patient’s legal representative for publication of this report and any accompanying images.
The authors have no conf licts of interest.
LWD wrote the study. All authors have made substantial contributions to the acquisition, analysis, or interpretation of data for the work and drafting the work or revising it critically for important intellectual content, and provided final approval of the version to be published.
 World Journal of Emergency Medicine2022年3期
World Journal of Emergency Medicine2022年3期
- World Journal of Emergency Medicine的其它文章
- Mortality-related electrocardiogram indices in methanol toxicity
- The combination of creatine kinase-myocardial band isoenzyme and point-of-care cardiac troponin/contemporary cardiac troponin for the early diagnosis of acute myocardial infarction
- Increasing angiotensin-converting enzyme (ACE) 2/ACE axes ratio alleviates early pulmonary vascular remodeling in a porcine model of acute pulmonary embolism with cardiac arrest
- Shrinking lung syndrome in autoimmune inflammatory diseases: A case series and review of literature
- Traumatic tension pneumocephalus: A case report
- Blunt myocardial injury and gastrointestinal hemorrhage following Heimlich maneuver: A case report and literature review