
Endoscopic pedicle flap grafting in the treatment of esophageal fistulas: A case report
2020-06-17 05:54YuHangZhangJiangDuChuanHuiLiBingHu
World Journal of Clinical Cases 2020年11期
Yu-Hang Zhang, Jiang Du, Chuan-Hui Li, Bing Hu
Yu-Hang Zhang, Jiang Du, Chuan-Hui Li, Bing Hu, Department of Gastroenterology, West China Hospital, Sichuan University, Chengdu 610041, Sichuan Province, China
Abstract
Key words: Diverticulum; Esophageal fistula; Endoscopy; Pedicle grafting; Case report
INTRODUCTION
The esophageal diverticulum is a rare disorder, which is usually asymptomatic and does not require treatment. Fistulization is a rare complication of esophageal diverticula[1], which often requires surgery that can be invasive and traumatic. In addition, because the diverticulum is a cavity protruding outward from the esophageal lumen, it might not be appropriate to use a stent as treatment.
干預(yù)前兩組生命體征循環(huán)指標(biāo)相近,P>0.05;干預(yù)后觀察組生命體征循環(huán)指標(biāo)優(yōu)于對(duì)照組,P<0.05。如表2.
Flap transplantation has been widely used in plastic surgery for treating various skin defects, chronic ulcers, fistulas, or sinus tracts. Pedicle flap is a type of flap attached to the original site that provides blood supply during grafting. Muscle or omental flaps have been reported to be used in surgical repair of esophageal leakage and fistula[2,3]. Hochbergeret al[4]endoscopically transplanted a gastric mucosal flap to prevent esophageal stricture after endoscopic submucosal dissection of early squamous cell carcinoma. Inspired by that study, we hypothesized that the mucosal flap could help induce the closing of esophageal fistula when surgery is contraindicated. Therefore, we improved this mucosal transplantation method by using pedicle esophageal mucosal flap to close mediastinal esophageal fistulas.
CASE PRESENTATION
Chief complaints
A 49-year-old man was admitted to our hospital complaining of reiterative backache,occasional bloody sputum, and choking when eating or drinking.
History of present illness
Symptoms of backache and bloody sputum started 7 years ago. The pain was located in the scapular region. Consequently, the patient was diagnosed with chronic bronchopneumonia and was treated accordingly. Ten months ago, he experienced choking during eating or drinking. Recently, the aforementioned symptoms became aggravated and were followed by a low-grade fever.
History of past illness
The patient had a history of an esophageal diverticulum 10 years ago.
Comorbidity
The patient had concomitant mild depression and was taking Olanzapine 2.5 mg qd.
Physical examination
Upon admission, the patient’s temperature was 37.5 °C, pulse rate was 84 bpm,respiratory rate was 19 breaths per minute, and the blood pressure was 102/62 mmHg. Breath sounds at the right lower pulmonary lobe region were reduced, and fine rales could be heard.
Laboratory examinations
Blood analysis revealed that white blood count was 4.49 × 109/L with a neutrophil percentage of 79.3%. The biochemistry test and electrocardiogram were normal.Sputum microbiological cultivation revealed no obvious pathogenic bacteria.
Imaging examinations
Chest computed tomography showed dilation of the lower esophagus and air in the adjacent mediastinum (Figure 1A). Esophagram confirmed the presence of mediastinal esophageal fistula around the 9ththoracic vertebra level (Figure 1B). In addition, esophagogastroduodenoscopy revealed a giant diverticulum of 2.0 cm in diameter at the right post wall, 32-34 cm aborally. Two fistulas (0.5 cm and 0.3 cm in diameter respectively; 33 cm aborally) were confirmed in the cavity of the diverticulum (Figure 1C).
FINAL DIAGNOSIS
The final diagnosis suggested an esophageal fistula secondary to spontaneous rupture of the diverticulum.
INTERVENTIONAL STRATEGY
Based on this diagnosis, surgical resection of the diverticulum or repair of the fistulas was not recommended by the surgeon due to possible side effects related to surgery(uncontrolled mediastinitis or nonhealing of suture wounds) of fistula with chronic infection. In addition, the doctor suggested that a stent should not be applied because it could not seal fistula orifices in the outward protruding diverticulum, and the diverticulum cavity might contain pus. Instead, an endoscopic pedicle flap grafting(EPFG) was recommended and accepted by the patient who signed the informed consent.
TREATMENT
Upon admission, the patient was prescribed cefoxitin 2000 mg ivgtt q12h and parenteral nutrition. EPFG was performed under general anesthesia as follows: (1) An area of about 2.0 cm × 1.0 cm cranially to the fistulas was marked; (2) The salineepinephrine-indigo carmine solution was then injected into the submucosal layer(Figure 1D). Mucosal incision and submucosal dissection were performed (Figure 1E)using a dual knife (Olympus, Tokyo, Japan), leaving the distal edge of the flap (the pedicle, 0.4 cm in diameter) intact; (3) When the pedicle flap was ready (Figure 1F),we applied ablation to the surrounding mucosa of the fistulas using argon plasma coagulation (ERBE, Germany) to make it easier for later attachment (Figure 1G); (4)Rat-tooth forceps were employed to match the free edges of the flap to the ablated mucosa (Figure 1H). Moreover, several titanium clips were used for fixation (Figure 1I) leaving an ulcer area of the original flap (Figure 1J); and (5) Finally, percutaneous endoscopic gastrostomy was performed for future enteral nutrition (Figure 1K).
No procedure-related complications were observed. Ceftriaxone 2000 mg ivgtt qd,esomeprazole 40 mg ivgtt qd, carbazochrome sodium 60 mg ivgtt qd, and enteral nutrition through the percutaneous endoscopic gastrostomy tube were administered after the surgery.
OUTCOME AND FOLLOW-UP
Coughing and backache were relieved, and no fever was observed a week after the surgery. The patient was discharged from the hospital thereafter. Forty-five days after the surgery, endoscopic examination showed that the fistulas were reduced in size.The larger one was reduced from 0.5 cm to 0.2 cm, while the smaller one was fully closed (Figure 1L). We offered the patient a second chance of EPFG, but it was refused. The patient is now considering a surgical option of resecting the diverticulum and is waiting for the clearance of the chronic infection so as to be indicated for surgery by feeding through the percutaneous endoscopic gastrostomy tube.
DISCUSSION
Esophageal fistulization is usually caused by trauma, surgery, neoplasm, radiation, or erosion. In this case, it occurred on the basis of diverticulum. Diverticulum, which causes fistula, is rather rare and is often misdiagnosed as a lung infection,bronchiectasis, or pulmonary abscess[5]. Surgery or endoscopic techniques are required to remove or close fistulas from the esophagus[6,7]. Yet, surgical closure or resection can be performed only in cases with small defects and without contamination in the mediastinum[8]. In this case, the patient presented with sputum caused by a local infection in the lung and mediastinum, which excluded surgery.
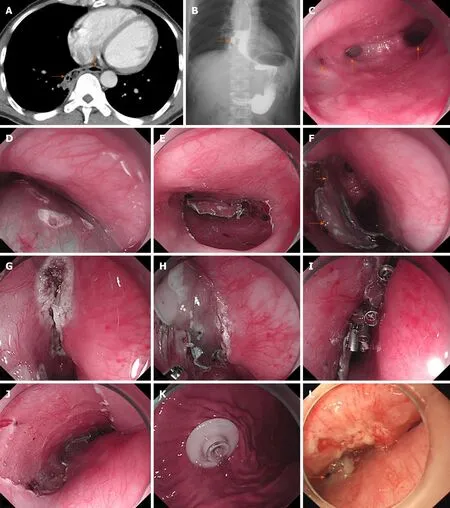
Figure 1 Results of examinations and treatment. A: Computed tomography scan (rightward arrow: Fistula; downward arrow: Esophageal lumen); B: Esophagram revealed the presence of esophageal fistula (arrow) around the 9th vertebra level; C: Endoscopic examination confirmed the presence of two fistulas, which are 0.3 cm(left arrow) and 0.5 cm (middle arrow) in diameter and the esophageal lumen (right arrow); D and E: Submucosal injection was followed by (E) endoscopic submucosal dissection; F: The mucosal flap (lower arrow) with the caudal edge reserved as the pedicle (upper arrow) was made ready after endoscopic submucosal dissection; G and H: Ablation of the surrounding mucosa before (H) covering the fistulas with the flap; I: Several titanium clips were used for fixation; J: Ulcer area left after endoscopic submucosal dissection; K: Percutaneous gastrostomy; L: Forty-five days after the endoscopic surgery, the larger fistula (arrow) reduced from 0.5 cm to 0.2 cm and the smaller one was closed.
For benign esophageal fistulas, nonsurgical treatment like endoscopic stent placement has similar outcomes compared with surgical modality[9]. Nevertheless,this type of treatment has shown to be effective in only 45% of cases and mainly for patients with punctiform orifices (less than approximately 2.5 mm)[10]. Therefore, the size of the orifices might be slightly larger in our case. In addition, the diverticulum cavity is protruding outward, which makes it difficult for the stent to cover the orifice.In that case, the cavity would become a container for pus, which might induce further inflammation if surgery was performed.
Endoscopic cell sheets and free mucosal flap transplantation have been reported to prevent strictures secondary to endoscopic submucosal dissection[11,12]. On this basis,we hypothesized that a pedicle flap with sufficient blood supply than mere free mucosa would endure longer and exhibit greater potential to close the fistula,reserving the integrity of the esophagus. We chose an adjacent esophageal pedicle flap other than skin or previously reported gastric mucosa because skin could not maintain long-term esophageal function and often develops morphological changes,while gastric mucosa has acid-secreting capability[13].
Although the larger fistula was not completely closed, the reduction in size suggested that this new approach was effective in treating esophageal fistula. Possible reasons for the incomplete closure may be that the course of the disease was too long and that local infection and inflammation impeded epithelization. In view of this, we speculate that selected cases with smaller fistula and little contamination may be better candidates for flap grafting. Nevertheless, future studies with more cases are needed to validate its efficacy and identify best candidates. Comparative studies involving EPFG, stent, and surgical repair using muscle flap are also needed in the future to demonstrate the advantage and disadvantage of each modality. Perhaps a combination of EPFG and stent might also be a choice.
CONCLUSION
Considering the fistula’s anatomic and physiologic traits, accessibility, and minimally invasive nature, pedicle flap grafting under endoscopy might be a better choice for esophageal fistula. In addition, it exhibits potential to be applied in esophageal fistulas without diverticulum, and its combination with stent could be considered as well. Future studies are needed to explore its clinical applicability.
猜你喜歡
債券(2020年4期)2020-08-04
計(jì)算機(jī)應(yīng)用(2018年12期)2019-01-08
商周刊(2018年26期)2018-12-29
債券(2018年11期)2018-02-21
電子技術(shù)與軟件工程(2017年3期)2017-03-22
爆笑show(2016年2期)2016-04-11
醫(yī)學(xué)信息(2015年5期)2015-03-31
醫(yī)學(xué)信息(2015年7期)2015-03-20
 World Journal of Clinical Cases2020年11期
World Journal of Clinical Cases2020年11期
- World Journal of Clinical Cases的其它文章
- Tumor circulome in the liquid biopsies for digestive tract cancer diagnosis and prognosis
- Isoflavones and inflammatory bowel disease
- Cytapheresis for pyoderma gangrenosum associated with inflammatory bowel disease: A review of current status
- Altered physiology of mesenchymal stem cells in the pathogenesis of adolescent idiopathic scoliosis
- Association between liver targeted antiviral therapy in colorectal cancer and survival benefits: An appraisal
- Peroral endoscopic myotomy for management of gastrointestinal motility disorder