
Corpus callosum agenesis: Role of fetal magnetic resonance imaging
2016-11-30 12:33:57AchourRadhouaneNejiKhaled
Achour Radhouane, Neji Khaled
Emergency Department of Maternity and Neonatology Center, Faculty of Medicine of Tunis, Tunis, Tunisia
Corpus callosum agenesis: Role of fetal magnetic resonance imaging
Achour Radhouane*, Neji Khaled
Emergency Department of Maternity and Neonatology Center, Faculty of Medicine of Tunis, Tunis, Tunisia
ARTICLE INFO
Article history:
Received
Received in revised form
Accepted
Available online
Corpus callosum agenesis
Corpus callosum agenesis (CCA) was evaluated by ultrasound examination and magnetic resonance imaging (MRI) with many studies. Ultrasonography was able to suspect CCA by indirect signs but a definitive diagnosis of CCA was achieved in rare cases. MRI was able to diagnose complete CCA in majority of cases. Additional neurological abnormalities including heterotopia, gyration anomaly, asymmetry of the cerebral hemispheres, and Dandy-Walker variant were documented, as well as an ocular anomaly which was described, by MRI examination. Prenatal counseling for fetal agenesis of the corpus callosum is difficult as the prognosis is uncertain. The association with other cerebral abnormalities increases the likelihood of a poor outcome and ultrasonographic assessment of the fetal brain is limited. We found MRI to be a safe and useful additional procedure to complement ultrasonographic diagnosis or suspicion of CCA.
1. Introduction
The corpus callosum is the most important cerebral commissure allowing axonal fibers to cross the midline. Corpus callosum agenesis (CCA) is an important condition in man that can reveal numerous genetic syndromes. The corpus callosum develops from the commissural plate, a dorsal region of the telencephalon. Then, axons growing from pyramidal neurons of cortical layer III extend and cross the midline.
Predicting CCA remains dubious and debate continues on the issue. The only prognostic indicator which currently can be confi rmed with acceptable reliability is whether CCA is isolated or not. Most studies have found that prognosis is generally unfavorable in the event CCA with retarded psychomotor development or epilepsy. The character partial or complete nature of the agenesis does not seem to infl uence prognosis signifi cantly. Antenatal diagnosis is based on fetal ultrasound, however magnetic resonance imaging (MRI) enables a finer search for associated brain malformations, and in particular neuronal migration anomalies.
2. Case report
We report a case of diagnosis of isolated fetal CCA. No consanguineous parents. We released a fetal MRI who is a specific imaging modality, always performed after a reference ultrasound examination. MR improves prognosis evaluation, since it enables depiction of no associated abnormalities, notably gyral abnormalities, posterior fossa malformations, and intra-cranial cysts. In our case MRI was confi rmed isolated fetal CCA (Figure 1). Caesarean section was performed at 38 weeks gestation. A healthy male baby weighing 3 400 g was safely delivered.
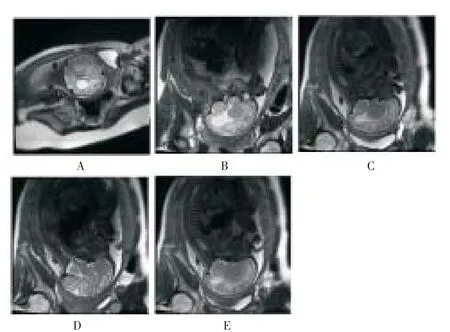
Figure 1. Isolated fetal corpus callosum agenesis.
3. Discussion
The corpus callosum, a forebrain commissure, originates from the primitive lamina terminals. The fi rst callosal fi bers form by day 74 of gestation and formation of corpus callosum is complete by 115 d; however, the process of myelination continues after birth. The extent of malformation varies from partial to complete agenesis. In partial agenesis, the posterior part is not developed because the corpus callosum develops in an antero posterior direction. However, cases of anterior agenesis have also been reported[1]. In CCA, the lateral ventricles are shifted laterally and the 3rd ventricle is enlarged and displaced superiorly with its roof extending dorsally. CCA could be an isolated anomaly or associated with abnormalities in other parts of the brain like heterotopias, microgyria, abnormal cerebral fi ssures, porencephalic cysts and hydrocephalus.
Callosal agenesis has been reported by several authors. Grogono[2] reported 0.7% of CCA in a large series while Jeret et al.[3]came across 33 cases of CCA in a series of 1 447 CT scans of brain. Epidemiological surveys have approximately estimated the prevalence of CCA as 1 in 20 000 individuals[4].
The aetiology is multifactorial but in most of the cases, the cause is unknown. Genetic factors, toxic eff ects of alcohol on the fetus, endogenous toxins leading to lactic acidosis, vascular and metabolic defects and various congenital infections have been found to be closely associated with the aetiology of CCA[5].
Various chromosomal defects including trisomies have been reported in medical literature with CCA. Serur et al. reviewed 81 cases of CCA from medical literature, of which 21 had trisomy, 14 had trisomy and 18 had aberrations of chromosomes[6].
Antenatal diagnosis is possible from 20 weeks of gestation. A decision to terminate is diffi cult to take without reservation until more is known about the incidence of asymptomatic cases. Blum et al. reported that six of twelve infants with antenatally diagnosed callosal agenesis had a normal development at 2–8 years of age[7]. Infants with associated manifestations or chromosomal anomalies had a poor outcome. Fetal karyotyping, looking for associated anomalies and thorough antenatal sonographic examination of the foetus may be of immense help in deciding to terminate pregnancy. The diagnosis of CCA rests on neuro imaging; cranial ultrasonography in infancy and MRI of the brain in later years. The latter technique is far superior for the diagnosis of partial agenesis, while cranial ultrasonography serves as an easy alternative for the diagnosis of complete agenesis[8]. In our experience, the radiological diagnosis of CCA has been mostly coincidental, hence neuroradiological imaging remains an absolutely essential investigation of developmental delay[5].
We found MRI to be a safe and useful additional procedure to complement ultrasonographic diagnosis or suspicion of CCA. Prenatal MRI is a valuable complementary technique for either diagnosis of CCA and depiction of associated neurologic abnormalities. In light of results and data reported in the literature, MRI appears to be an essential and reliable complement to fetal ultrasound in the event of suspected complete or partial agenesia of the corpus callosum and to search for associated malformations. Antenatal counseling in the event of diagnosis of agenesis of the corpus callosum is diffi cult because the individual prognosis remains poor.
Declare of interest statement
The authors declare that they have no confl ict of interest.
[1] Aicardi J, Chevrie JJ, Baraton J. Agenesis of Corpus Callosum. In: Vinken PJ, Bruyen GW, Klawans HL, editors. Handbook of Clinical Neurology. Revised series. Brain malformations. Amsterdam: North Holland; 1987: 149-173.
[2] Grogono JL. Children with agenesis of corpus callosum. Dev Med Child Neurol 1968; 10: 613-616.
[3] Jeret JS, Serur D, Wisniewski K, Fish C. Frequency of agenesis of the corpus callosum in the developmental disabled population as determined by CT Brain. Pediatr Neurosci 1985-86; 12: 1001-1003.
[4] Jones K, Smith DW, Ulleland C, Stressguth AP. Pattern of malformations in off spring of chronic alcoholic mothers. Lancet 1973; 1: 1267-1271.
[5] Chacko A, Koul R, Sankhla DK. Corpus callosum agenesis. Neurosciences 2001; 6(1): 63-66.
[6] Serur D, Jeret JS, Wisniewski K. Agenesis of the corpus callosum: Clinical, neuro radiological and cytogenetic studies. Neuropediatrics 1988; 19: 87-91.
[7] Blum A, Andre M, Broulle P, Husson S, Leheup B. Prenatal echographic diagnosis of corpus callosum agenesis: The Nancy experience 1982-1989. Genetic Counseling 1990; 38: 115-126.
[8] Atlas SW, Zimmerman RA, Bilaniuk LT. Corpus callosum and limbic system: Neuroanatomic MR evaluation of developmental anomalies. Radiology 1986; 160: 355-362.
ent heading
10.1016/j.apjr.2016.03.004
*Corresponding author: Achour Radhouane, Emergency Department of Maternity and Neonatology Center, Faculty of Medicine of Tunis, Tunis, Tunisia.
Tel: +21698549398
E-mail: radhouane.a@live.com
Fetal
Magnetic resonance imaging Prognosis
 Asian Pacific Journal of Reproduction2016年3期
Asian Pacific Journal of Reproduction2016年3期
- Asian Pacific Journal of Reproduction的其它文章
- A rare cause of infertility: A late complication of female genital mutilation
- Chilled and post-thawed semen characteristics of buffalo semen diluted in tris extender enriched with date palm pollen grains (TPG)
- Establishment, characterization and cryopreservation of Fars native goat fetal fibroblast cell lines
- Somatic embryogenesis and in vitro flowering in Hybanthus enneaspermus (L.) F. Muell.-a rare multipotent herb
- Pollutant exposure in Manila Bay: Effects on the allometry and histological structures of Perna viridis (Linn.)
- Changes in sperm characteristics of the three main breeds of sheep in Algeria after dietary supplementation