
Application of fluorescence in situ hybridization in the detection of bladder transitional-cell carcinoma:A multi-center clinical study based on Chinese population☆
2019-04-10 06:56:40KaYaXLYDDaHaYaWaJaGaMaYaXaZaJaQaXbZcGaDaGaYaJaGaGaWaYaXaJaJaFaYaQaJaSaJaHaTaXaKaLaQaBaSaZaLaWaWaWbLc
Asian Journal of Urology 2019年1期
L Z*,Ka YaX LY DDa M,Ha L,Y Ya,J L,D Wa,W L,Y C,Ja Ga,K Ma,Ya Xa,S Za,H Ja,W H,Qa W,Xb J,Zc Ga,Q L,Da X,X Ga,Ya Ja,W Ga,Ga S,Q Wa,Ya L,J H,L X,Xa S,F Ja,Ja Fa,M C,Z L,J Z,D Ya,L Qa,L M,Ja Sa,Y D,Ja S,Y T,S Ha,Ta Xa,C Ka,Z K,Y La,X Qa,Ba Sa,S Za,Y La,S X,D Wa,J Wa,W F,Z Wb,J Lc
aDepartment of Urology,Peking University First Hospital,Beijing,China
bInstitute of Urology,Peking University,Beijing,China
cNational Urological Cancer Center,Beijing,China
dAir Force General Hospital,PLA,Beijing,China
eDepartment of Urology,Peking Union Medical College Hospital,Beijing,China
fDepartment of Urology,Beijing Chao-Yang Hospital,Beijing,China
gDepartment of Urology,Armed-Police General Hospital,Beijing,China
hDepartment of Urology,Shanxi Medical University First Hospital,Taiyuan,China
iDepartment of Urology,Hebei Medical University Second Hospital,Shijiazhuang,China
jDepartment of Urology,The General Hospital of the People’s Liberation Army,Beijing,China
kDepartment of Urology,First Af filiated Hospital of Jilin University,Changchun,China
lDepartment of Urology,Union Hospital,Tongji Medical College,Huazhong University of Science and Technology,Wuhan,China
mDepartment of Pathology,The First Af filiated Hospital of Fujian Medical University,Fuzhou,China
nDepartment of Urology,The Second Xiangya Hospital of Central South University,Changsha,China
oDepartment of Urology,General Hospital of Guangzhou Military Command of PLA,Guangzhou,China
pDepartment of Urology,West China School of Medicine,Chengdu,China
qDepartment of Urology,Shangdong Province-owned Hospital,Jinan,China
rDepartment of Urology,Peking University Shenzhen Hospital,Shenzhen,China
sDepartment of Urology,The Central Hospital of Jinan City,Jinan,China
tDepartment of Urology,Shanghai Changzheng Hospital,Shanghai,China
uDepartment of Urology,The Third Af filiated Hospital of Sun Yat-sen University,Guangzhou,China
vDepartment of Urology,Beijing Anzhen Hospital of Capital Medical University,Beijing,China
wDepartment of Urology,The Second Af filiated Hospital of Xi’an Jiaotong University,Xi’an,China
xDepartment of Urology,The Second Hospital of Tianjin Medical University,Tianjin,China
yDepartment of Urology,People’s Hospital of Xinjiang Uygur Autonomous Region,Wulumuqi,China
zDepartment of Urology,Guangdong General Hospital,Guangzhou,China
aaDepartment of Urology,The First Af filiated Hospital of Soochow University,Suzhou,China
abDepartment of Urology,The First Hospital of Zhejiang Province,Hangzhou,China
acDepartment of Urology,The First Af filiated Hospital of Dalian Medical University,Dalian,China
adDepartment of Urology,Daping Hospital,Research Institute of Surgery,Third Military Medical University,Chongqing,China
aeDepartment of Urology,Mianyang Central Hospital,Mianyang,China
afDepartment of Urology,General Hospital of PLA General Staff Headquarters,Beijing,China
agDepartment of Urology,First Af filiated Hospital of Anhui Medical University,Hefei,China
ahDepartment of Urology,Renmin Hospital of Wuhan University,Wuhan,China
aiDepartment of Urology,Fudan University Shanghai Cancer Center,Shanghai,China
ajDepartment of Urology,Xiangya Hospital of Central South University,Changsha,China
akDepartment of Urology,Peking University Third Hospital,Beijing,China
alDepartment of Urology,Cancer Hospital of Chinese Academy of Medical Sciences,Beijing,China
amDepartment of Urology,The First Af filiated Hospital of Sun Yat-sen University,Guangzhou,China
anDepartment of Urology,Sun Yat-sen University Cancer Center,Guangzhou,China
aoDepartment of Urology,Beijing Friendship Hospital of Capital Medical University,Beijing,China
apDepartment of Urology,Wenzhou Central Hospital,Wenzhou,China
aqDepartment of Urology,Peking University People’s Hospital,Beijing,China
arDepartment of Urology,The First Hospital of China Medical University,Shenyang,China
asDepartment of Urology,Qinghai Province People’s Hospital,Xining,China
atDepartment of Urology,Beijing Tongren Hospital of Capital Medical University,Beijing,China
auDepartment of Urology,Qilu Hospital of Shandong University,Jinan,China
avDepartment of Urology,Nanfang Hospital,Southern Medical University,Guangzhou,China
awDepartment of Urology,Tianjing Medical University General Hospital,Tianjin,China
axDepartment of Urology,Shanghai General Hospital,Shanghai,China
ayDepartment of Urology,Beijing Hospital,Beijing,China
azDepartment of Urology,The First Af filiated Hospital of Wenzhou Medical University,Wenzhou,China
baDepartment of Urology,Southwest Hospital,Chongqing,China
bbDepartment of Urology,Lanzhou University Second Hospital,Lanzhou,China
bcDepartment of Urology,The People’s Hospital of Guangxi Zhuang Autonomous Region,Nanning,China
KEYWORDS Bladder transitionalcell carcinoma;Fluorescence in situ hybridization;Detection;Grade;Stage
Abstract Objective:To evaluate the diagnostic value of fluorescence in situ hybridization(FISH)in bladder cancer.Methods:We enrolled healthy volunteers and patients who were clinically suspected to have bladder cancer and conducted FISH tests and cytology examinations from August 2007 to December 2008.Receiver operating characteristic(ROC)curve analysis was performed and the area under curve(AUC)values were calculated for both the FISH and urine cytology tests.Results:A cohort of 988 healthy volunteers was enrolled to establish a reference range for the normal population.A total of 4807 patients with hematuria were prospectively,randomly enrolled for the simultaneous analysis of urine cytology,FISH testing,and a final diagnosis as determined by the pathologic findings of a biopsy or a surgically-excised specimen.Overall,the sensitivity of FISH in detecting transitional-cell carcinoma was 82.7%,while that of cytology was 33.4%(p<0.001).The sensitivity values of FISH for non-muscle invasive and muscle invasive bladder transitional-cell carcinoma were 81.7%and 89.6%,respectively(p=0.004).The sensitivity values of FISH for low and high grade bladder cancer were 82.6%and 90.1%,respectively(p=0.002).Conclusion:FISH is significantly more sensitive than voided urine cytology for detecting bladder cancer in patients evaluated for gross hematuria at all cancer grades and stages.Higher sensitivity using FISH was obtained in high grade and muscle invasive tumors.
1.Introduction
Bladder cancer(BC)is the second most common malignancy of the urinary tract[1].More than 70%of BC patients have super ficial disease at initial diagnosis,whereas 30%have already advanced to the muscle-invasive stage.Early diagnosis of BC is essential to prevent progression of Ta and T1 tumors to the muscle-invasive stage.Although nonmuscle invasive transitional-cell carcinoma can be treated by transurethral resection(TUR),the 5-year and 15-year recurrence rates are 70% and 90%,respectively,and approximately 15%-25%of the recurrent tumors progress to high grade or muscle invasive disease[2,3].Early diagnosis,appropriate treatment and proper surveillance are thought to be important parts of therapy.
Cystoscopy remains the gold standard for patients in whom BC is suspected.However,it is unacceptable for a considerable number of patients,which lowers the surveillance compliance.Cytology remains the gold standard of non-invasive methods to detect BC,but it has poor sensitivity.Therefore,new methods are needed for the early detection of BC.
Early studies demonstrated that fluorescence in situ hybridization(FISH)analysis for aneuploidy of specific chromosomes and loci might be useful to screen urine or bladder washings for early tumor detection or recurrence[4-10].Therefore,FISH to detect urinary exfoliated cells with these genetic alterations has been tested and used in Europe and the United States.However,the reliability of FISH tests has not been verified in the Chinese population,and differing geographic locations may result in genetic discrepancies when Chinese patients are compared with a western population.Therefore,it is necessary to explore the genetic alterations of BC within the Chinese population.We report the results of a multicenter trial performed to assess the ability of the FISH test to detect BC in voided urine in patients with gross hematuria with or without a history of BC.
2.Patients and methods
2.1.Patients
The Chinese Ministry of Health organized a national investigation and enrolled more than 52 tertiary hospitals.Between January 2007 and June 2007,a total of 988 healthy volunteers(We enrolled 20 cases from each hospital.After analysis,we excluded invalid results,leaving only 988 samples for final analysis)were enrolled in this study.All volunteers had signed consent forms to authorize the analysis of their medical records.Institutional review board approval for the study was obtained form each center.Within these volunteers,495 cases were male,aged 32-67 years,and 493 were female,aged 37-56 years.Exfoliated cells from urine samples of these volunteers were used to establish normal population thresholds for the FISH testing used in this study.
Between August 2007 and December 2008,4807 patients with hematuria who were suspected of transitional cell tumors by B-mode ultrasound were randomly enrolled in this trial.The patient group was comprised of men and women(63.04±13.31 years old[mean±SD],range 15-97 years).Simultaneous analyses of urine cytology and FISH testing were performed before patients underwent cystoscopy with biopsy(If there was any invisible tumor,we did a tumor biopsy;if there wasn’t,we did a randomized biopsy of the whole bladder)followed by computed tomography(CT)or magnetic resonance imaging(MRI)scan of the upper urinary tract.For the patients with suspicious tumors,proper treatment was provided,including transurethral resection of bladder tumor(TUR-Bt),transurethral resection of prostate(TUR-P),radical cystectomy,radical nephrectomy and nephroureterectomy.
2.2.FISH
The FISH DNA probes were provided by Beijing Golden Bodhisattva Kar Medical Technology Co.,Ltd.The probe consists of two combinations,namely the CSP3(red)/CSP7(green)and the GLP p16(red)/CSP17(green)probe combinations.
2.2.1.Sample processing
Urine samples of at least 200 mL in volume were collected during out-patient visits and divided into two equal parts for FISH and cytology.The cytology and pathology analyses were performed by two specialists.For FISH detection,the 100 mL urine sample was centrifuged at 2 000 rpm for 10 min.Then,the supernatant was removed,and the pellet was re-suspended with collagenase B before incubation in a 37°C water bath for 20 min.The sample was then centrifuged at 1 000 rpm for 10 min,the supernatant was removed,and the cells were re-suspended in a 0.075 mol/L KCl hypotonic solution before incubation in a 37°C water bath for 20 min.The cells werefixed twice by the addition of 2 mL fixative solution(methanol:glacial acetic acid 3:1)before centrifugation for 10 min and were transferred to a glass slide followed by aging.The slides were then treated with RNase A and pepsin,followed by rinsing in a 2×saline sodium citrate(SSC)(pH 7.0)solution and gradient dehydration in 70%,85%and 100%ethanol that had been precooled at-20°C for 2 min.
2.2.2.FISH
The combined FISH probes CSP3/CSP7 and GLP p16/CSP17 were used in this experiment.The CSP3 and GLP p16 probes were marked by the tetramethyl rhodamine with a red fluorescence signal,while the CSP7 and CSP17 probes were marked by green fluorescence.The slides were prepared by soaking in 73°C ± 1°C denaturation solution for 5 min,followed by gradient dehydration in 70%ethanol,85%ethanol and 100%ethanol(-20°C)for 3 min.After natural drying,the slides were placed in a 45°C-50°C hybridization oven for 2-5 min.The probe mixtures were prepared by mixing 7 μL of hybridization buffer,1 μL of deionized water,and 2 μL of the appropriate probe in a microcentrifuge tube at room temperature.The FISH probes were denatured at 73°C ± 1°C in a water bath for 5 min and stored in a 45°C-50°C water bath until the hybridization was performed.A total of 10 μL of the denatured probe mixture was applied on top of the hybridization mixture on each slide.The slides were immediately covered with a coverslip and sealed with rubber cement before incubation in a wet slide box at 42°C overnight.The slides were washed immediately in 46°C ± 1°C 50%formamide/2× SSC solution,2× SSC solution,and 2× SSC/0.1%NP-40 solution,and then soaked in 70%ethanol in a dark box for drying.The slides were then counter-stained with 15 μL of DAPI solution.After 10-20 min in the dark room,the fluorescence signals were assessed by microscopy and images were recorded.
2.2.3.Threshold standards
In each case,atypical cellular nuclei as well as aneuploidies of chromosomes 3,7,or 17 were counted using fluorescent microscopy.The number and frequency of cells missing p16 loci was calculated by the following equation to establish normal thresholds:Threshold value=mean+3 SD.
2.2.4.Evaluation of results
In normal cells,the CSP3,CSP7,and CSP17 centromere probes and the GLP p16 locus probe always detected a diploid state by the presence of two green and two red signals in the nucleus.The absence of a diploid signal indicated an abnormal cell.Aneuploidies of chromosomes 3,7,or 17 appeared as multiple signals with the nucleus whereas a missing p16 site presented as less than two fluorescent signals in the nucleus.One hundred different cells were counted from every healthy volunteer sample,and the frequency of aneuploidies on chromosomes 3,7,and 17 as well as the number of cells missing p16 were calculated to establish the normal threshold.When the frequency of aneuploidies on chromosomes 3,7,or 17 or the frequency of cells lacking p16 was greater than the threshold value,the sample was deemed abnormal.When the patients had at least two types of abnormal results with these probe signals,a diagnosis of bladder urothelial carcinoma was issued.
2.3.Cytology
After the FISH assay,a 50 mL urine specimen each time was centrifuged at 2 000 rpm for 10 min.Cells were collected using the procedures described above and were then applied to glass slides for natural drying followed by 95%ethanol fixation and H-E staining by professional pathologists.The final result was a combination of the 100 mL sample.
2.4.Statistical analysis
SPSS 19.0 statistical software for Windows(SPSS,Chicago,IL,USA)was used for statistical analysis.Receiver operating characteristic(ROC)curve analysis was performed,and area under curve(AUC)values were compared between groups;the Chi-squared test was used to determine statistical significance between groups(p<0.05 was considered statistically significant).
3.Results
A total of 4 807 people with gross hematuria provided informed consents and were enrolled in this trial.Of the total subjects,4 688 completed both tests and valid results were obtained from 4 125.Of these 4 125 patients,those who had suspicious upper tract masses or complicated cystoscopy examinations were excluded,leaving 3 959 patients with valid pathologic diagnosis for analysis.These patients included 3 021 males and 938 females,aged 15-97 years(mean 63.04±13.31 years).Due to the large number of biopsy specimens,only 979 patients were randomly selected for central analysis staging and grading(Fig.1).
The p16 chromosomal loci were completely missing in 1 270(30.8%)of cases,partially missing in 1 873(45.4%)cases,and p16 chromosomal loci were missing in three or more locations in 1 592(38.6%)cases.Overall,p16 locus chromosome abnormalities were noted in 3 007(72.9%)of all cases.Chromosomes 3,7,or 17 were deleted in 817(19.8%),878(21.3%),and 945(22.9%)cases,respectively.Chromosomes 3,7,or 17 were doubled in 2 677(64.9%),2 673(64.8%),and 2 450(59.4%)cases,respectively.Abnormalities on chromosomes 3,7,or 17 were detected in 2 941(71.3%),2 978(72.2%)and 2 780(67.4%)cases,respectively.
Of all of the 3 959 patients for whom a FISH test,cytology analysis and pathologic cystoscopy diagnosis were completed,3 640 patients were diagnosed with transitional cell BC,and of these,correct diagnoses(true positive)were made by FISH and cytology in 3 011 and 1 217 cases,respectively.Non-BC diagnoses were made in 319 patients and included in flammation,renal tumor,benign bladder tumor and bladder tumor with a non-transitional cell origin.Correct diagnoses(true negatives)were made by FISH and cytology in 265 and 299 cases,respectively(Table 1).
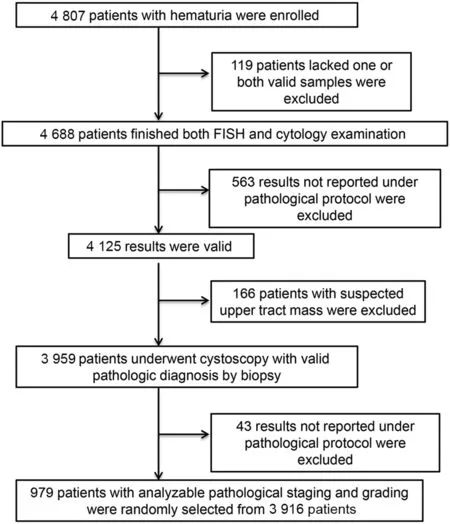
Figure 1 Work flow for patient FISH and cytology.FISH,fluorescence in situ hybridization.
Table 2 displayed the comparison of FISH test and cytology results in the diagnosis of all transitional cell BC.The sensitivities of FISH and cytology were 82.7%and 33.4%,respectively(p<0.001).The specificity values of FISH and cytology were 83.1%and 93.7%,respectively(p<0.001).ROC curve analysis was performed and AUC values were calculated.The AUC values were 0.829 and 0.636 for FISH and cytology,respectively(p<0.001).The positive predictive values for FISH and cytology were 98.2%and 98.4%,respectively(Table 2).
Of the 983 patients with analyzable pathologic information,855 had transitional cell BC.Within this subset of patients,there werefive Tis tumors,254 Ta tumors,336 T1 tumors,184 T2 tumors,56 T3 tumors and 20 T4 tumors.Thus,595 patients had non-muscle invasive cancers and 260had invasive cancers.The FISH test was able to identify 81.7%of the non-muscle invasive cancers and 89.6%of the invasive cancers(p=0.004),while cytology results could be used to identify 22.9%and 39.6%of the invasive cancers,respectively(p<0.001).Low grade tumors were present in 532 patients,and high grade tumors were present in 323 patients.The results from the FISH tests were used to identify 82.5%of the low grade cancers and 90.1%of the high grade cancers(p=0.003),while cytology results were used to identify 21.8%and 42.4%of the low and high grade tumors,respectively(p<0.001)(Table 3).
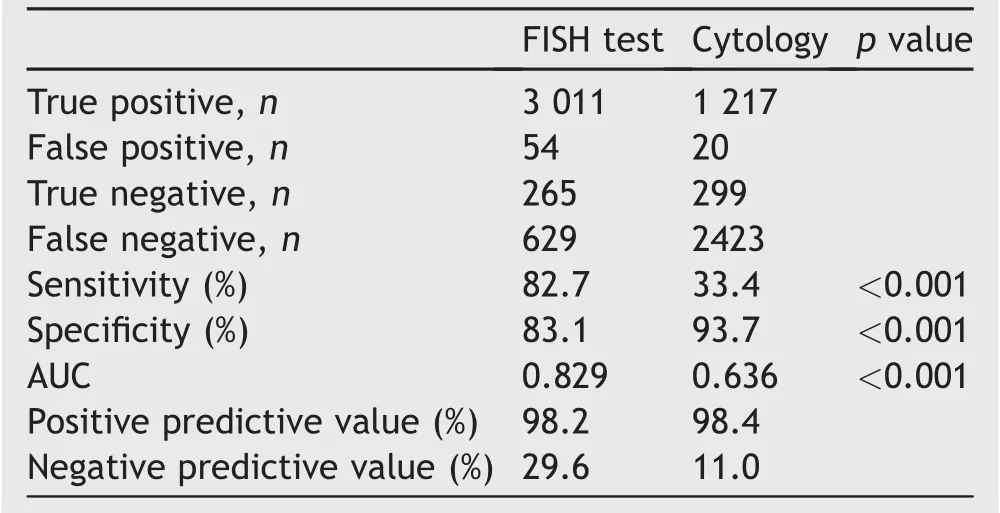
Table 2 Comparison of FISH test and cytology in the diagnosis of all bladder transitional cell cancer(n=3 959).
Table 4 shows the sensitivity and specificity of the FISH test and cytology in patients with or without a history of transitional cell carcinoma in any site.The sensitivity values of FISH for previous transitional cell carcinoma patients and primary hematuria patients were 84.38%and 85.76%,respectively(p=0.655)and those for cytology were 31.29%and 28.18%,respectively(p=0.430).The specificity values for FISH were 50%and 77.5%,while these values were 100%and 90%for cytology,respectively.
4.Discussion
Conventional urine cytology remains the most commonly used method in association with cystoscopy for the diagnosis of new BC and its recurrences;however,the limited sensitivity of this approach has prompted the search for newdiagnostic techniques[11].Various new alternative laboratory tests based on the detection of different substances,such as BTA stat,BTA TRAK,NMP22,telomerases,and fibrinogen degradation products have become available for the diagnosis of BC[12].However,the unsatisfactory specificities reported to date in comparison with urine cytology have limited the clinical utility of these assays,possibly forscreening and surveillance only[13-16].Some other trails had proved FISH to be a more accurate tool in detecting and predicting recurrence for urothelial carcinoma patients[17-19].
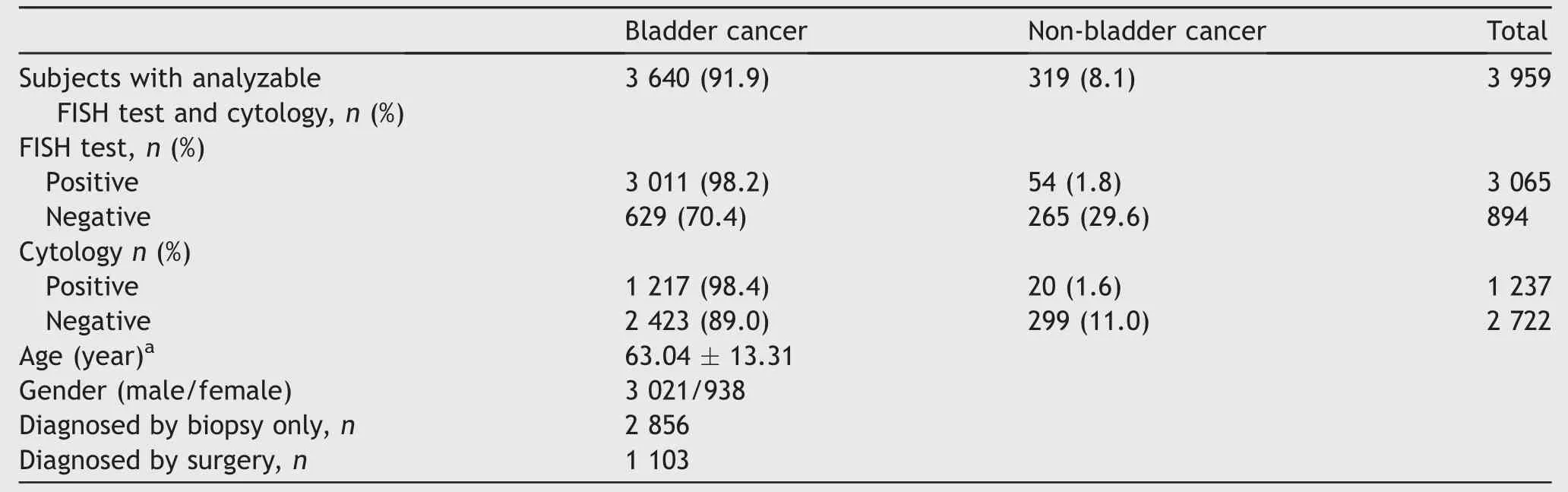
Table 1 Characteristics of the cohort that presented with hematuria.
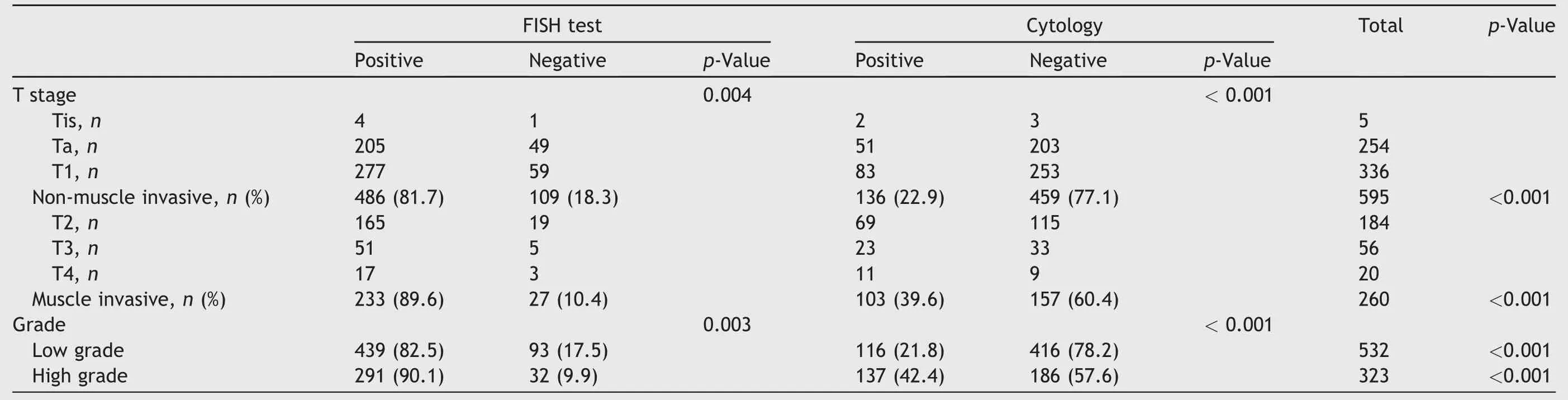
Table 3 Characteristics of all patients with valid pathological diagnoses (n = 855).
Cystoscopy is presently the standard examination by which patients can be accurately diagnosed and monitored,and none of the laboratory tests developed have been able to replace it in the primary detection of the BC.
In thismulticenterstudy,the combination of centromeric probes for chromosomes 3,7,and 17 along with p16 site-specific probes was used to detect chromosomal abnormalities in urine exfoliated cells.Previous studies based on western population showed that FISH might be a promising tool in detecting,surveillance and even predicting,but still the conclusions were controversial[20-27].Also many studies proved FISH to be of good sensitivity and specificity in the detection of upper urinary transitional-cell cancer[28,29].Our study was the first multicenter study in China.Our results showed that genetic alterations in chromosomes 3,7,or 17 or p16 loci in cancer patients accounted for 71.3%,72.2%,67.4%and 72.9%of cases,respectively.As the results showed,this combination was consistent with the genetic changes reported in Chinese BC patients.
Overall,FISH had a sensitivity of 82.7%and an AUC of 0.829 while cytology had a sensitivity of 33.4%and an AUC of 0.636;both the sensitivity and the AUC values between FISH and cytology were significantly different.Although cytology had better specificity than that of FISH,we observed in our study that two patients had negative cystoscopy results but positive FISH test results(false positive)after 4 months and 6 months,respectively.Repeat cystoscopic biopsies confirmed BC in these patients.This result might due to Sarosdy’s proposal that FISH can detect chromosomal changes that begin before morphological changes[30].According to previous studies,FISH possesses the potential to predict UC development since patients with “false” positive FISH at the initial assessment commonly develop UC within 15-22 months,and a preceding positive FISH result is associated with tumor relapse in 86%of UC surveillance cases,including all high-grade recurrences.But unfortunately our study did not do further follow-up with those false positive patients[31-33].Therefore,close monitoring of “false positive” patients with hematuria may be necessary.This may lead to a possible screening method to identify high risk patients or provide surveillance of BC patients.
For non-muscle invasive BC and invasive BC,the sensitivities for FISH were 81.7%and 89.6%,respectively(p=0.004),and those for cytology were 22.9%and 39.6%,respectively(p<0.001).In cases of more aggressive disease,both tests showed better diagnostic value and FISH showed higher sensitivity.For low grade and high grade tumors,the sensitivities of the FISH test were 82.5%and90.1%,respectively(p=0.003),while the sensitivities of cytology were 21.8%and 42.4%,respectively(p<0.001).Both tests showed better diagnostic value in high grade tumors.The above results indicated a positive potential for FISH in detecting disease with poor clinical prognosis.
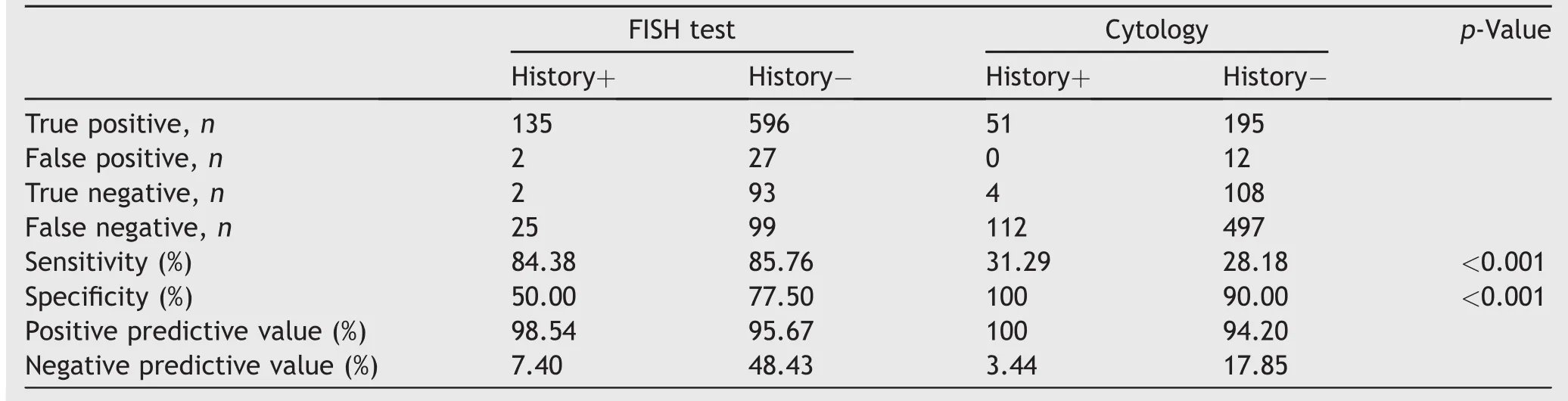
Table 4 The sensitivity of the FISH test in patients with or without a history of transitional cell cancer(n=979).
As shown in our results,we found no difference between the detection of BC in patients with or without a previous BC history.A surveillance protocol based on FISH results has been suggested for patients with BC,and cystoscopy is mandatory for patients with a positive FISH result.In the case of negative endoscopic findings,the high risk of tumor recurrence during the following months makes repeat follow-up cystoscopy necessary.For patients with negative FISH results,the undetected presence of an invasive BC is very improbable,and only some super ficial to low grade tumors may go undiagnosed;as a result,it could decrease or even eliminate the need for periodic cystoscopy until FISH-positivity is found.Our recent study agrees with the fact that most invasive diseases are unlikely to be missed,but the feasibility of this approach remains to be proven.
Currently,FISH detection of BC has been shown to have a higher sensitivity than cytology,and the Food and Drug Administration has also approved it as a diagnostic method for BC.Based on these results,the China Food and Drug Administration has adopted and approved FISH to detect BC.For FISH detection of BC,the current cost is expensive compared with urine cytology;however,this technology will be widely accepted in developing countries,such as China,if the cost of FISH testing can be reduced.
Our research also has some limitations,including that the sensitivity of cytology was lower than that previously reported.Additionally,a long-term study is still needed to determine the value of FISH in the surveillance of BC.
5.Conclusion
The FISH test provided better diagnostic value for bladder transitional cell carcinoma detection compared to cytology in patients with or without BC history in our series.The sensitivity of FISH is greater in high grade and muscle invasive disease than it is in low grade or non-muscle-invasive disease.
Author contributions
Liqun Zhou was involved in protocol/project development,data collection and management,drafting the manuscript and data analysis.Yi Ding was involved in data collection and management and revision of the manuscript.Xuesong Li was involved in protocol/project development,revision of the manuscript and supervision.Kaiwei Yang was involved in data collection and management,drafting the manuscript and data analysis.The remaining authors all were involved in data collection.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgments
This clinical research was funded by the Ministry of Health People’s Republic of China(No.WKJ2007-3-001).
 Asian Journal of Urology2019年1期
Asian Journal of Urology2019年1期
- Asian Journal of Urology的其它文章
- Detection of androgen receptor(AR)and AR-V7 in small cell prostate carcinoma:Diagnostic and therapeutic implications
- Albumin-linked prostate-specific antigen-activated thapsigargin-and niclosamide-based molecular grenades targeting the microenvironment in metastatic castration-resistant prostate cancer
- Prostate tumor neuroendocrine differentiation via EMT:The road less traveled
- Regulatory signaling network in the tumor microenvironment of prostate cancer bone and visceral organ metastases and the development of novel therapeutics
- Combination therapy with androgen deprivation for hormone sensitive prostate cancer:A new frontier
- Potential impact of combined inhibition of 3α-oxidoreductases and 5α-reductases on prostate cancer